,%204.5x4(4).jpg)
,%204.5x4(4).jpg)
,%204.5x4(4).jpg)
.jpg)
,%20PA.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
Shorter IBS Implants in Mandible M
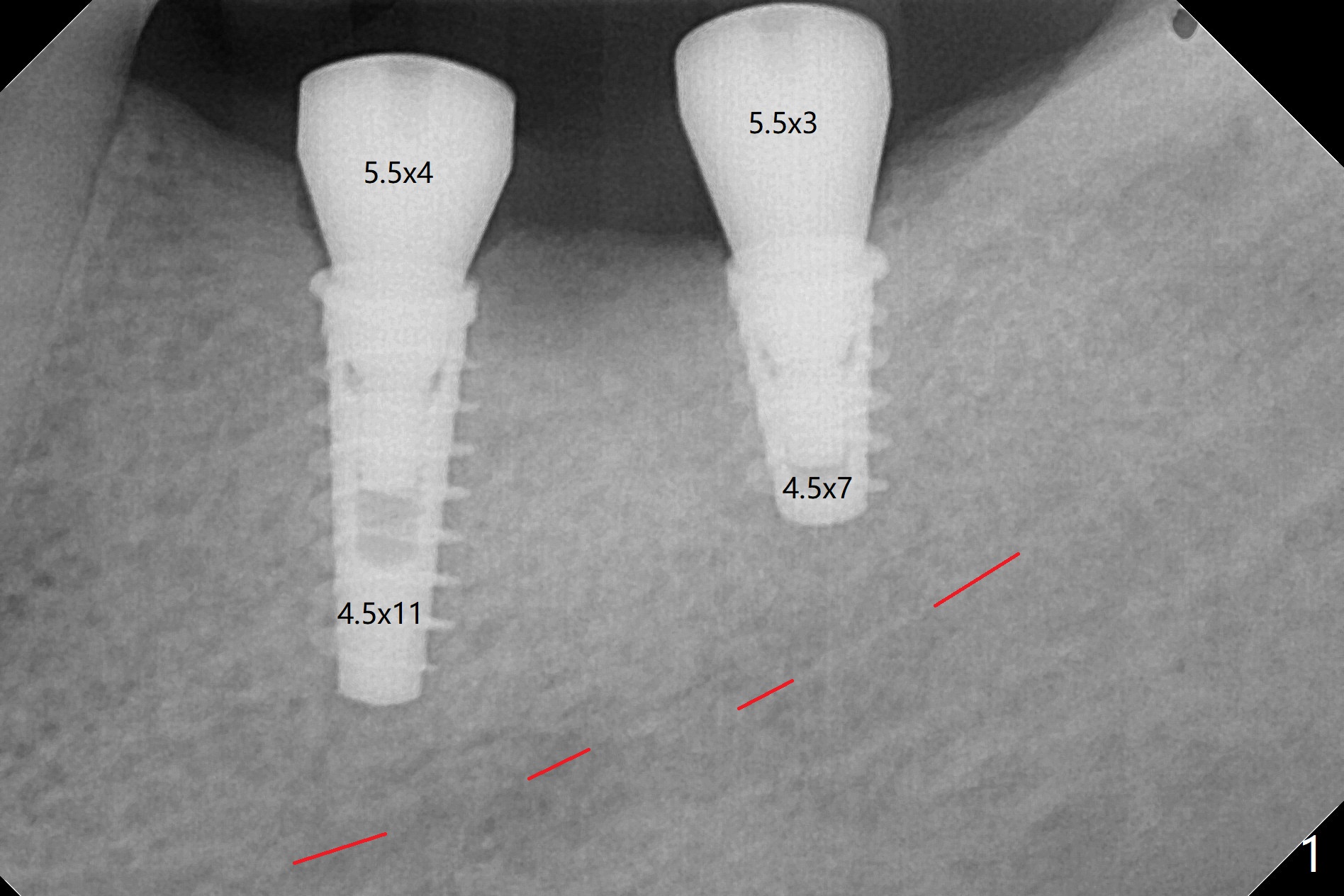
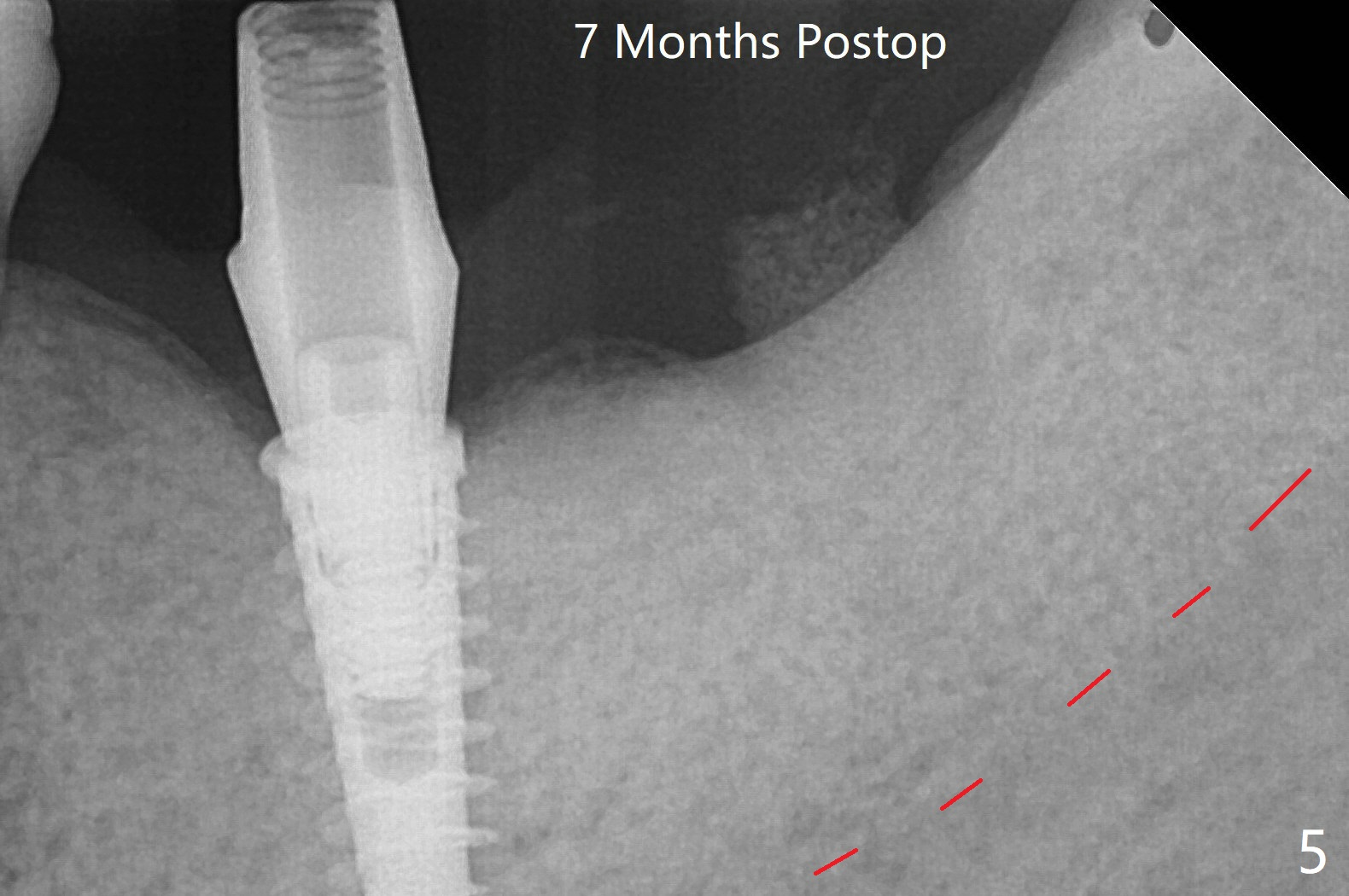
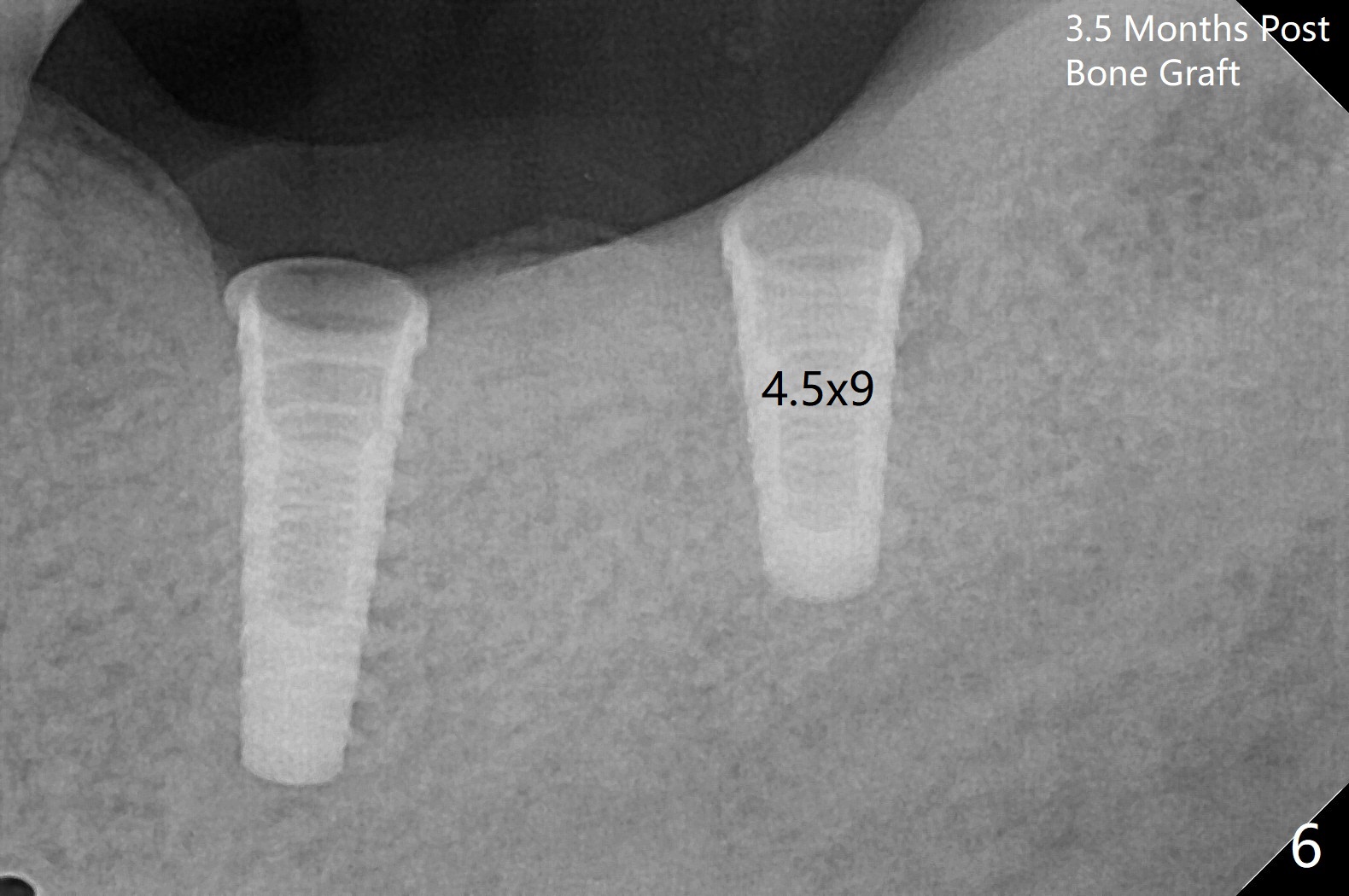
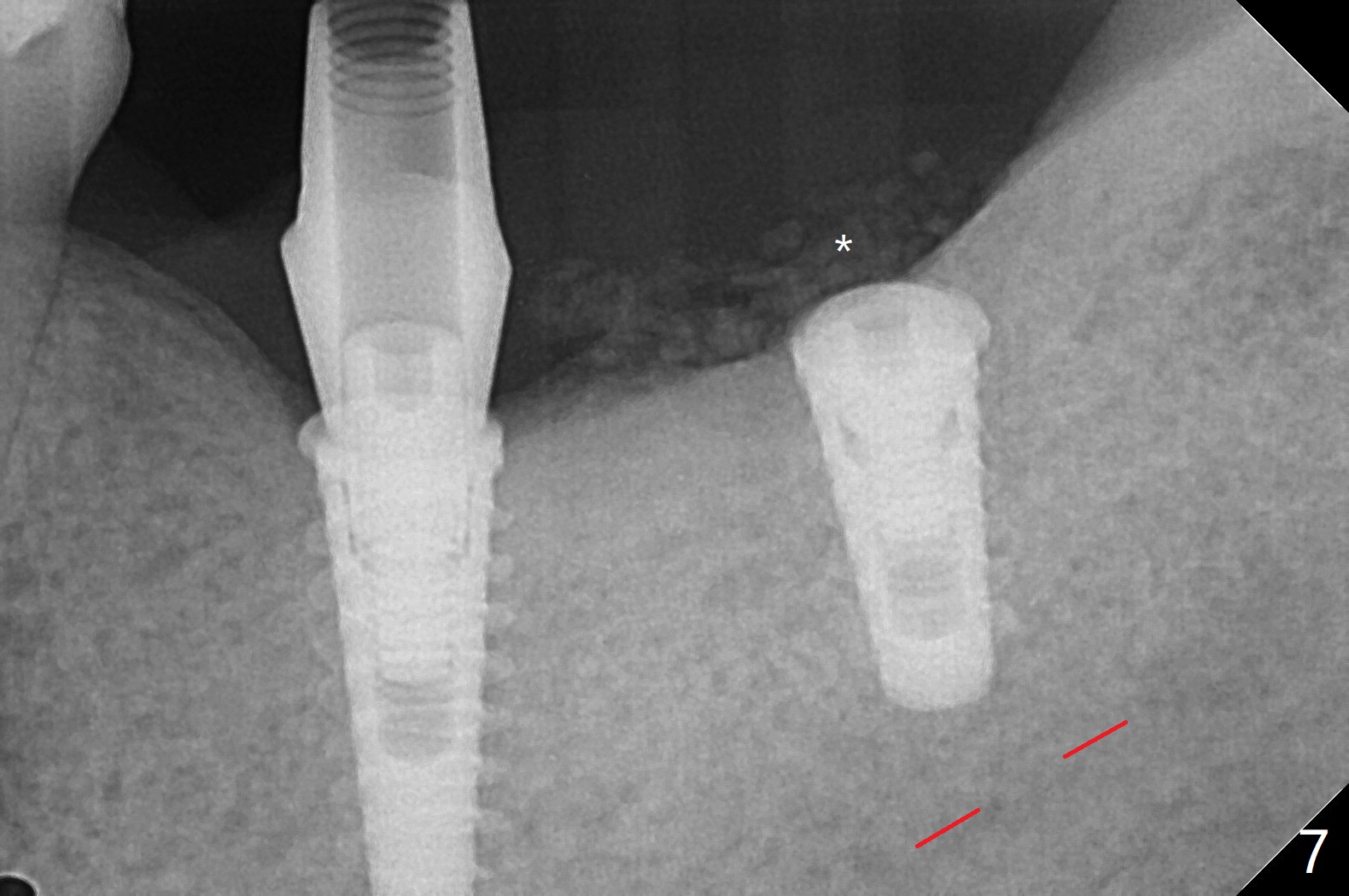
Following placement of a 4.5x11 mm implant at #19 (14 months post guide fabrication), a fixture anchor pin is placed. With stable guide, it is much easier to finish osteotomy and implant placement at #18 (Fig.1). Since the patient is nervous and sensitive to drilling, a shorter implant is placed (7 mm instead of 9 mm vs. 8.5 mm drill). The stability is unaffected because of the dense bone. After use of 5.5 mm profile drill, healing abutments (5.5x3 and 5.5x4 mm) are placed without interference. There is crestal bone loss in 3 months (Fig.2, as compared to Fig.1). Since there is more space apical to the pair abutment at #19 than that at #18, incomplete abutment seating is suspected at #19. More X-ray will be taken (Fig.3,4). In fact, it is not necessary. The space differential is also noted with healing abutments in Fig.1. BW cannot tell whether the abutment at #19 is seated or not (Fig.3). When the abutment is changed at #19 with 30 Ncm torque, the space differential remains (Fig.4, as compared Fig.2) and must be normal. The shorter implant at #18 appears not osteointegrate, since the patient feels pain when the abutment is torqued at 15 Ncm. The patient returns for temporary crown contour adjustment 1-2 weeks later. The implant at #18 is removed when the abutment screw is untightened 7 months postop; Cortical bone is placed with 6 month membrane (Fig.5). Three months later, incision will be made with reuse of the guide with fixture pin at #19. If a 4.5x9 mm implant cannot be placed, bury a short and/or narrow implant. Impression will be taken for #19 soon. In fact fixture pin cannot be seated. It appears that cancellous bone reforms, presumably low density. Underdrilling is conducted in diameter. The torque is high, but normal drilling is not carried out. The former implant exfoliated probably due to compression necrosis. The new implant is not completely seated, partially out of fear of being close to the Inferior Alveolar Canal (Fig.6). After cortical plate perforation, allograft is placed (Fig.7 *), followed by buccal flap release (periosteum underscored). In fact the implant does not have enough clearance from the Canal (red dashed line: the superior border of the Canal). The abutment at #19 returns to hold periodontal dressing in place. The implant is buried in the bone except lingual 4 months postop (Fig.8,9).
Return to No Deviation Xin Wei, DDS, PhD, MS 1st edition 01/30/2020, last revision 04/14/2021