.jpg)
.jpg)
|
|
|
|
|
|
|
|
|
|
||
Use of Profile Drill Twice
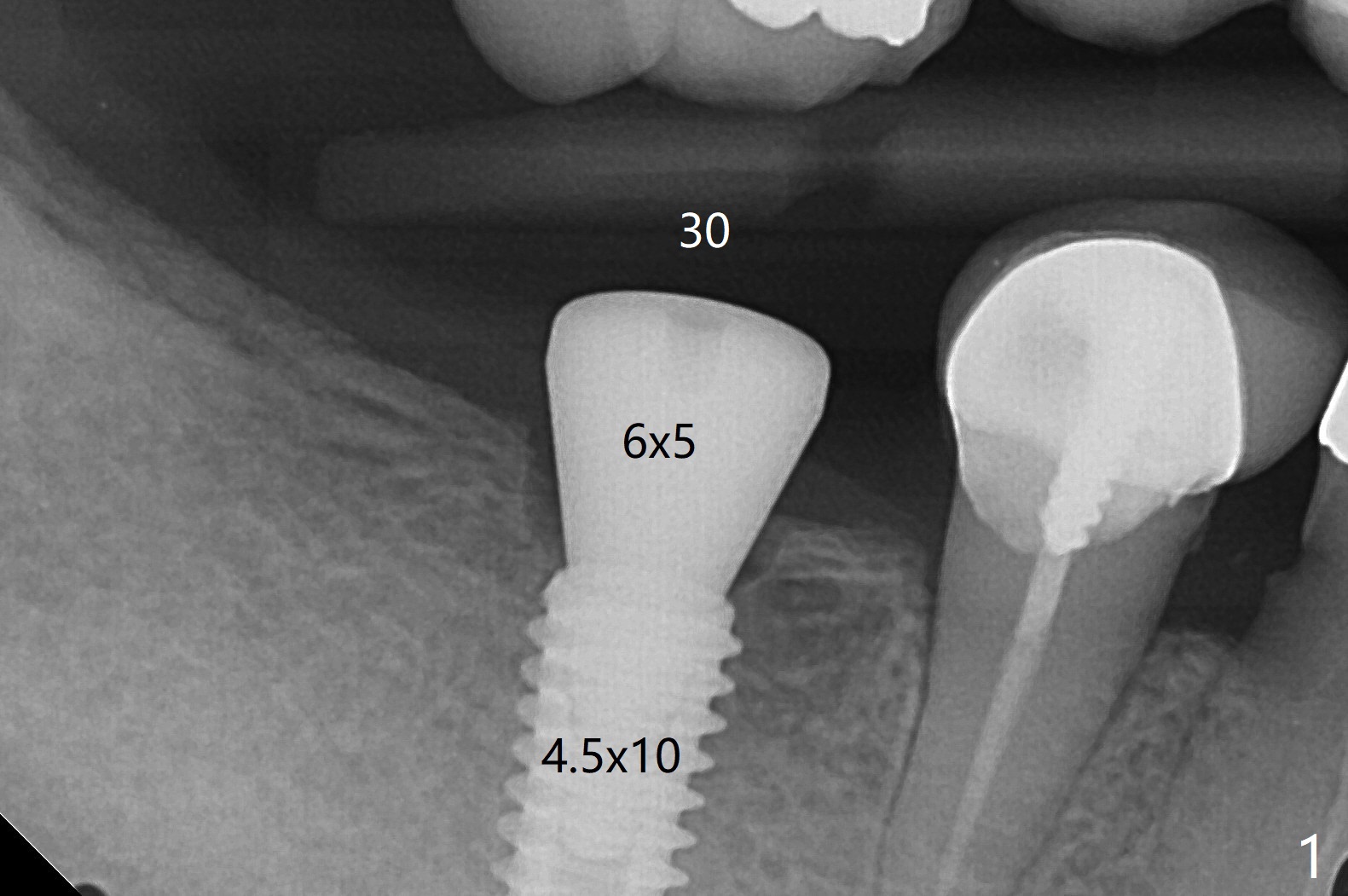
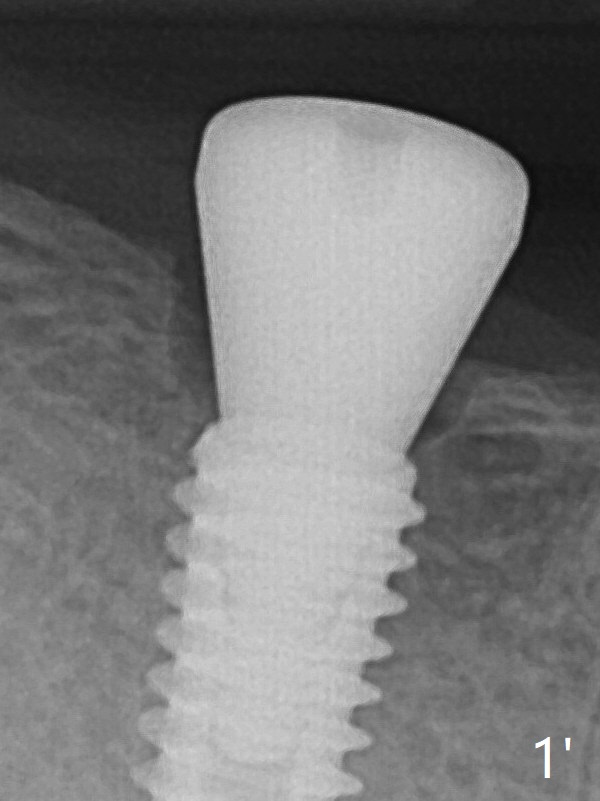
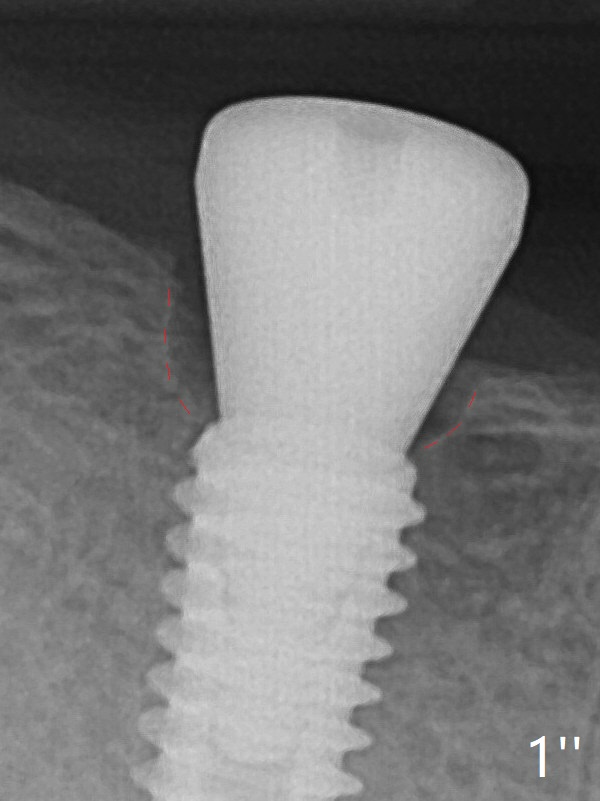
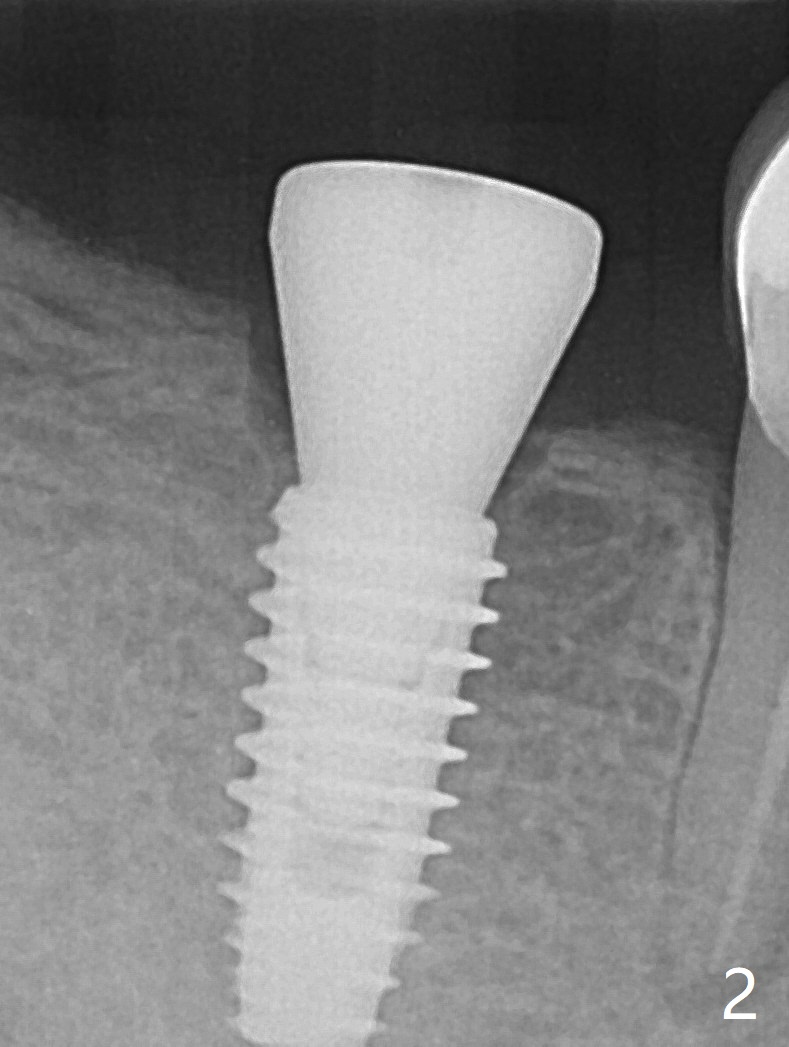
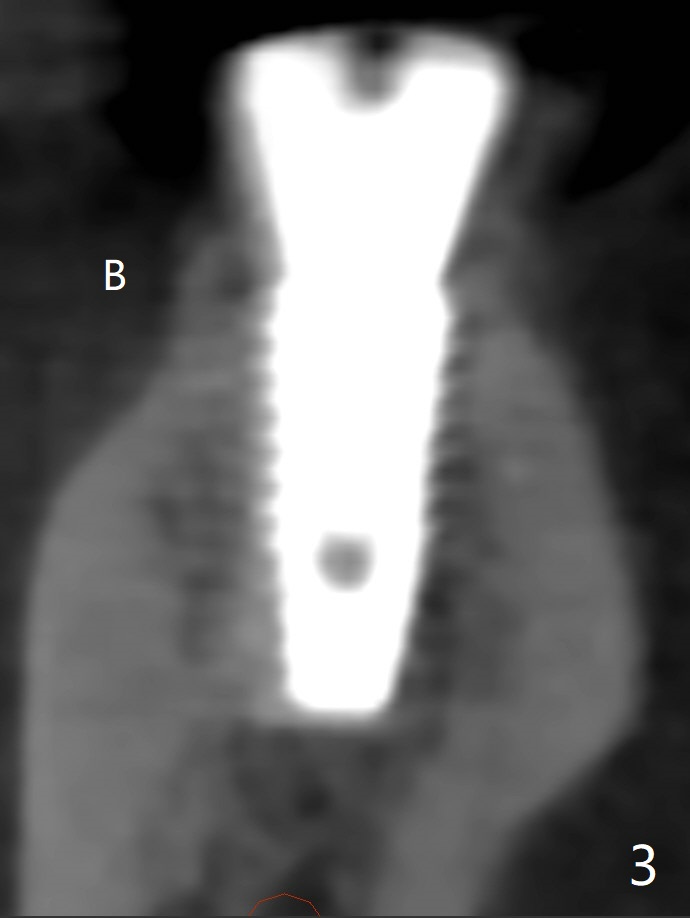
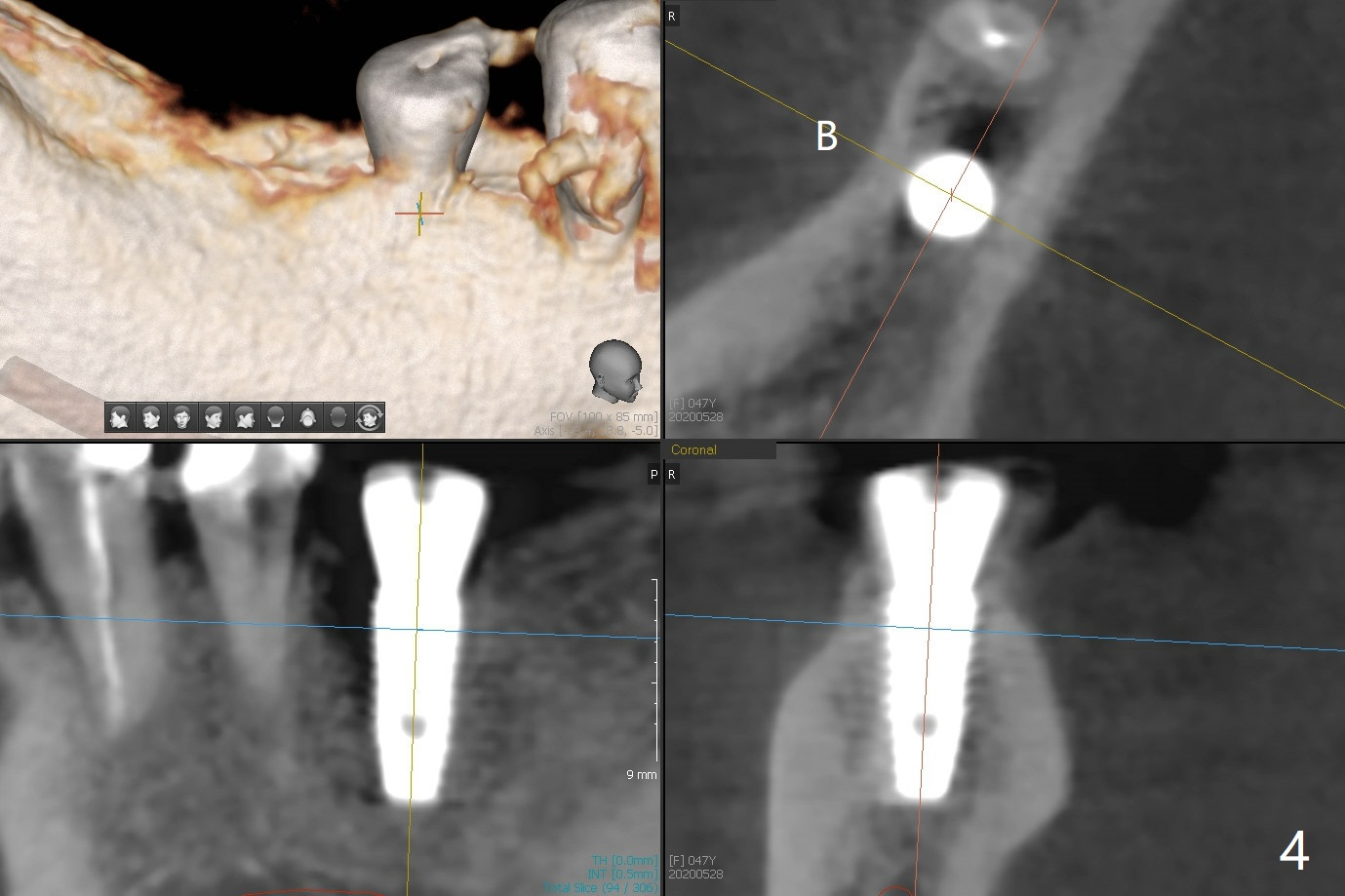
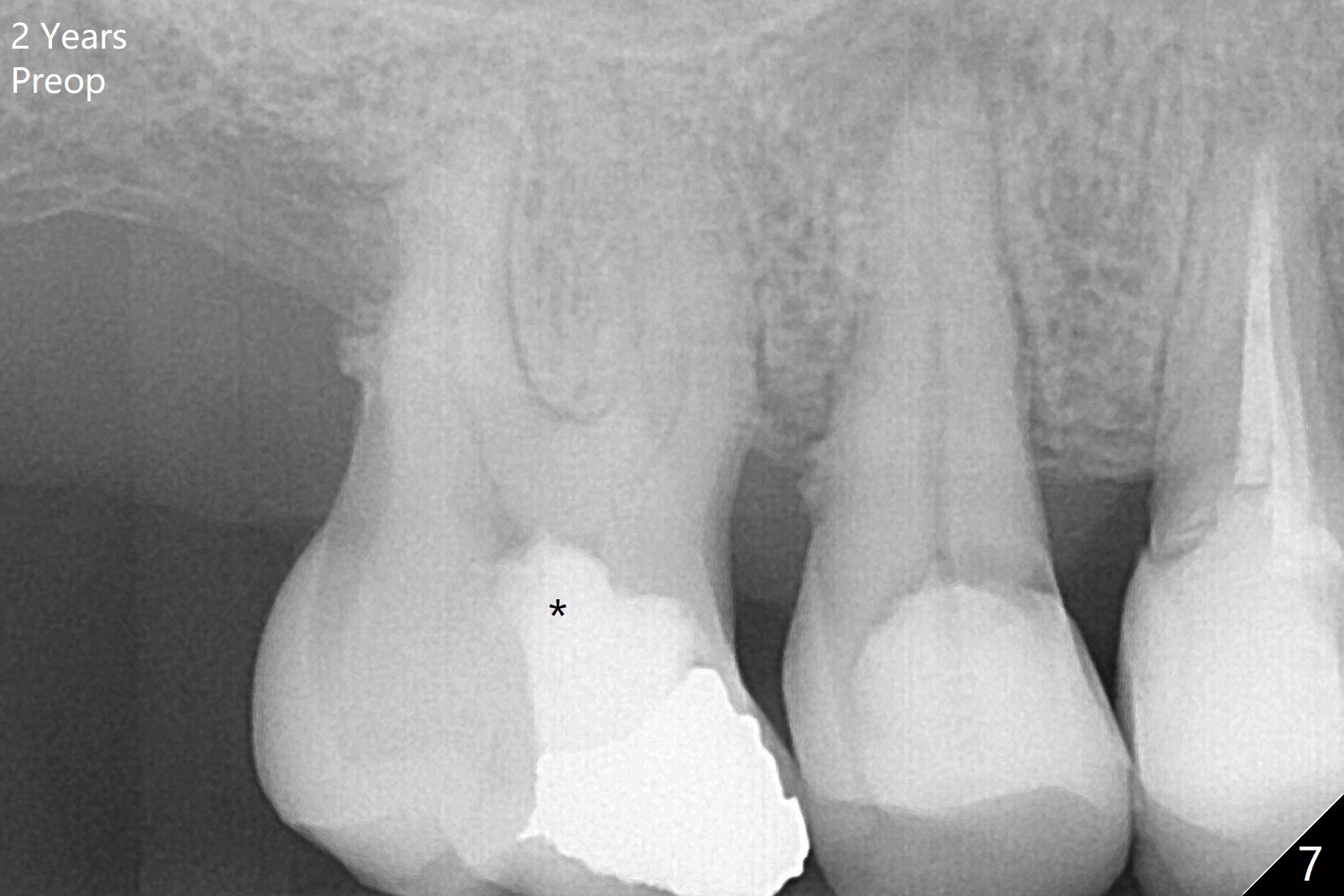
The female patient has limited mouth opening, complicated further by supraerupted opposing tooth. It is difficult to insert point drill and tap drill for #30 implant placement with guide. The former has to be inserted into the sleeve of the guide extraorally; two of them are placed intraorally together, while the tap drill is not used at all. When a 4.5x10 mm implant is placed, it is difficult to use #2 sensor to take PA. Finally a BW is taken with #2 sensor (Fig.1), while a PA is taken with #1 sensor (Fig.2). CT is taken to show clearance of the implant from the Inferior Alveolar Canal (Fig.3,4). To seat healing and later cemented abutments completely, a 5.5 mm profile drill is applied after implant placement; the outline is illustrated by red dashed line in Fig.1''. The elongated mesiolignual cusp of the tooth #3 has to be trimmed after placement of a 6x5 mm healing abutment. In fact trimming prior to osteotomy could solve the mouth opening partially. After removal of the 6x5 mm healing abutment, a 4.5x4(3) mm cemented abutment is incompletely seated (Fig.5 <) apparently due to proximity to the mesial crest (*). With reuse of a 4.6 mm profile drill, the abutment is fully seated (Fig.6), confirmed clinically by more clearance from the opposing tooth (Fig.7). Complete occlusal clearance is obtained by reduction of the opposing cusps without sensitivity since the tooth is nonvital (*). Return to No Deviation Xin Wei, DDS, PhD, MS 1st edition 05/28/2020, last revision 09/04/2020