,%20Vera.jpg)
|
|
|
|
|
|
|
|
|
|
Use of Once-Done Provisional Stabilizes Implant
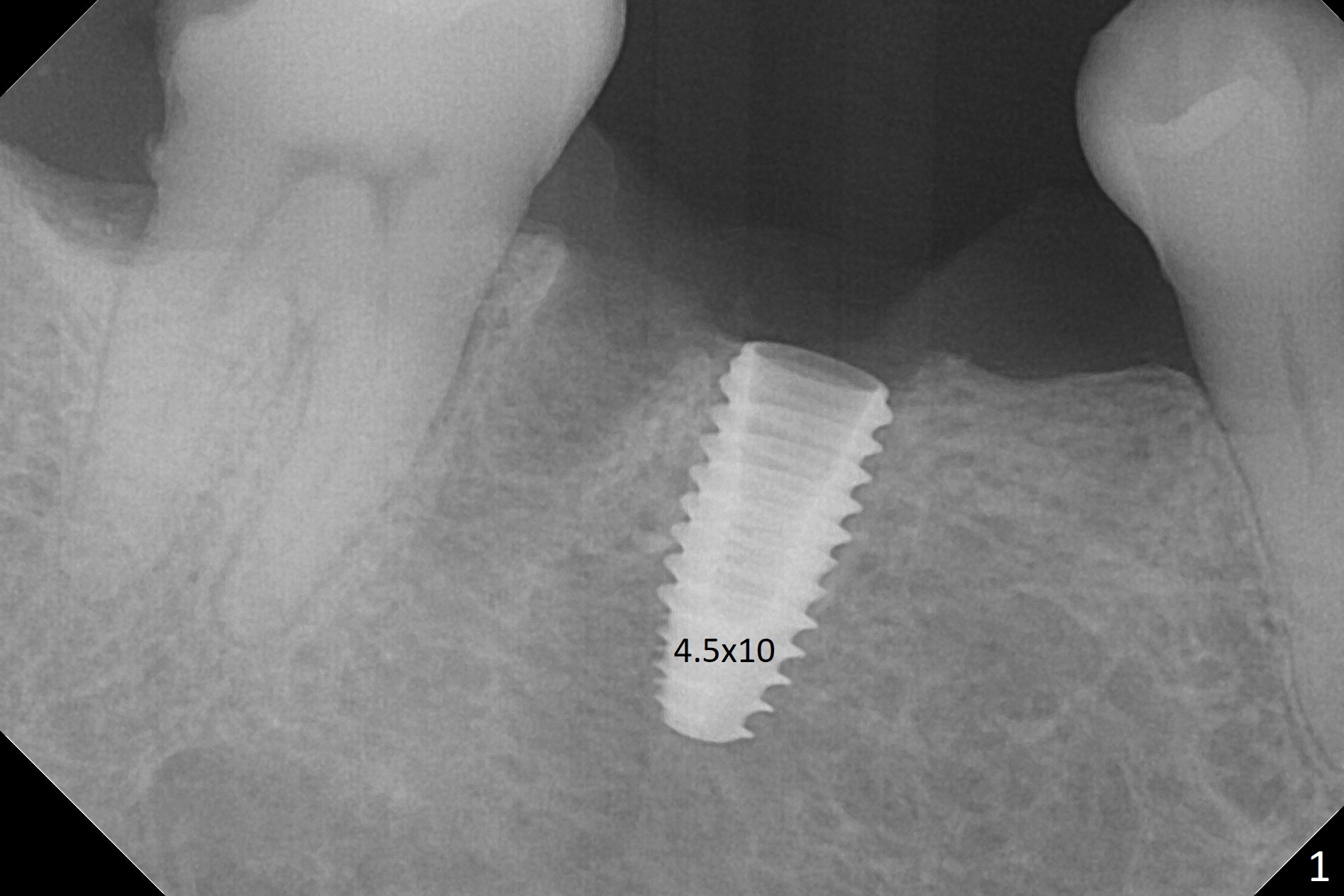
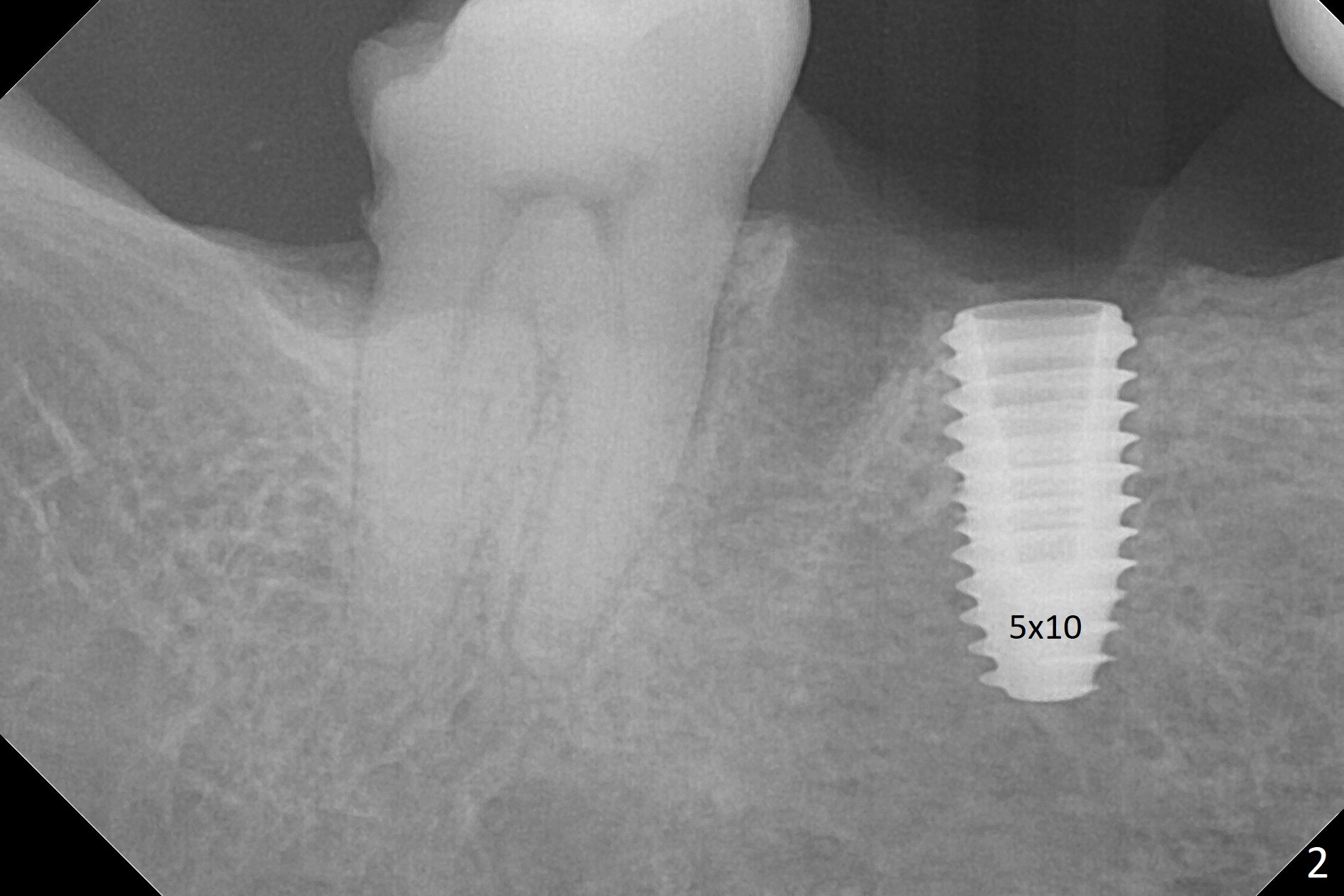
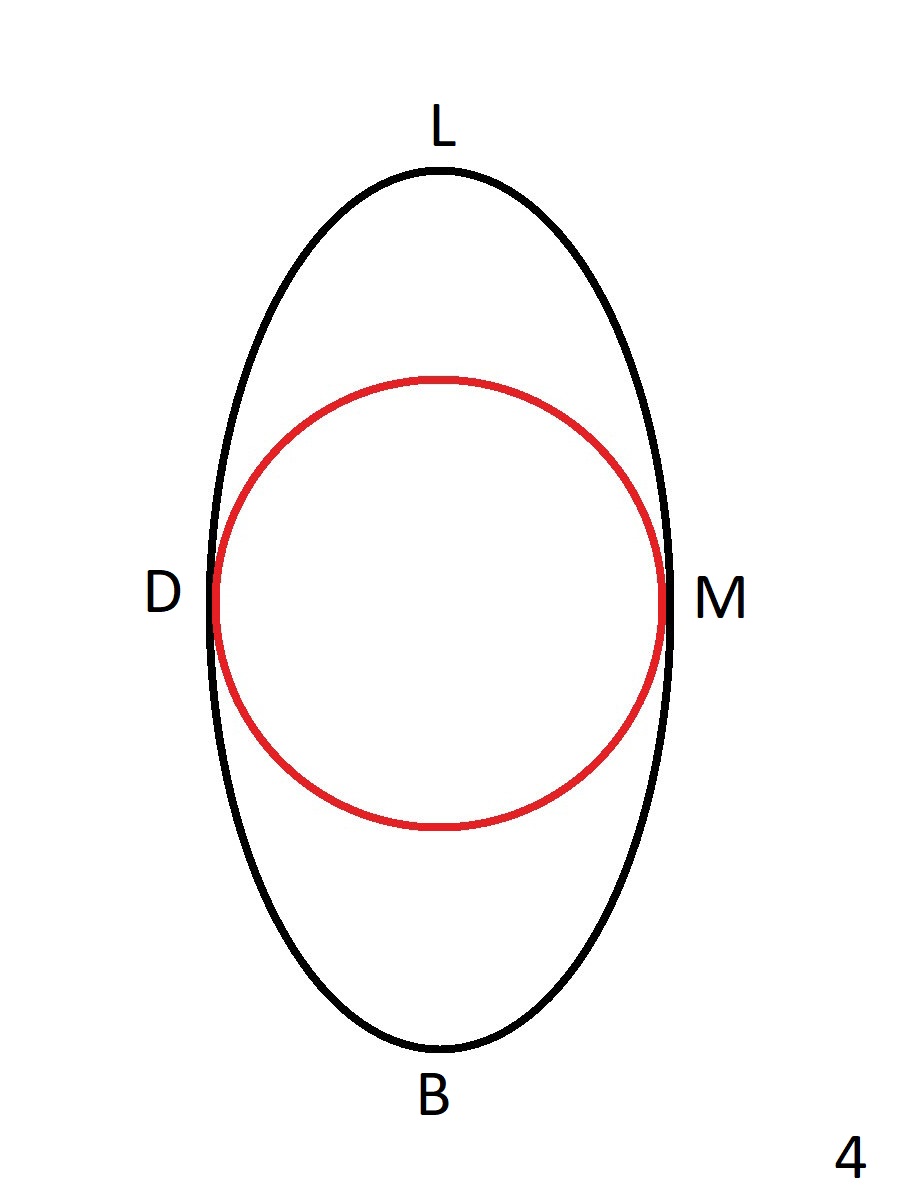
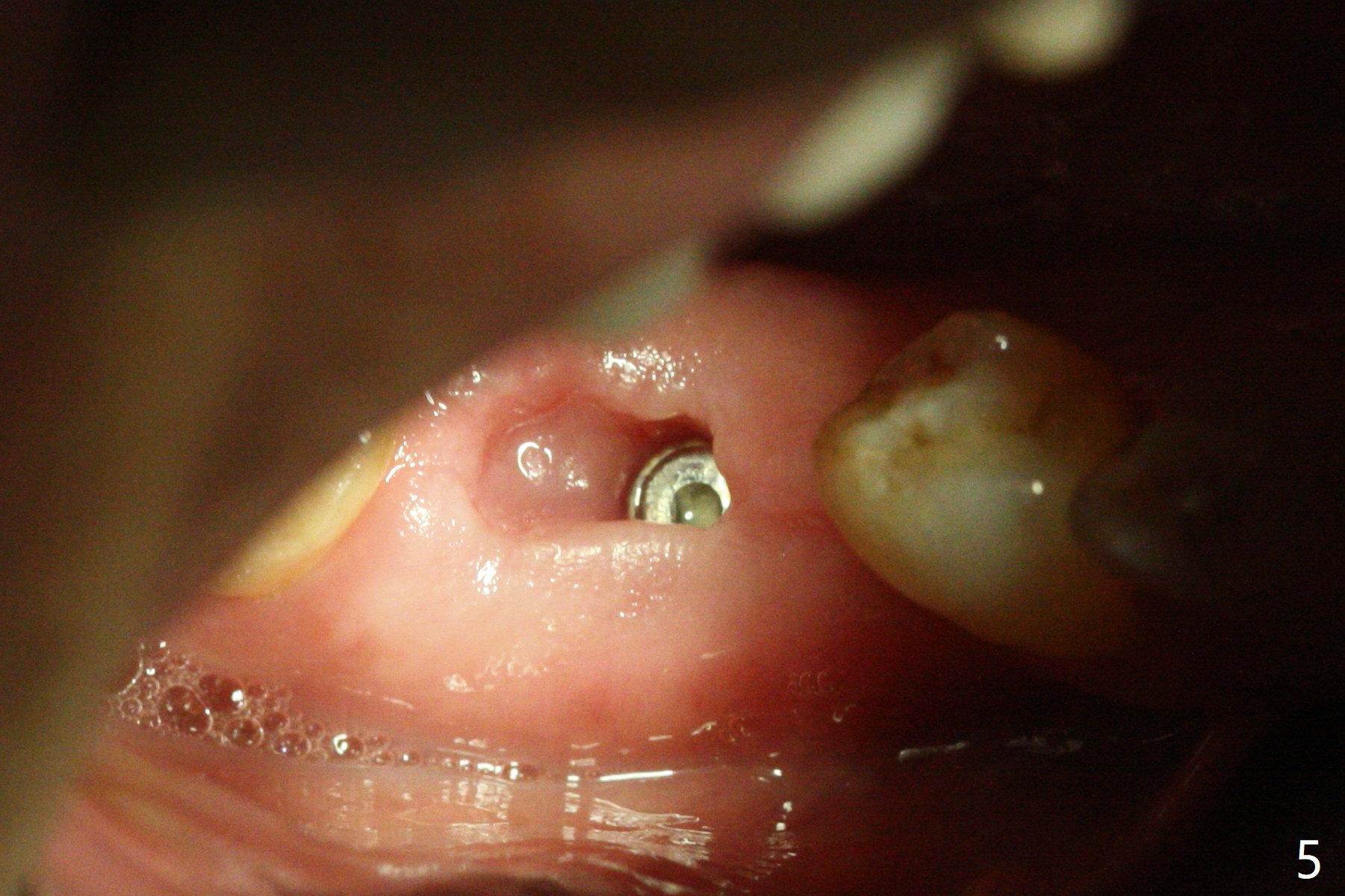
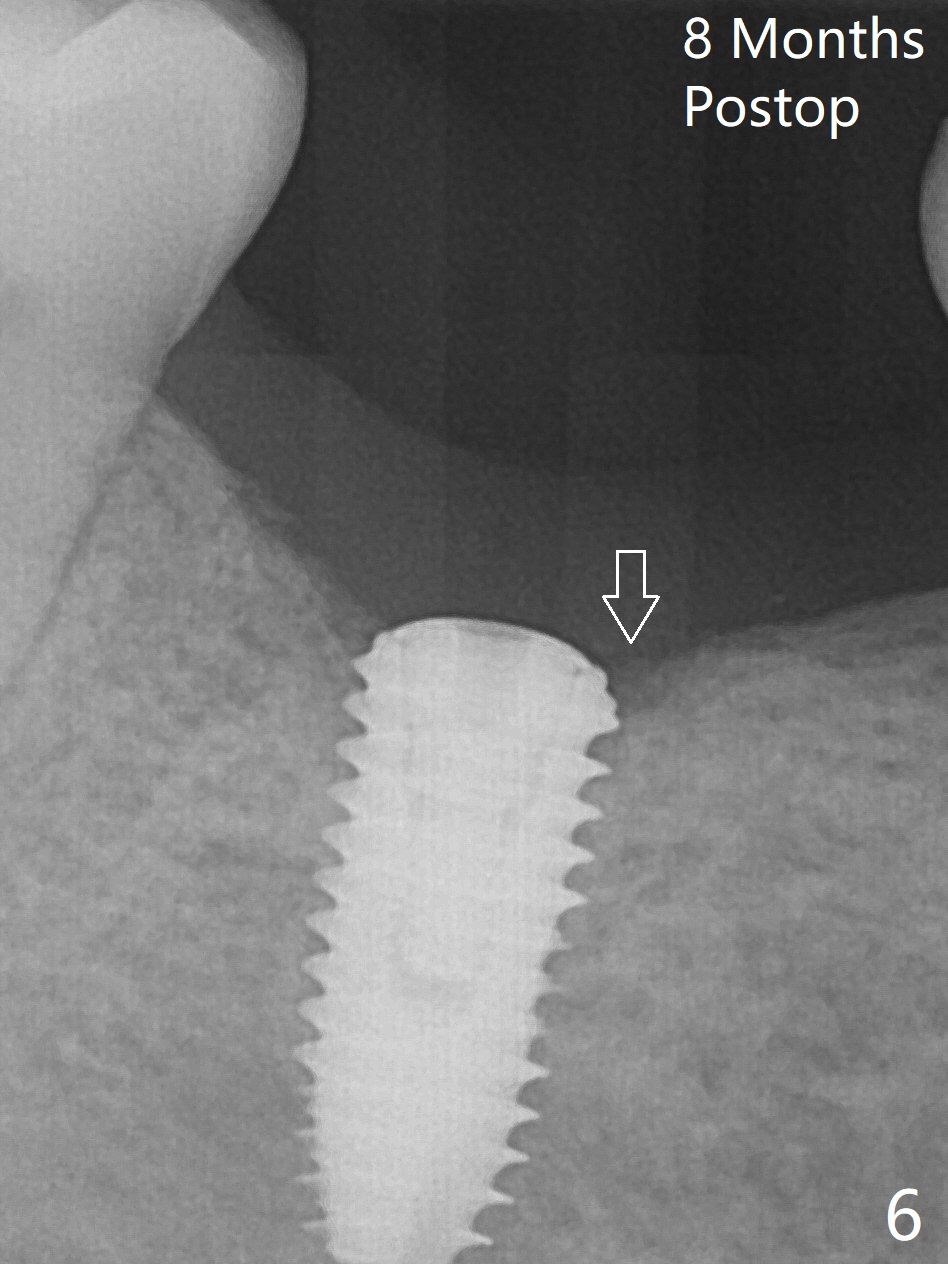
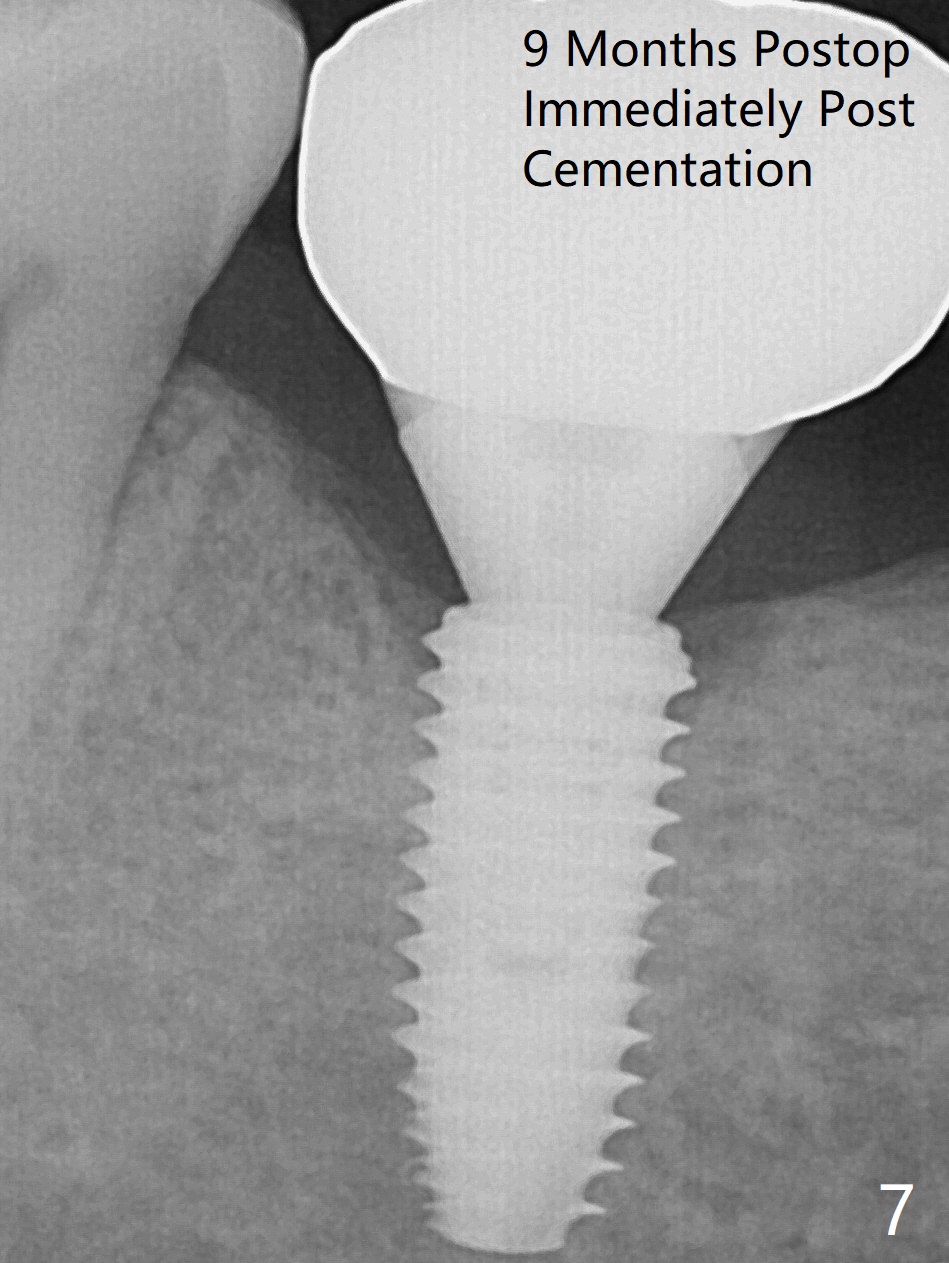
Because of severe pain, block anesthesia is administered prior to extraction. The mesial socket of the tooth #30 is deep with granulation tissue. A 4.5x10 mm dummy implant is placed with < 40 Ncm following sequential osteotomy until 4x13 mm over the septum (Fig.1 (low density)). After 4.5x13 mm drill, a 5x10 mm dummy implant is inserted with <40 Ncm (Fig.2). Since the Inferior Alveolar Canal is invisible (Fig.1,2 (pan should have been taken)), a 5x11.5 mm implant is placed with <20 Ncm. When a 6.5x5.5(3) mm abutment is placed, the underlying implant is turned (Fig.3). With collagen plug is placed in the distal socket and Vera graft around the implant, an immediate provisional is fabricated and relined. When it is seated, it has mobility. In fact the provisional should be locked into the edentulous area while it is malleable. To prevent low primary stability, osteotomy should be under prep, since the implant (red circle) contacts only two bony surfaces, i.e., the mesial (M) and distal (D) walls of the mesial socket (Fig.4 (occlusal view) black oval). There are gaps buccally (B) and lingually (L). In case of low stability, a healing screw or abutment should be placed; the remaining socket is closed with suture. The provisional is loose 19 days postop; it is removed by sectioning. A healing screw is placed. Twelve days later, the wound heals (Fig.5). The patient returns for uncover 8 months postop; although the implant has osteointegrated apparently, the crestal bone resorbs to the implant plateau level (Fig.6 arrow). It seems that the immediate implant should be routinely placed 2-3 mm deeper. The open margin is closed with composite when the abutment/crown is removed after cementation (Fig.7).
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments Xin Wei, DDS, PhD, MS 1st edition 12/27/2017, last revision 09/29/2018