

,%20Vera,%20M%20Osteogen%20plug,%20D%20collagen%20plug.jpg)
,%20Vera,%20M%20Osteogen%20plug,%20D%20collagen%20plug,%20IAC.jpg)




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
High Torque, Short Implant, Less Pain
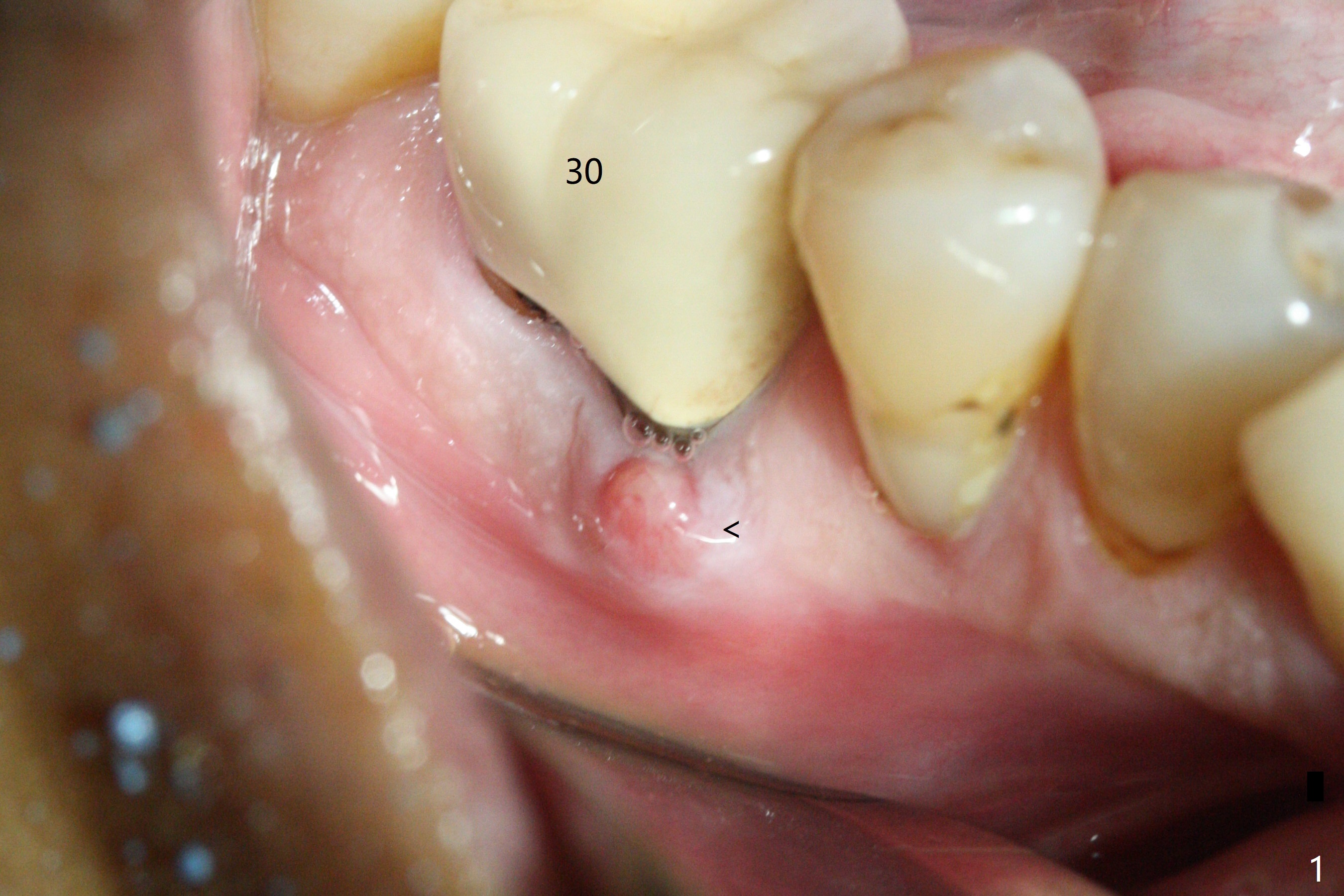
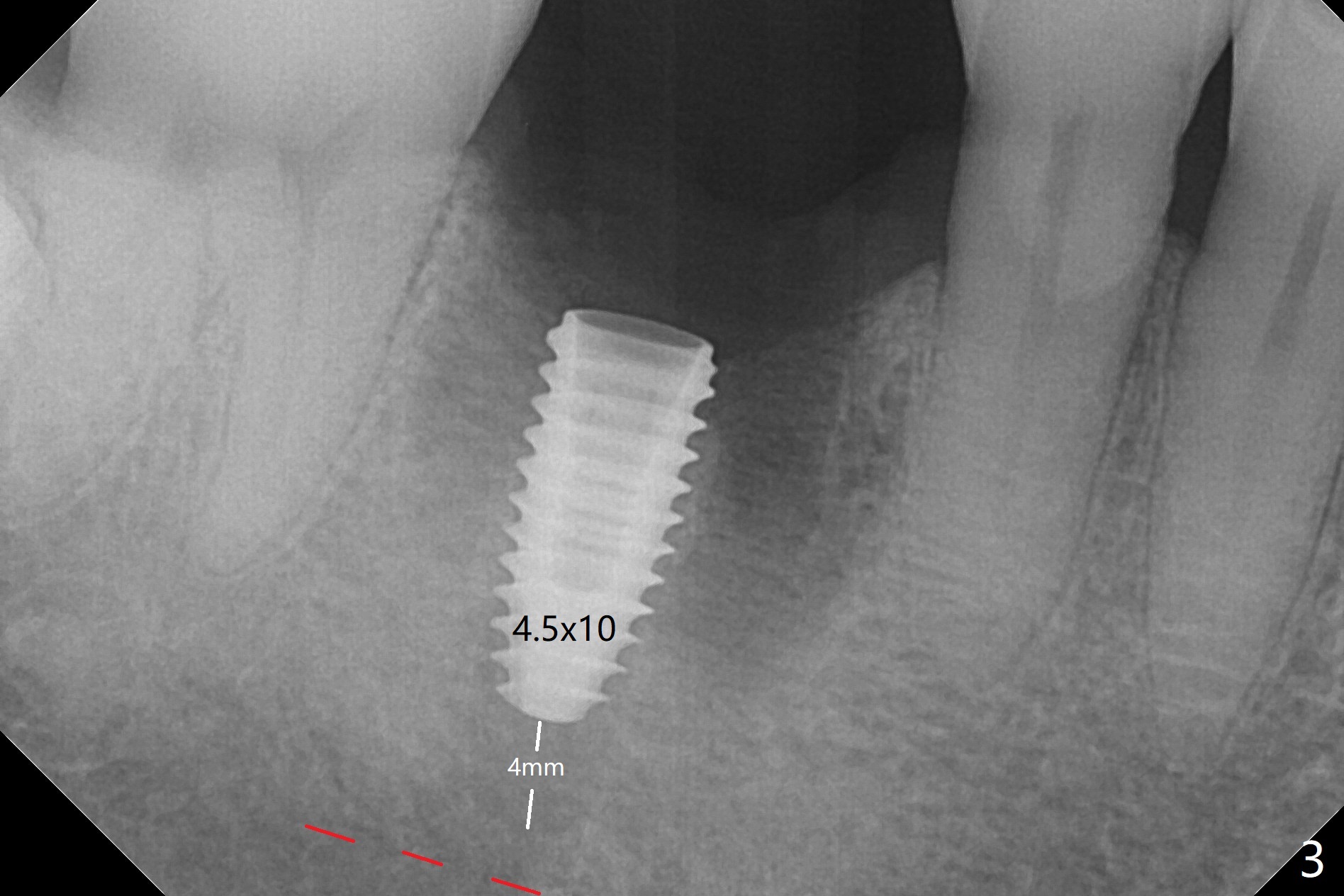
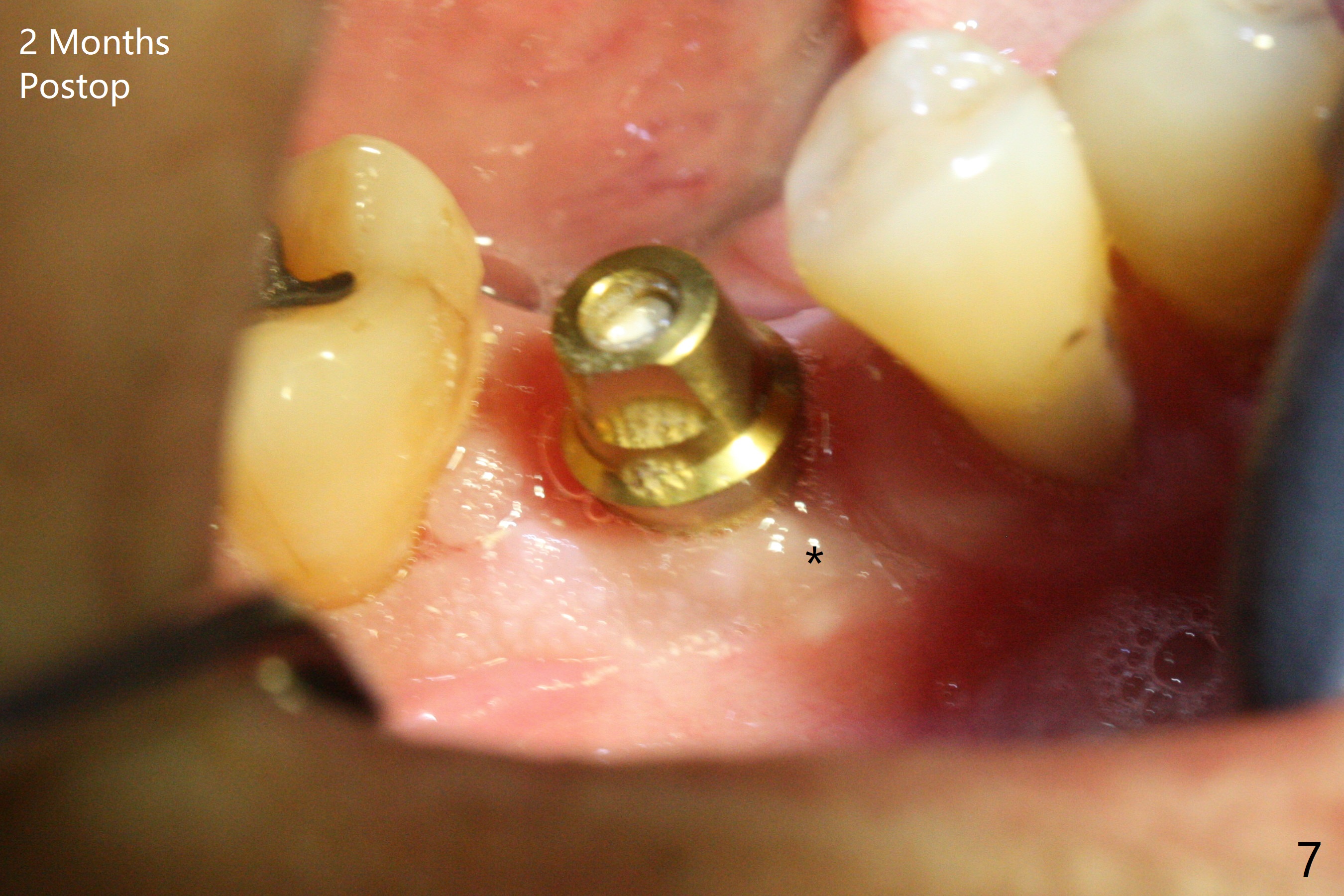
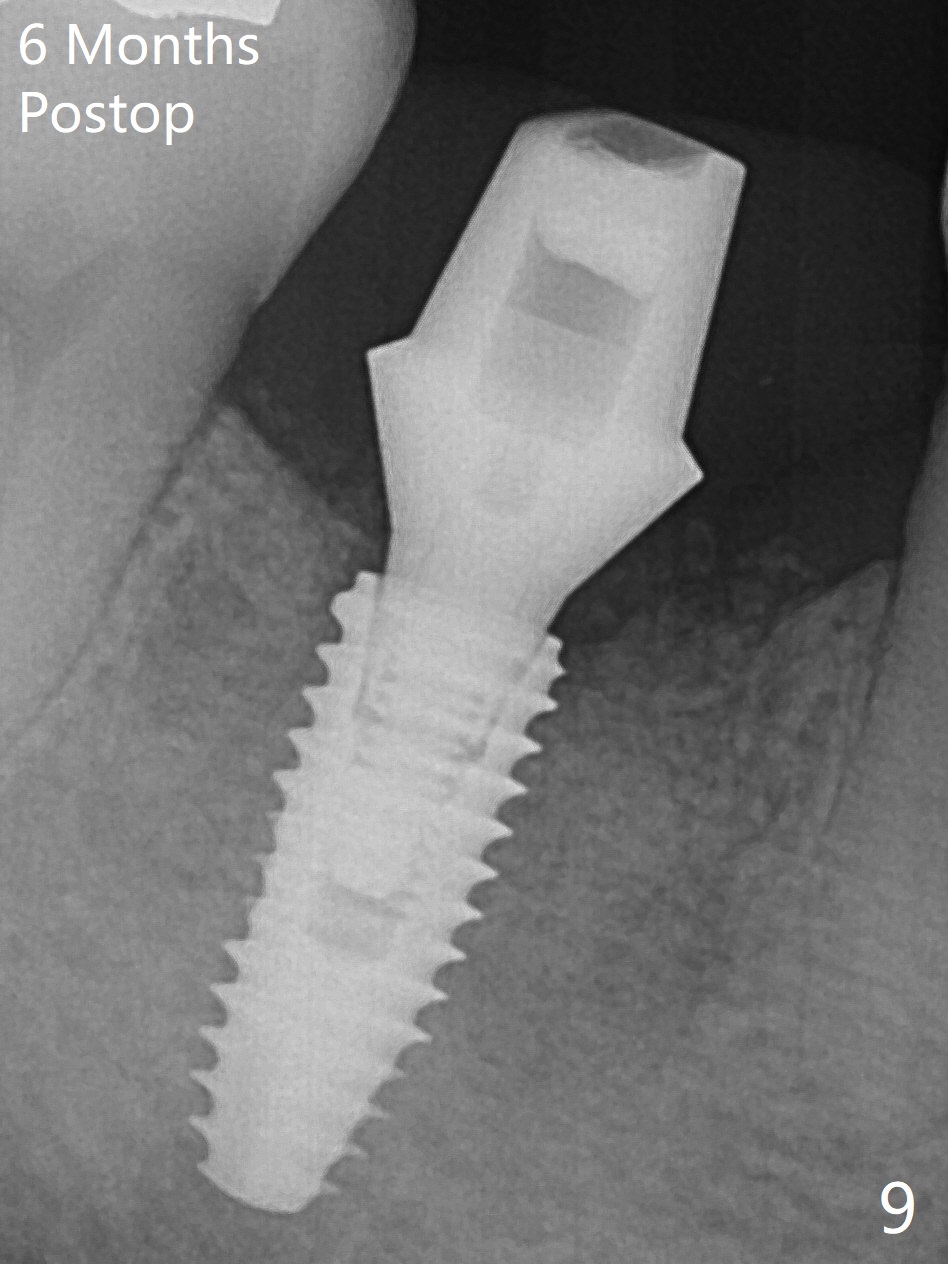
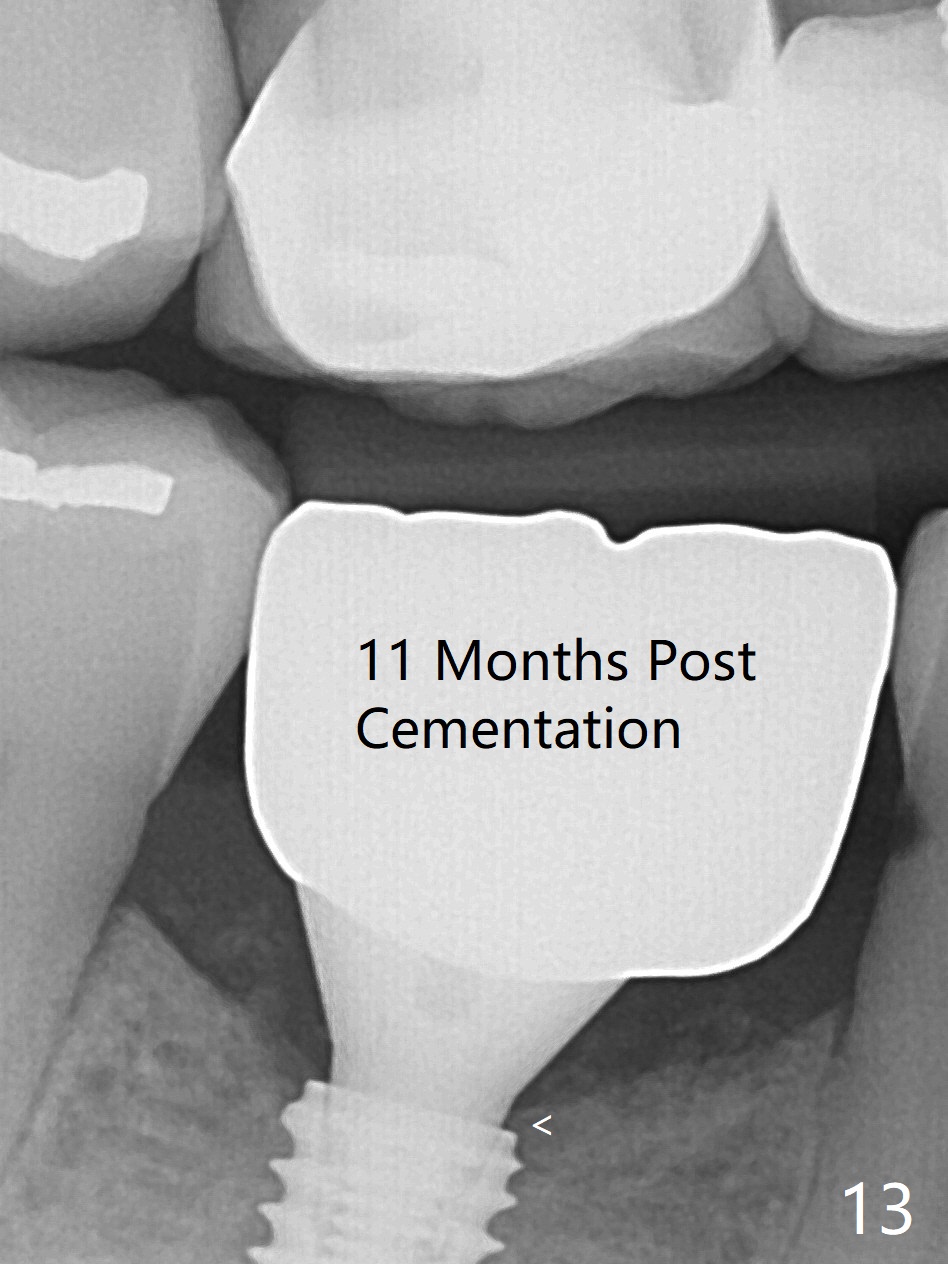
After extraction of the tooth #30, the mesiobuccal plate is found to be lost, corresponding to the fistula (Fig.1 <). Osteotomy is initiated in the flattened septum (lingual) for 13 mm (Fig.2). The patient feels pain when larger drills are being used. Marcaine has to be injected in an infiltration manner for pain control. When a 4.5x10 mm dummy implant is inserted with 55 Ncm, the end of the osteotomy (Fig.3 white line) is close to the Inferior Alveolar Canal (red dashed line). When a definitive implant (Fig.4: 4.5x11.5 mm) is placed with primary stability, there is an apical space (Fig.5 white double arrows). There is moderate postop pain. A shorter implant (10 mm) should be tried when the bone is dense. It will be associated with less pain. The fistula disappears 7 days postop (Fig.6). Although the patient appreciates that the pain is gone, there is atrophy mesiobuccally 2 months postop (Fig.7 *). The implant seems to be have been placed too buccally (Fig.8). With loss of the buccal plate, the implant should be placed away from it to prevent periimplantitis. The abutment is changed from 6.5x4(4) to 6.5x5.5 (3) mm with fabrication of a new provisional. The buccal margin is still supragingival 6 months postop and prep lower before impression. The mesial and distal sockets appear to have healed (Fig.9). When the crown is cemented, the mesiobuccal papilla is present (Fig.10 *), while the mesiolingual one is apparently absent (Fig.11 *). Using a temporary abutment and relining the provisional multiple times would increase the chance of rebuilding the missing papilla. The bone density around the implant increases 11 months post cementation (Fig.12). The dense (apparently cortical) bone seem to grow over the implant plateau 11 months post cementation (Fig.13 <).
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments Xin Wei, DDS, PhD, MS 1st edition 01/12/2018, last revision 04/20/2019