




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
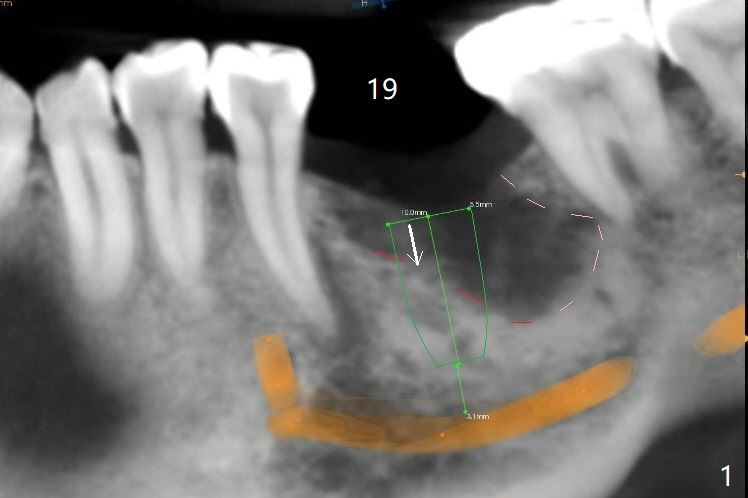
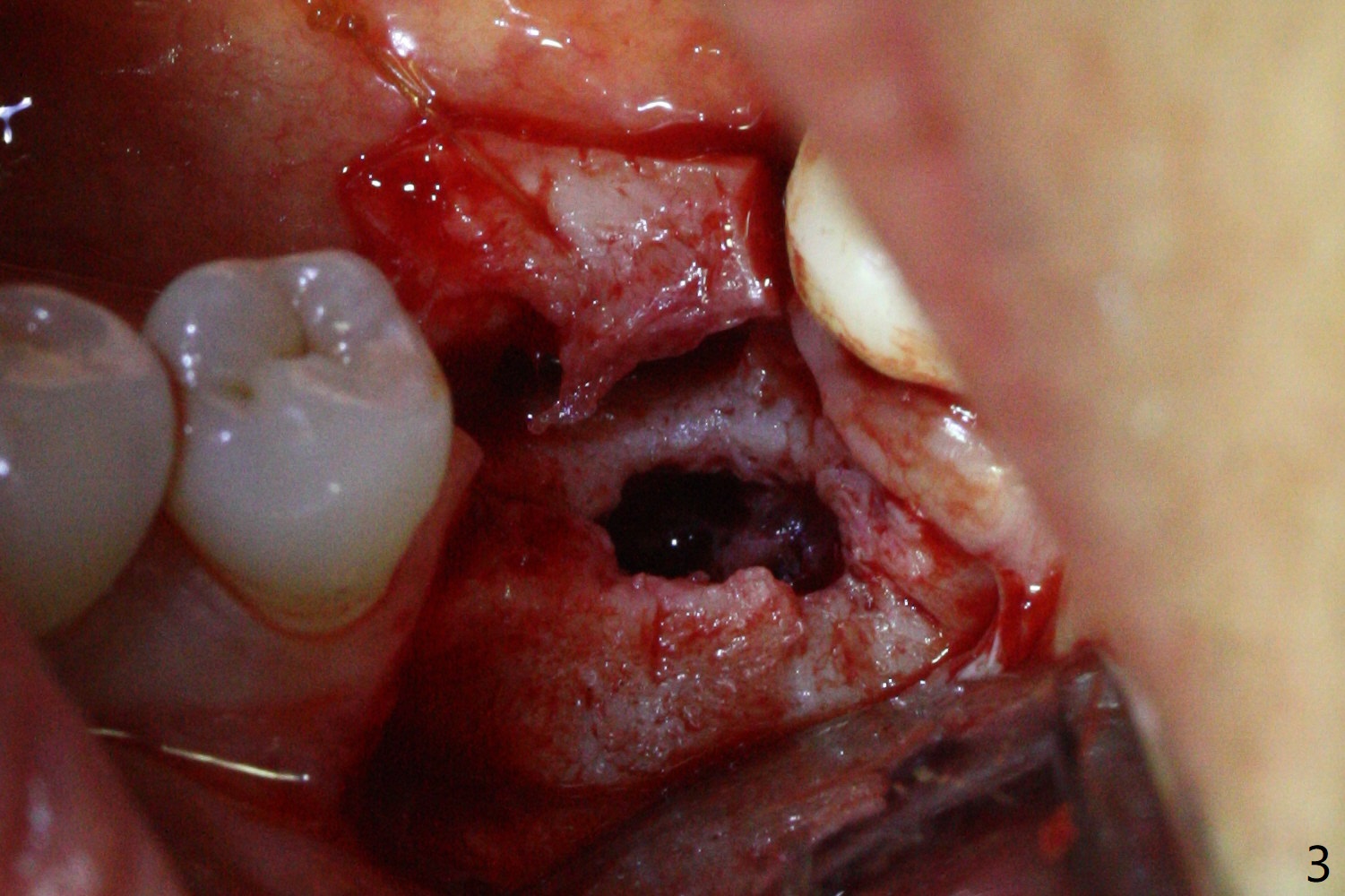
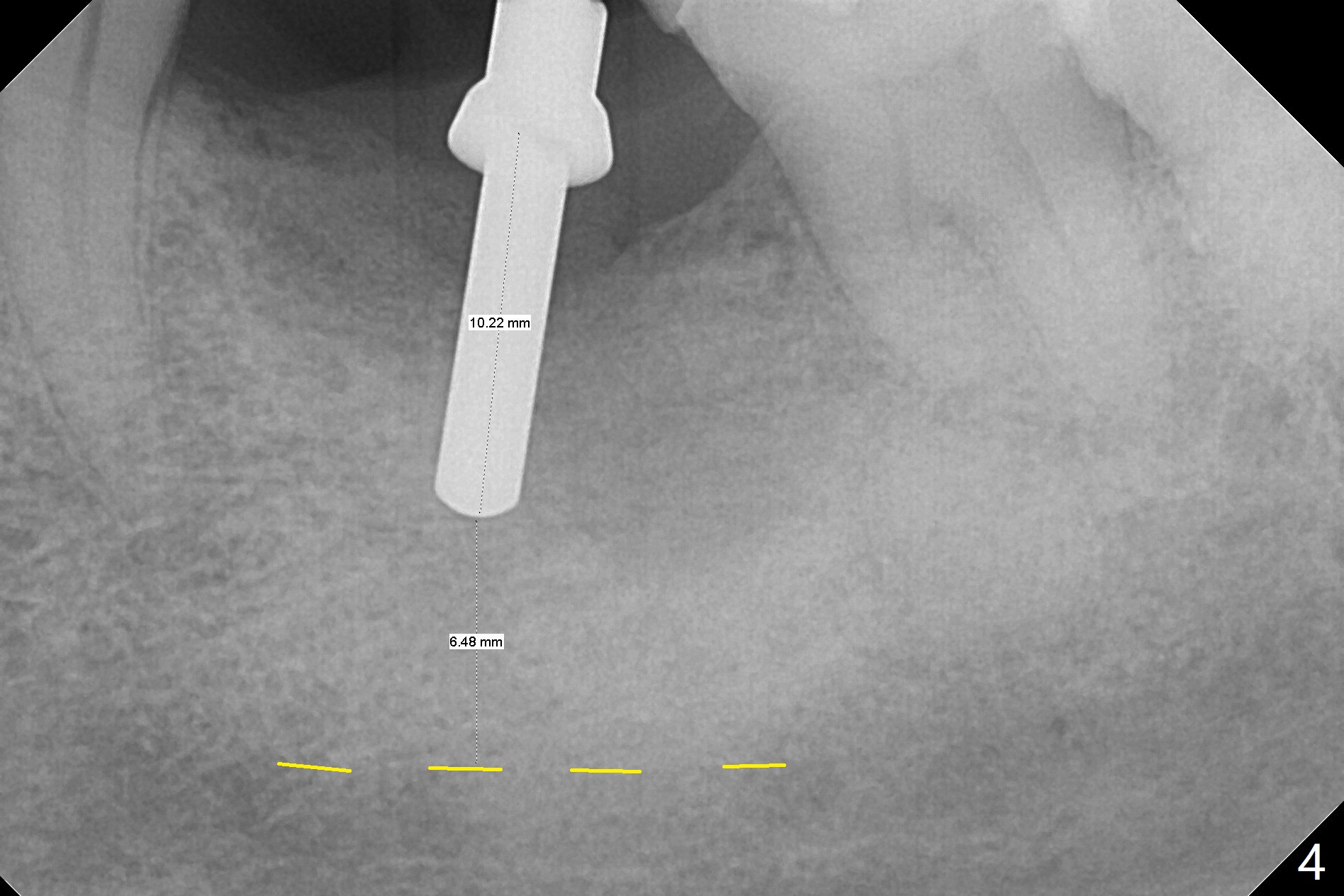
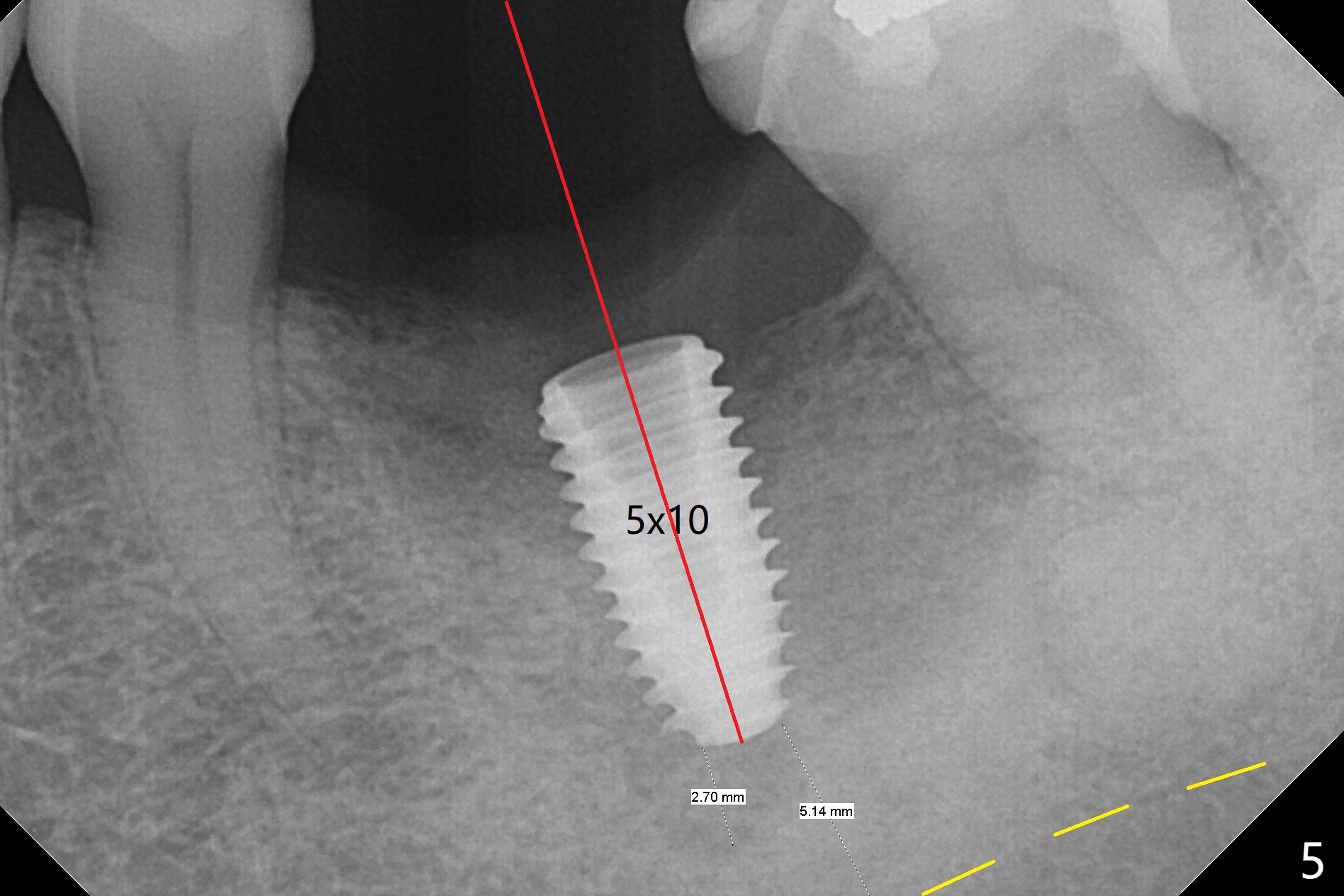
Unhealed Socket
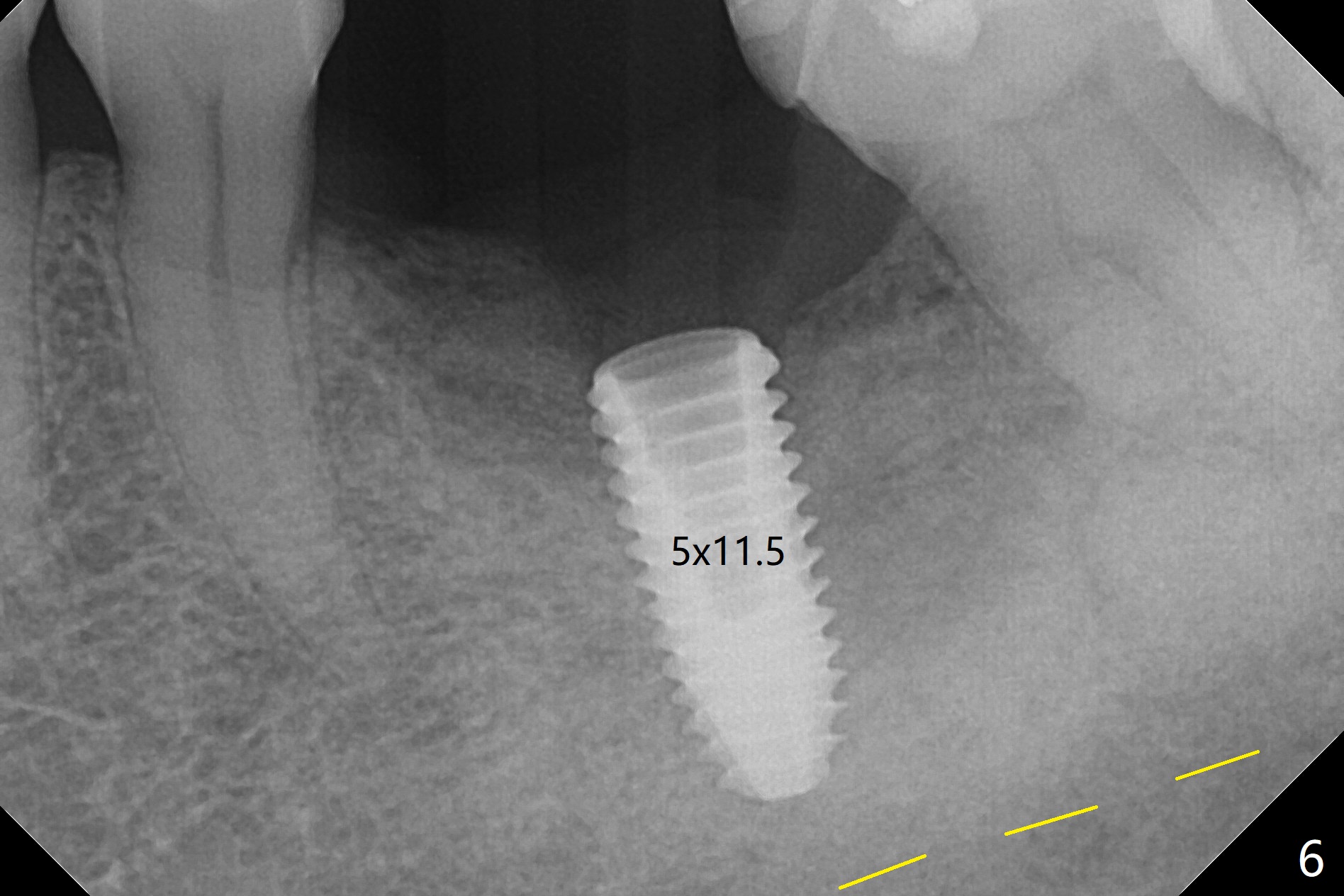
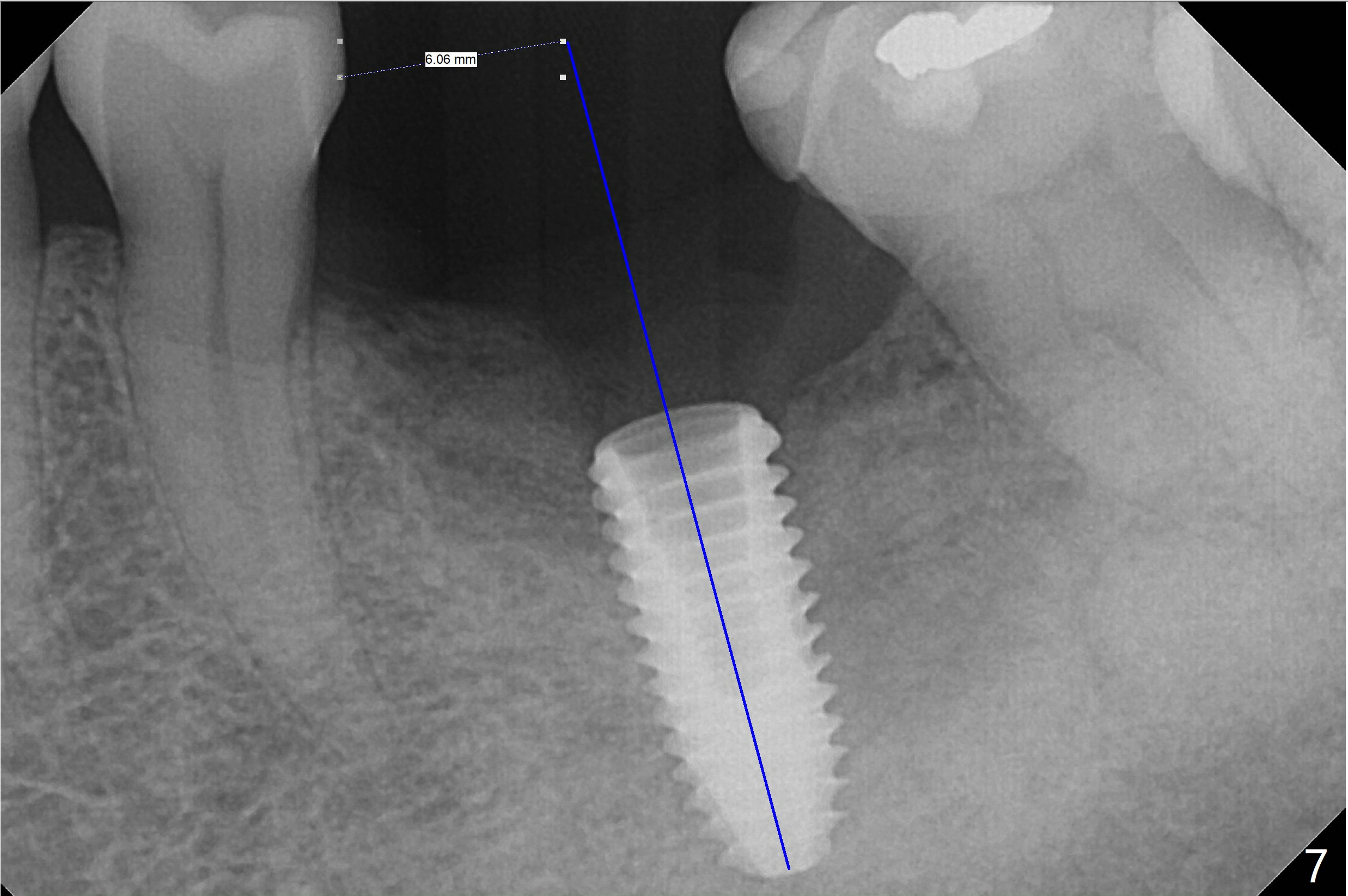
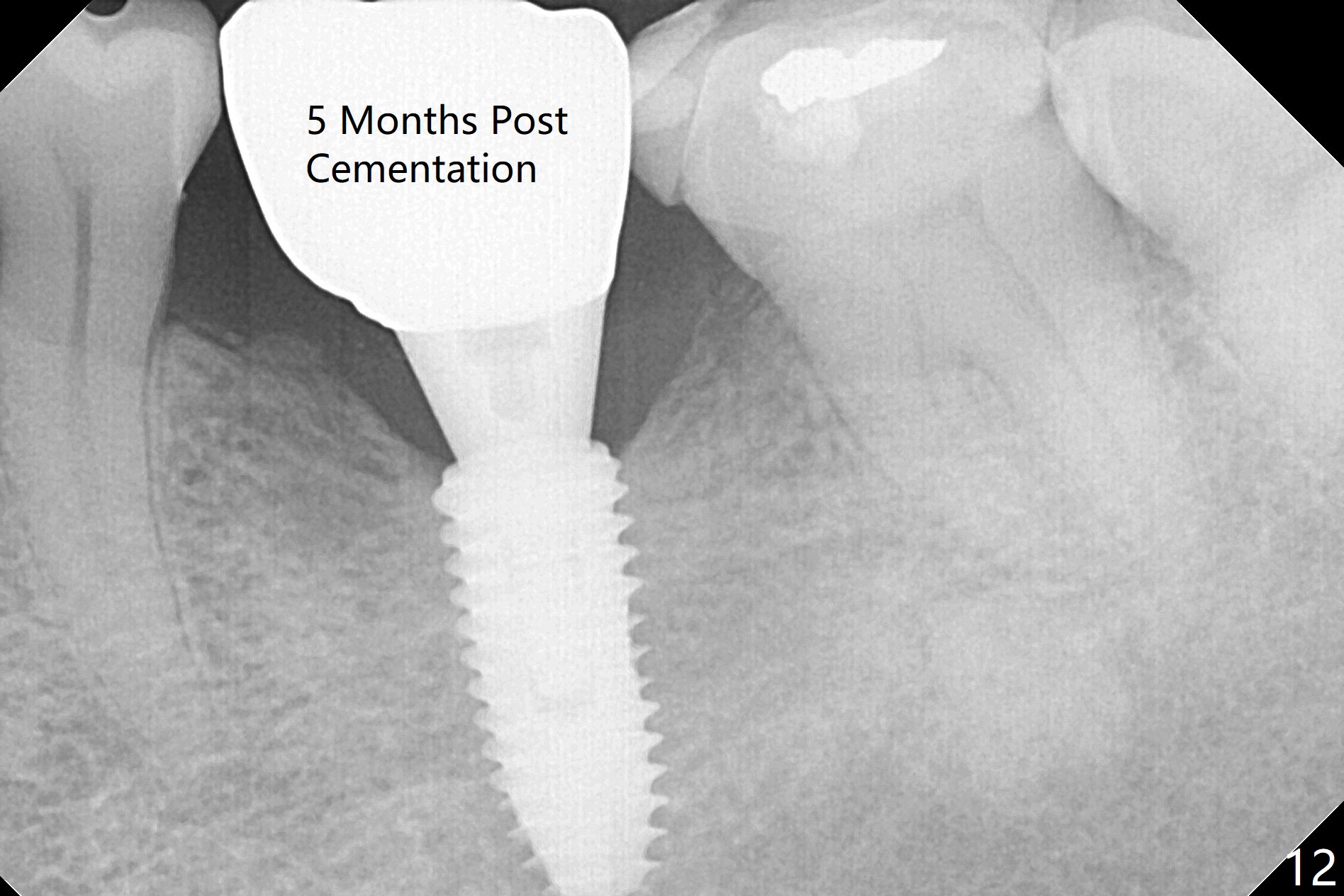
CT taken 4-5 months post extraction shows the outline of the socket at #19 (Fig.1 pink and red dashed line). By the time of surgery (6-7 months post extraction), the ridge looks narrow (Fig.2). In fact the socket does not heal (Fig.3). Osteotomy starts at the mesial border of the socket (Fig.4). When a 5x10 mm dummy implant is placed, the axis begins to be tilted distally (Fig.5 red line), which is more obvious when a definitive longer implant (5x11.5 mm) is placed (Fig.6,7). Osteotomy (Fig.1 arrow) at the mesial slope of the socket (red dashed line) should be initiated more mesial to compensate for the distal drifting while osteotomy is being increased and the implant is being placed. The distal defect is filled with Vanilla graft. Probably due to the mesial slope and the distal defect, the primary stability is <10 Ncm. A healing screw is placed with Vanilla allograft/autogenous bone. The bone forms coronal to the implant 4 months postop (Fig.8 *), which is removed for uncover. The mesial gingival embrasure of the permanent crown is large (Fig.9 *), as related to the mesial undercut associated with a 5.7x4 mm A 15 degree angled abutment (Fig.10). Reduction in the undercut should be able to help lab decrease the gingival embrasure (Fig.11 red line). The bone density around the implant increases with distinct trabecular pattern consistent with stress 5 months post cementation (1 year postop, Fig.12).
Return to
Lower
Molar Immediate Implant,
Armaments
Xin Wei, DDS, PhD, MS 1st edition 03/06/2018, last revision 03/05/2019