


|
|
|
|
|
|
|
|
|
|
|
|
Ridge Preservation
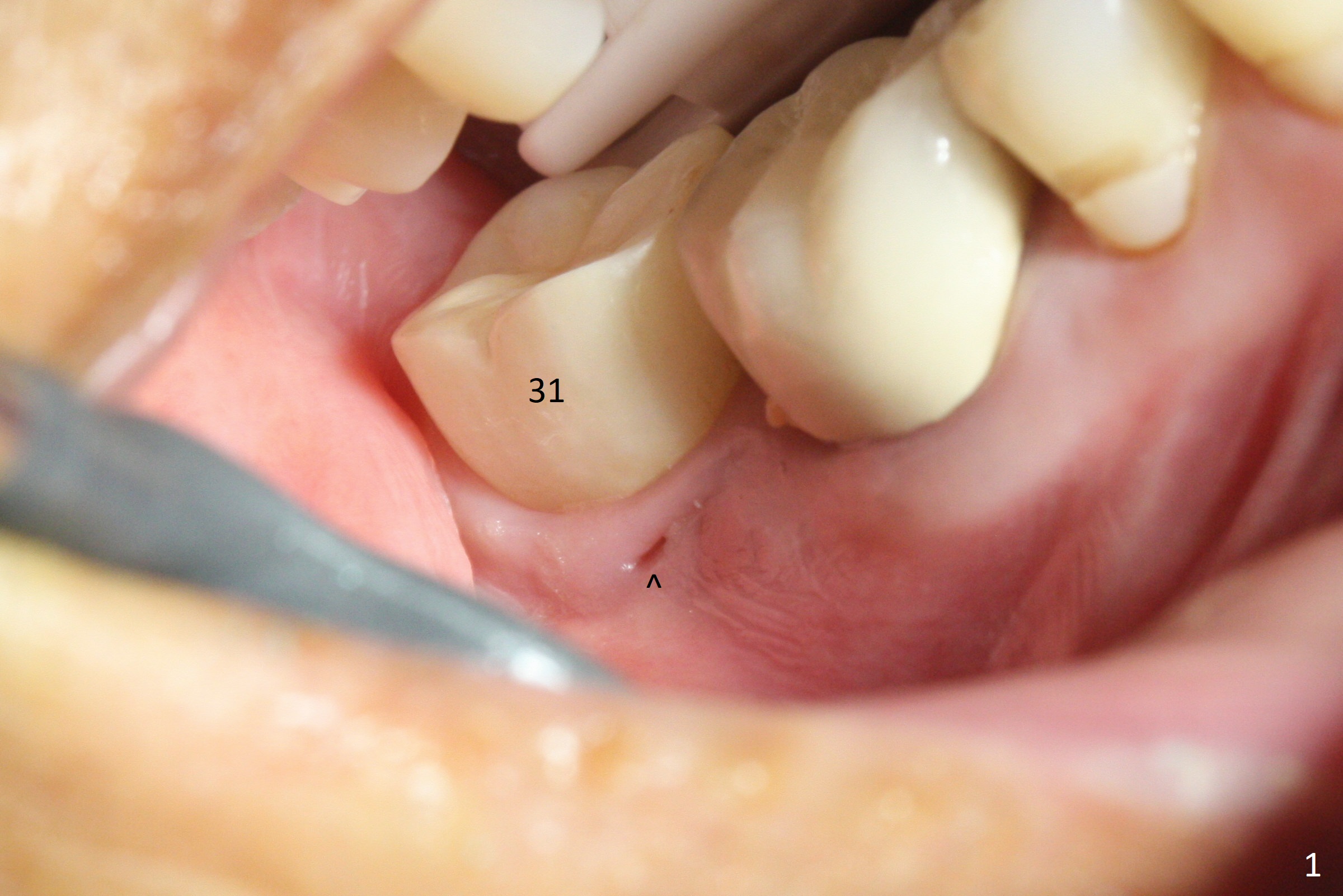
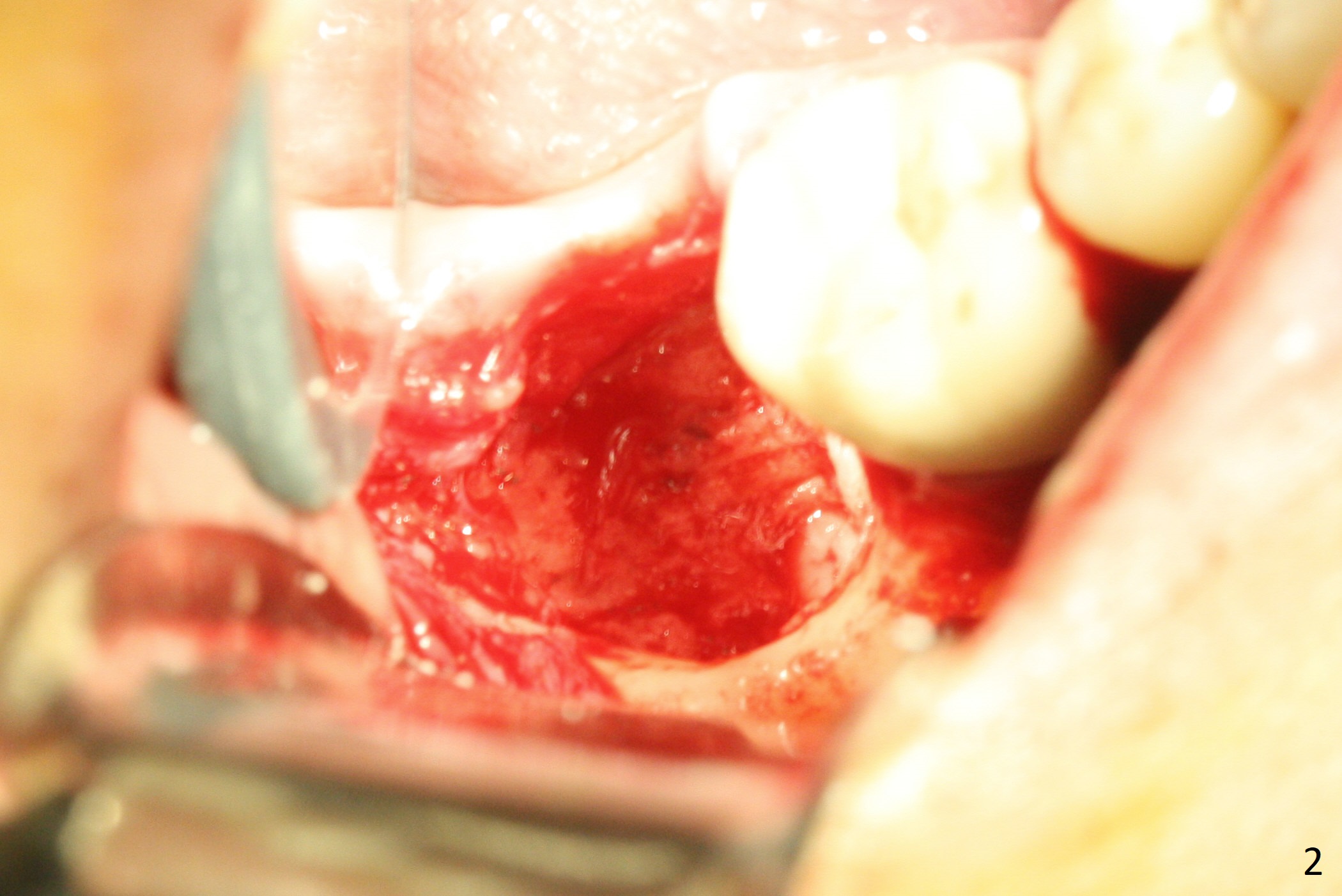
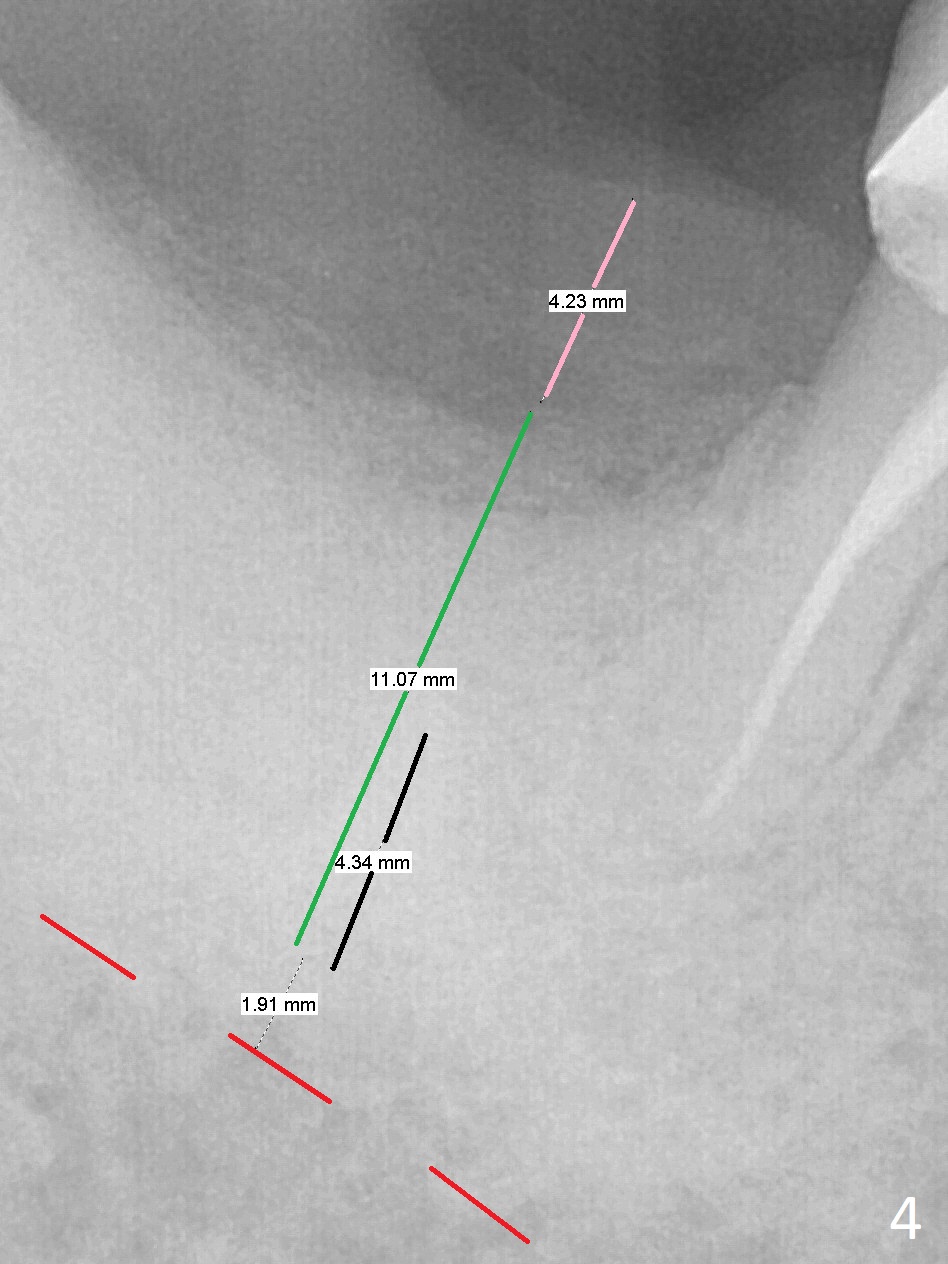
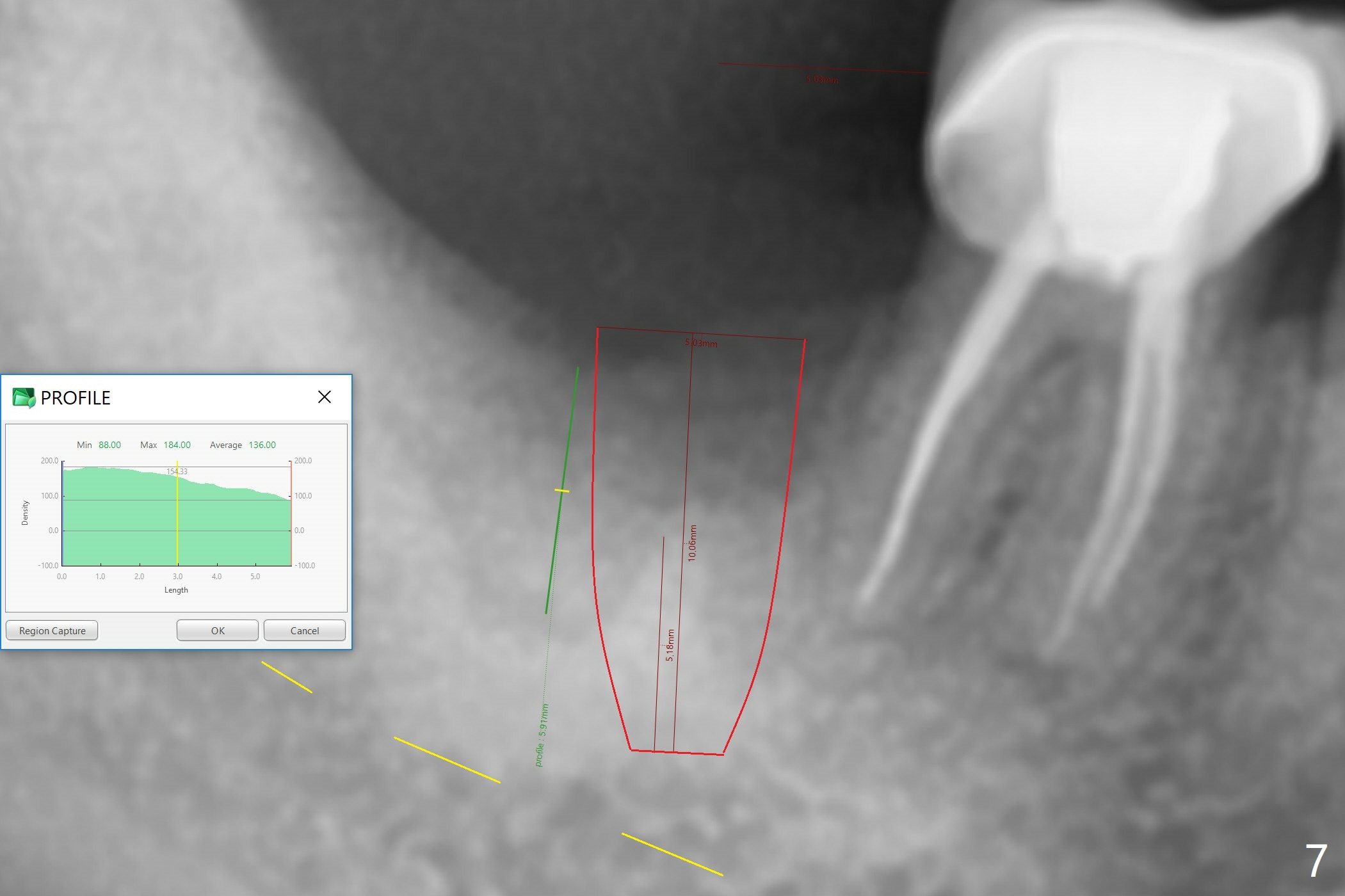
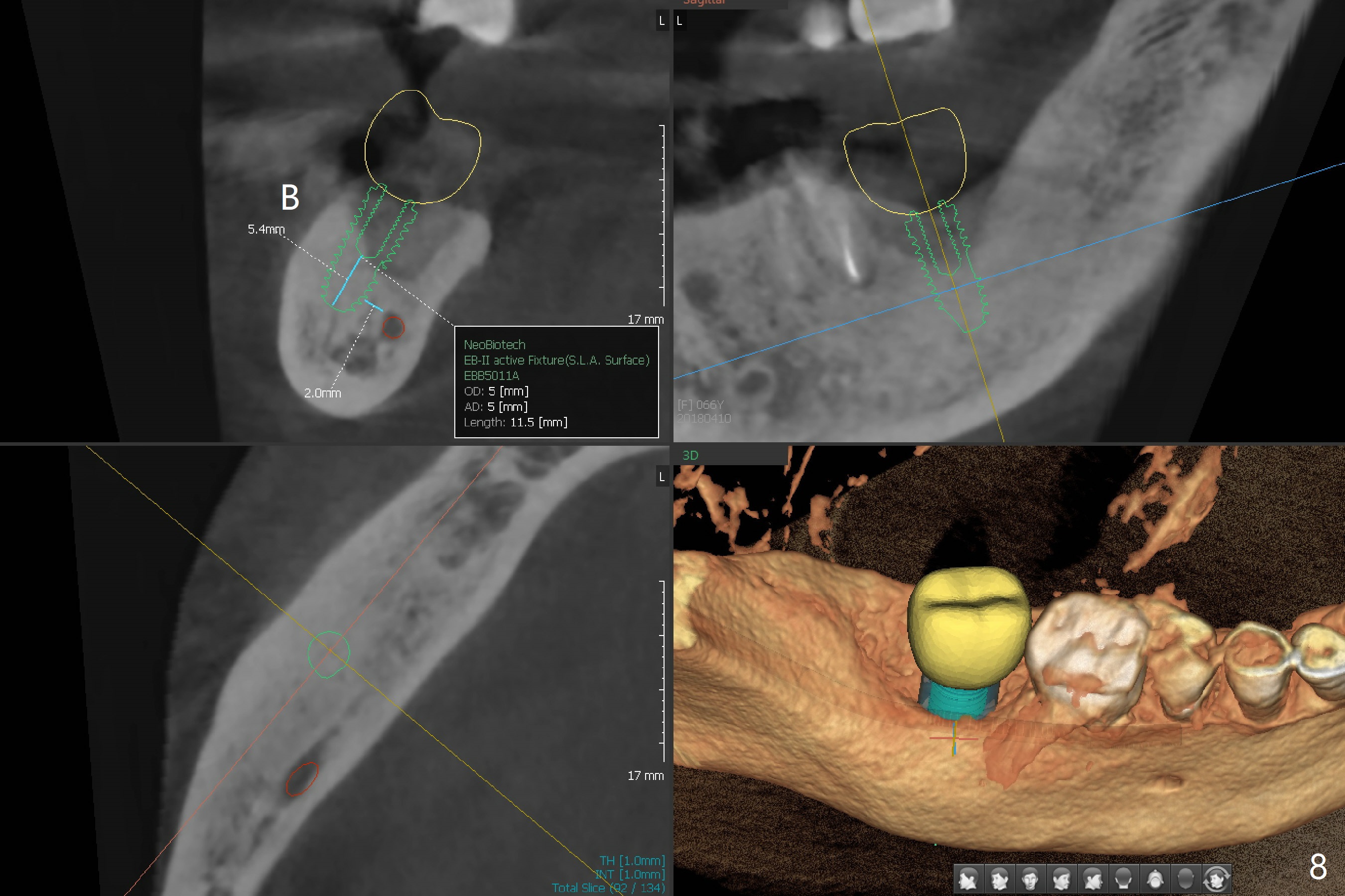
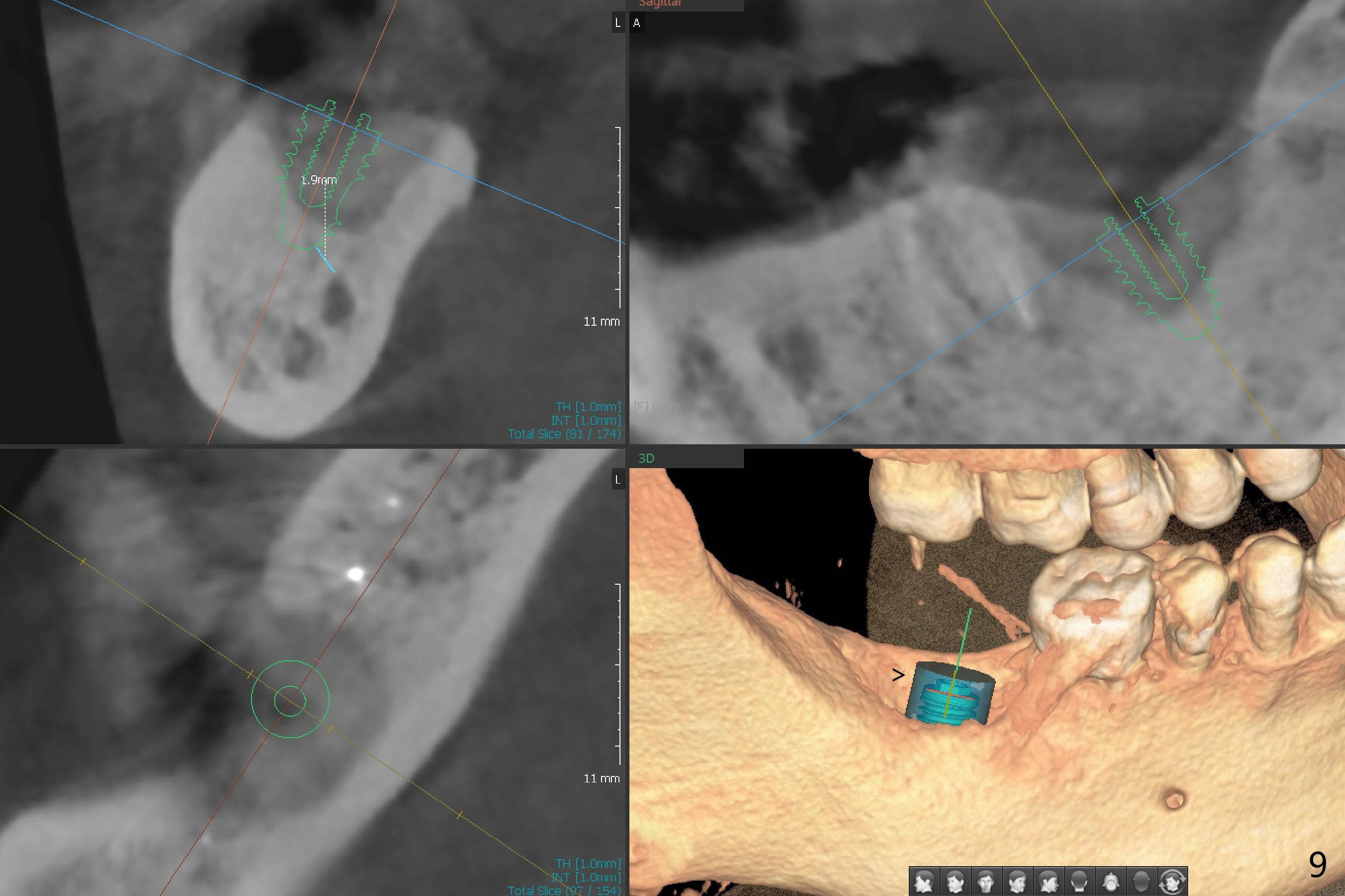
There is a mesiobuccal fistula at #31 with periimplantitis (Fig.1 ^). The bone loss is severe before and after implant removal (Fig.2). It is impossible to place bone-level implant in the original osteotomy due to insufficient bone height. There is pain when a new osteotomy is being initiated in the mesial slope. Following placement of Vera Graft (Fig.3), collagen plug and 6-month resorbable membrane, the wound is closed with suture (mild tension). Postop, there is oozing. Periodontal dressing should have been applied. If the ridge can be preserved in 4-6 months, a 11 mm long implant (Fig.4 green line with 4 mm of the native bone) can be placed with 1.9 mm clearance (red dashed line: the superior border of the Inferior Alveolar Canal); the abutment is estimated to have 4 mm cuff (pink). The socket appears to be healing 8 days postop (Fig.5). The ridge remains wide 5 months post implant removal, although the bone density is low (Fig.6,7 (still ~ 1000 units). It seems that a 5x11.5 mm implant could be placed in the mesiobuccal aspect of the bony defect (Fig.8). For better occlusion, the implant should be shorter (5x8.5 mm) after discussion with the guide lab (Fig.9). Make sure that the most coronal thread is buried by the bone graft, i.e., underneath the crest(>).
Return to Lower Molar Immediate Implant, Armaments Xin Wei, DDS, PhD, MS 1st edition 11/13/2017, last revision 04/19/2018