

.jpg)
,%20changed%20to%20(4).jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
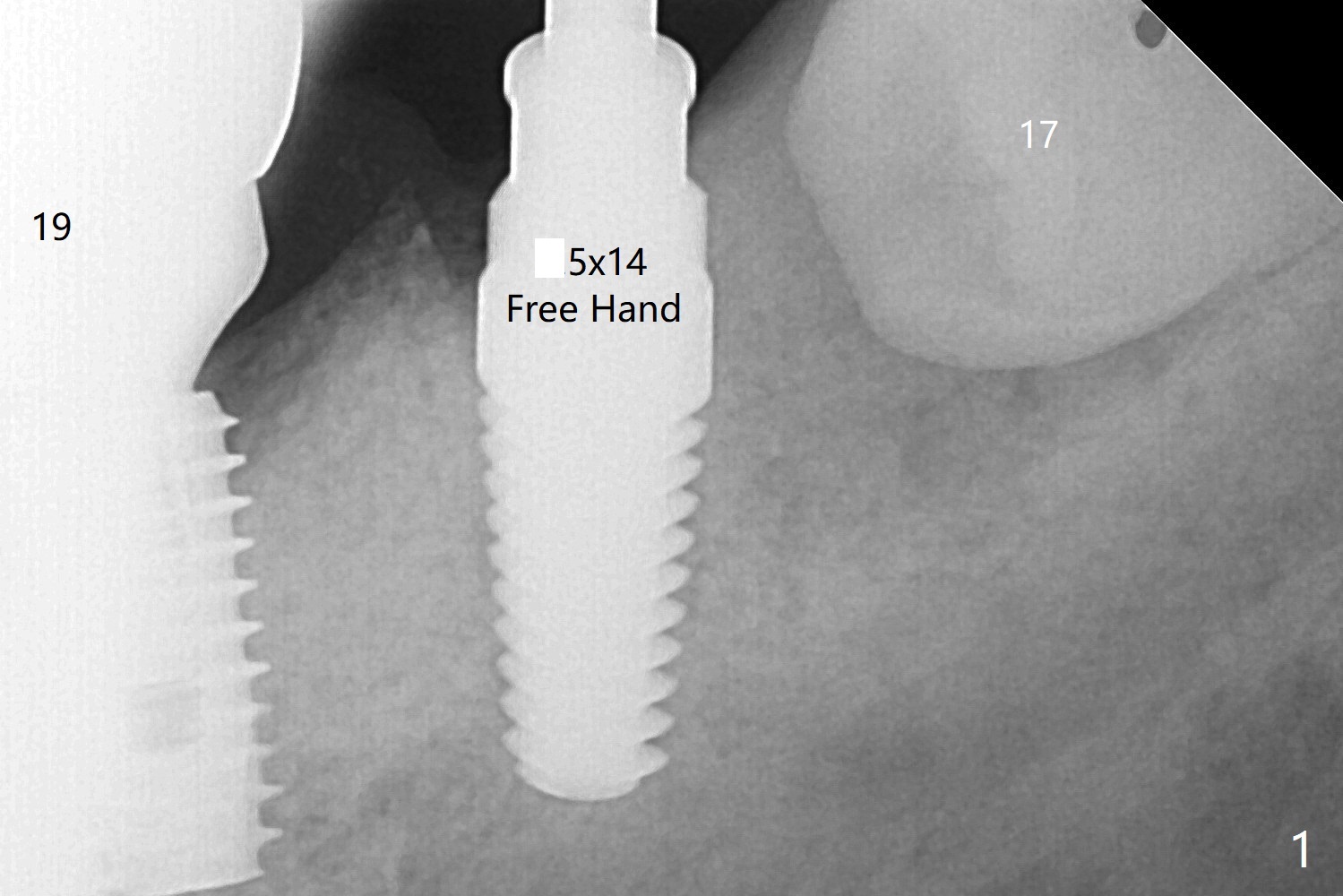
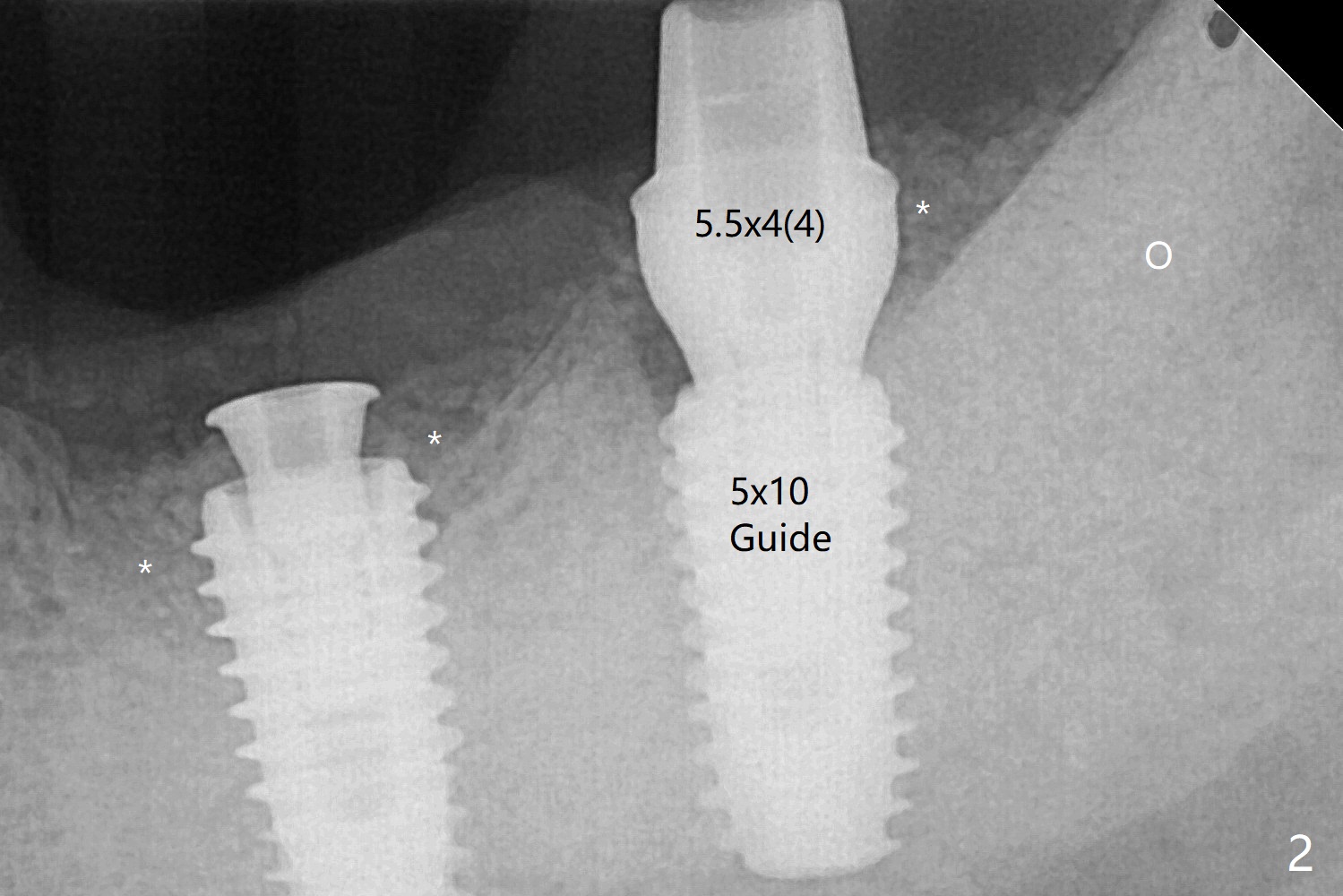
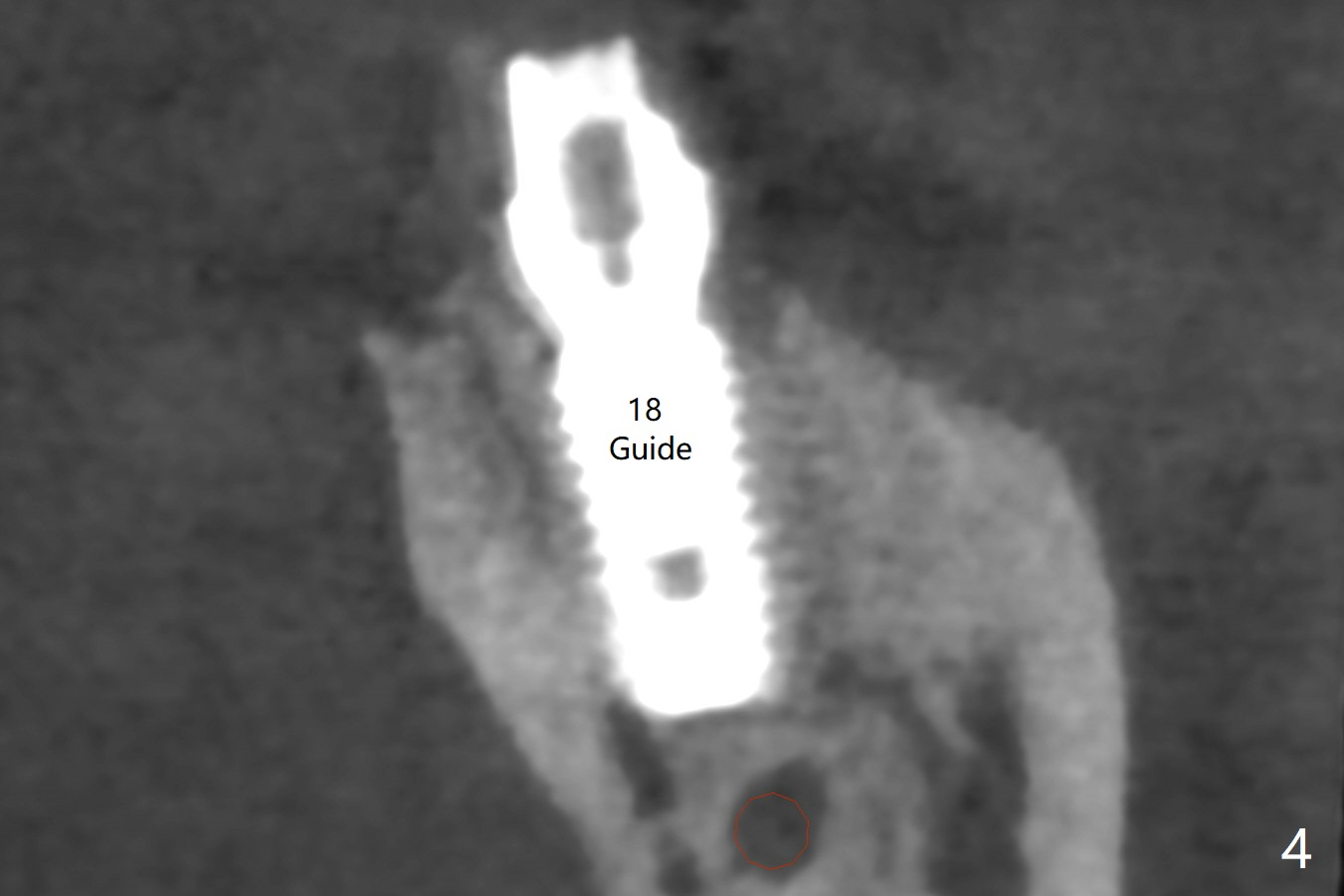
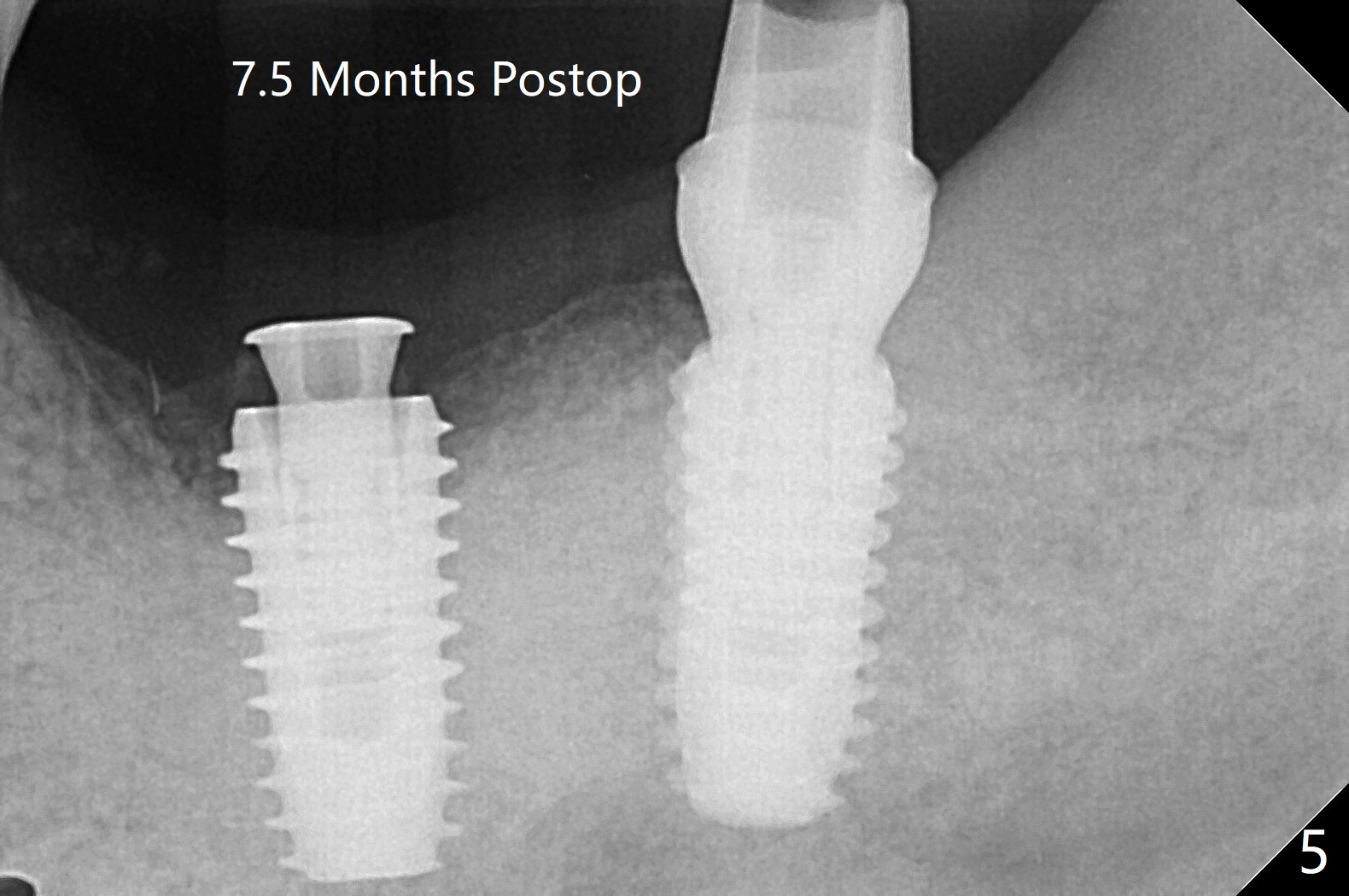
Guide vs. Free Hand M
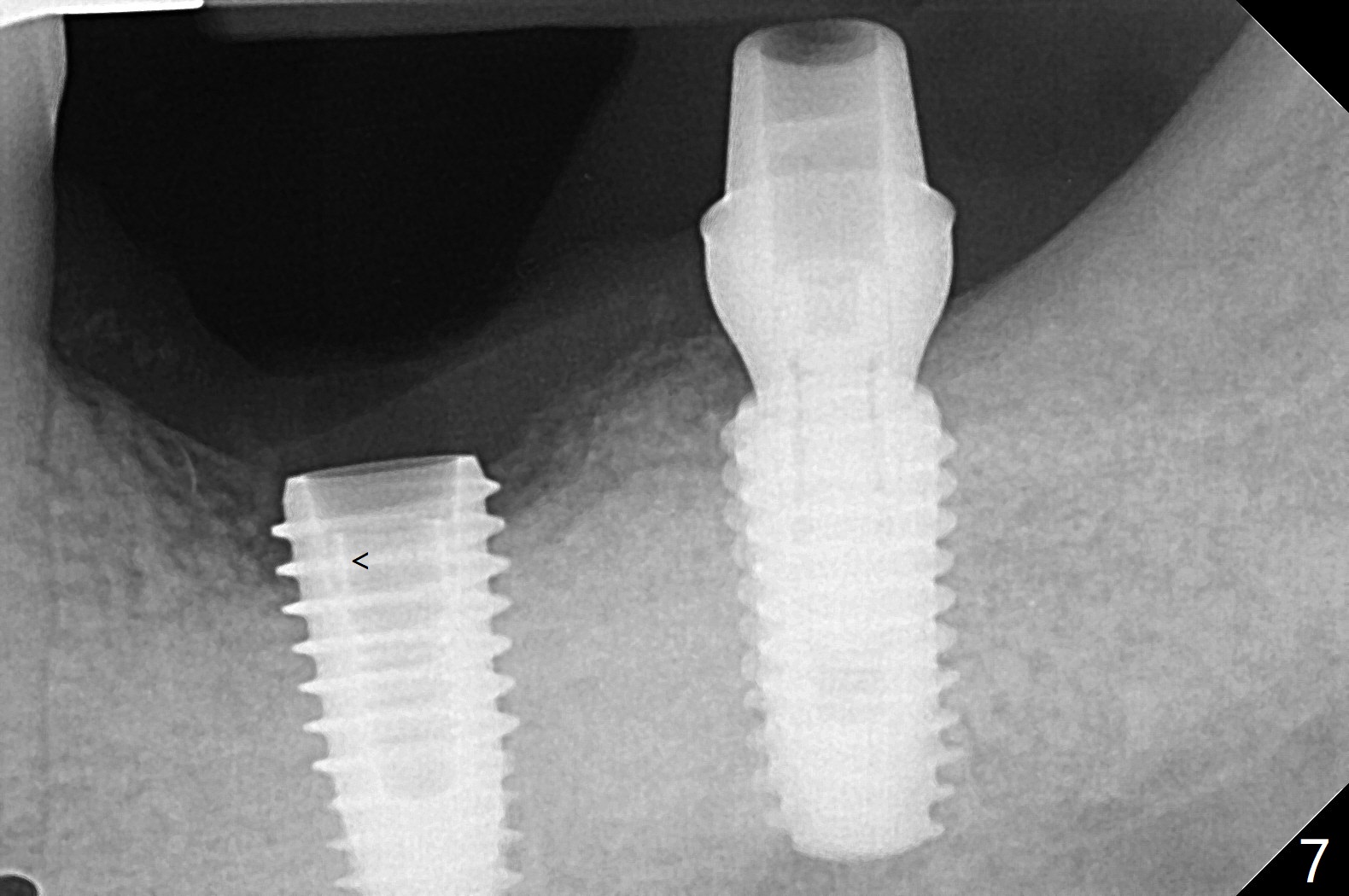
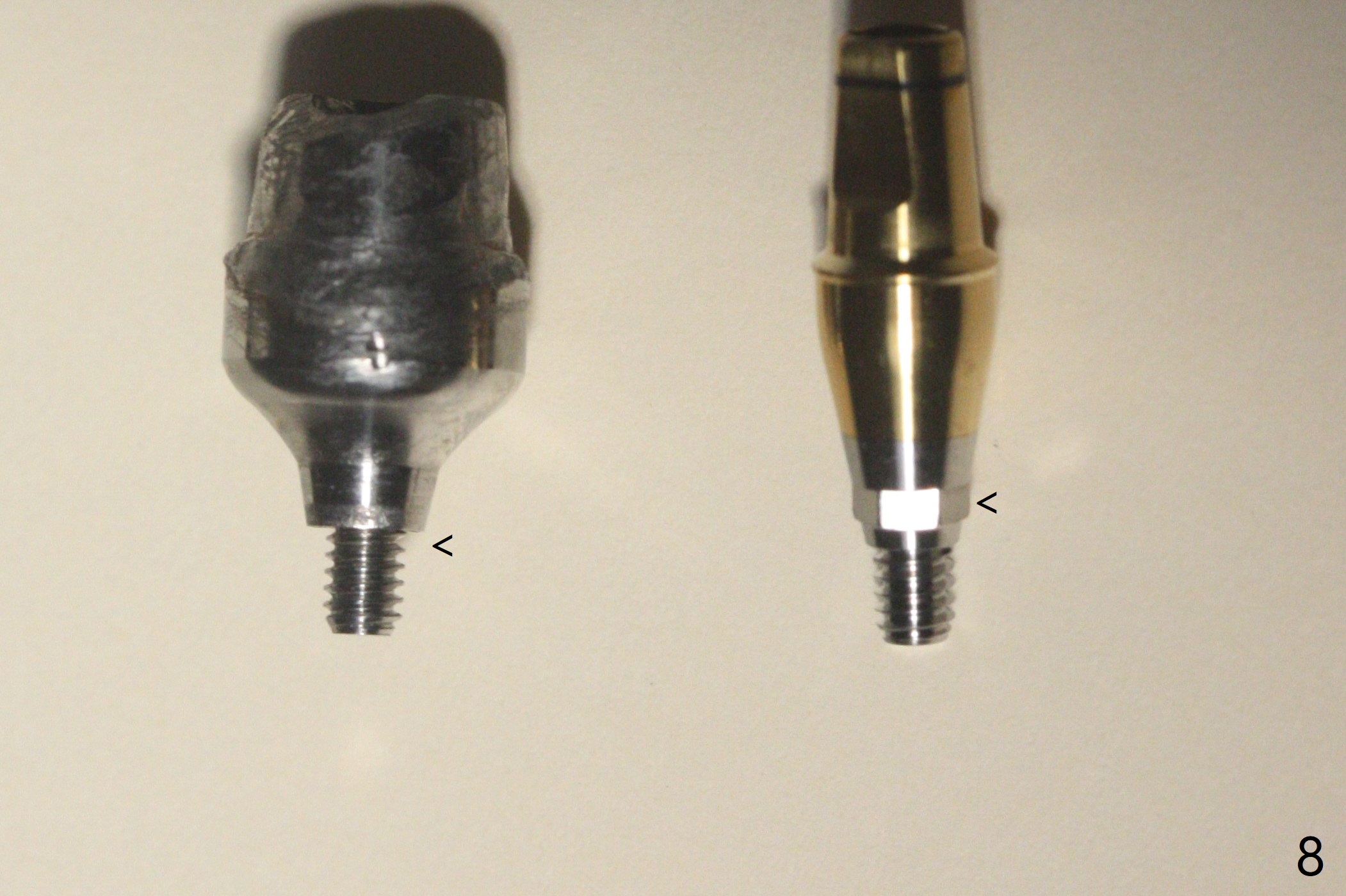
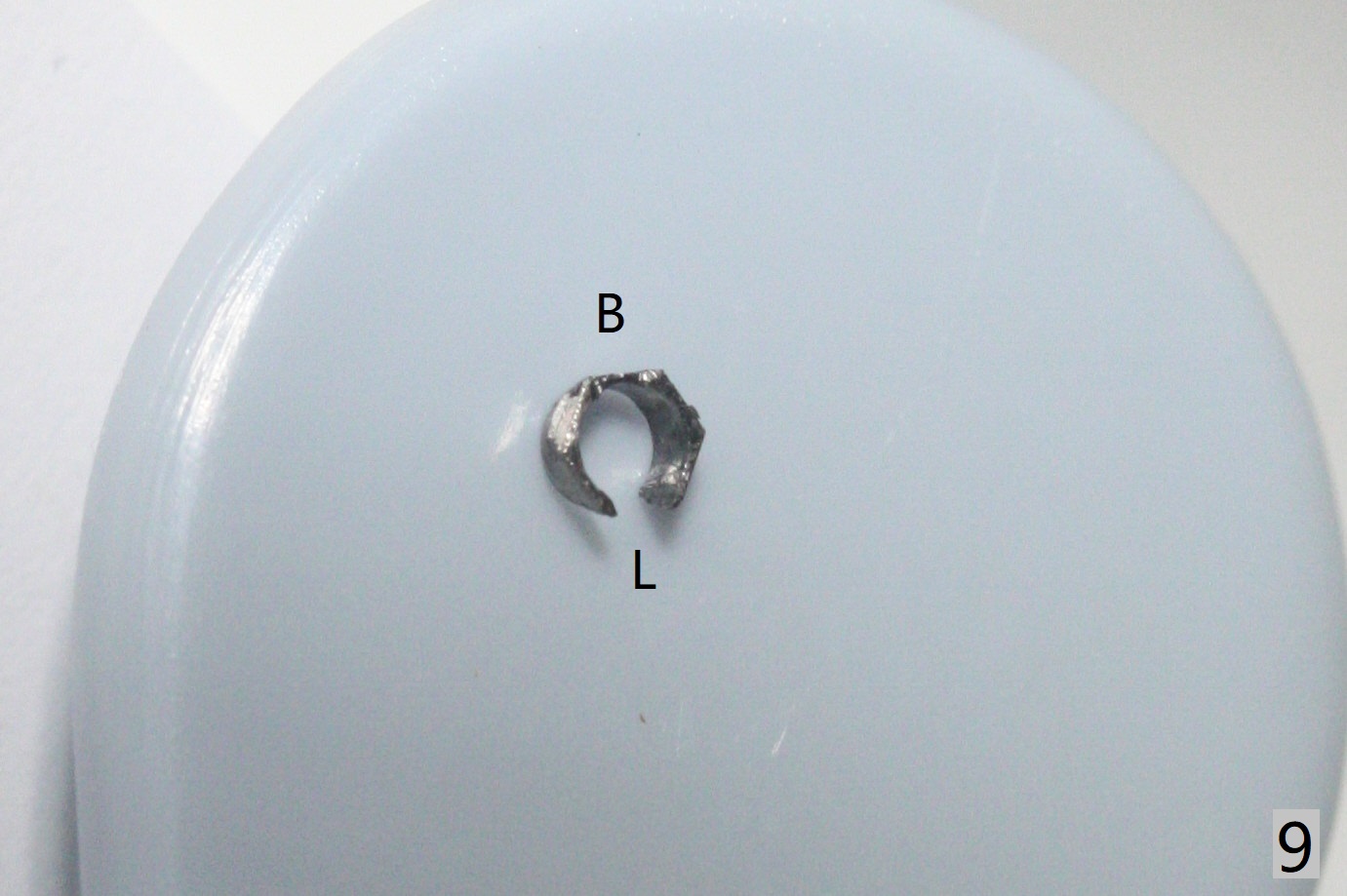
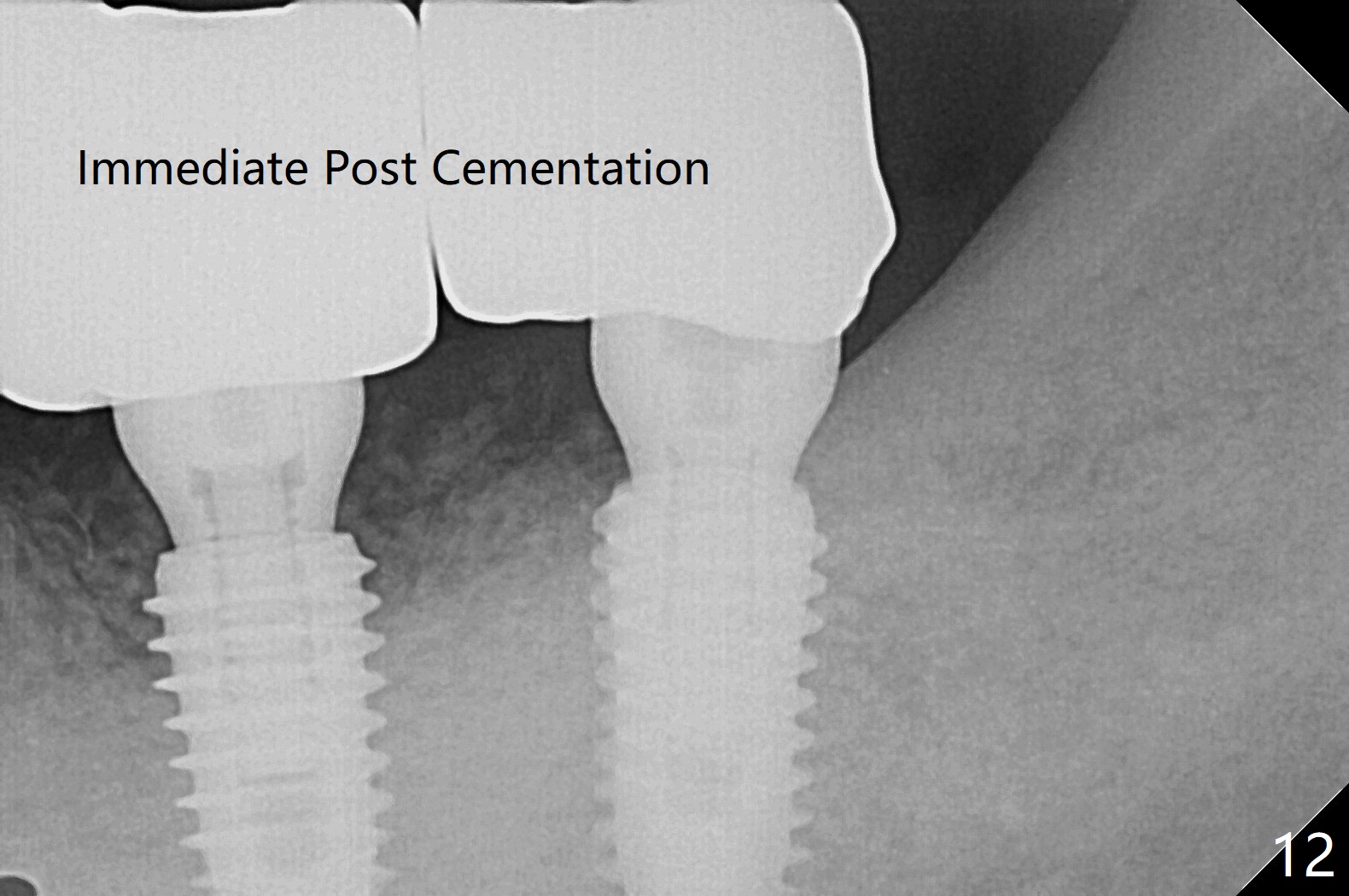
After finishing osteotomy with guide, a 5x14 mm tissue-level implant tap is used without guide because of limited mouth opening. It is not parallel to the implant at #19 (Fig.1). A bone-level implant is barely able to be placed with guide; it is parallel to #19 implant (Fig.2). Pre- and intra-op exam confirms periimplantitis at #19. In addition the horizontally impacted #17 has caries. A large incision is made for #19 debridement and bone graft. #18 bone graft (Fig.2 *) and #17 extraction and Osteogen plug (O) placement. Postop CT shows poor trajectory of #19 implant (Fig.3 (coronal section) free hand placement), which is associated with screw loosening and periimplantitis (lingual (L) threads supracrestal). In contrast #18 implant has good trajectory and placement level (Fig.4). The mesial defect of #19 seems to have been repaired and the implant at #18 osteointegrates 7.5 months postop (Fig.5). The wound at #19 heals except a small slit 7.5 months postop (bone graft, Fig.6). When the incompletely seated healing screw (Fig.2,3) is removed during uncover, it is difficult to place a cemented abutment. A healing abutment is placed instead. In fact the hex of the abutment fractures within the implant well (Fig.7,8 < (due to burial of 1.2 driver inside the abutment and bruxism)). Because of the deeply placed implant, incision is made and surgical long fissure bur is used to section the lingual (Fig.9 L) portion of the hex. When the buccal (B) portion of the hex is being sectioned, the hex dislodges by itself. There is no problem to insert a cemented abutment (Fig.10). Later a longer cuffed abutment is placed and bone graft is placed around the coronal threads (Fig.11 *). The bone graft around #19 implant looks stable 2 weeks post 2nd grafting (Fig.12). Return to Prevent Molar Periimplantitis (Protocols, Table) No Deviation Screw Xin Wei, DDS, PhD, MS 1st edition 02/10/2020, last revision 02/26/2021