




|
|
|
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
||||
|
|
|
|
||||
Partially
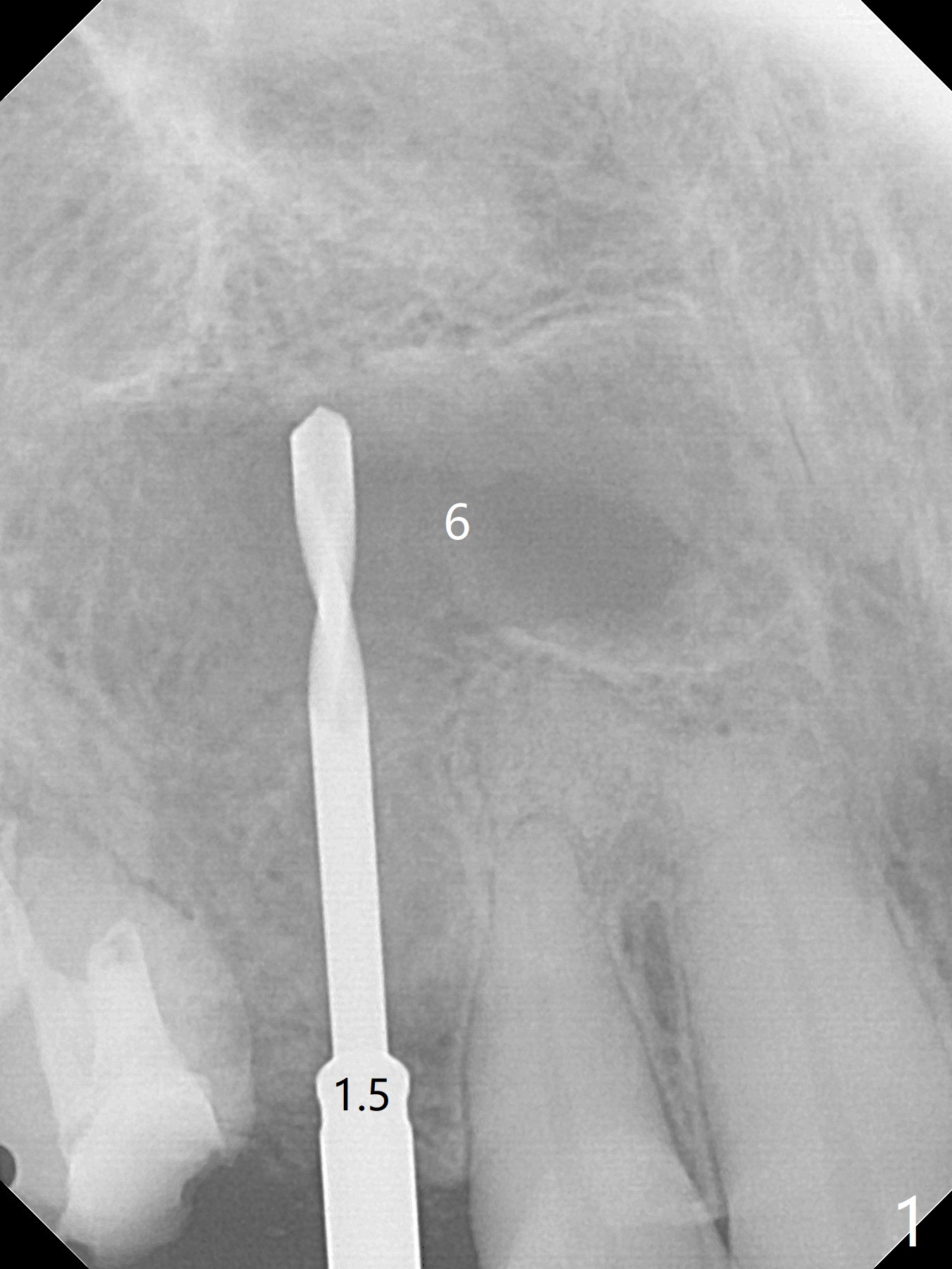
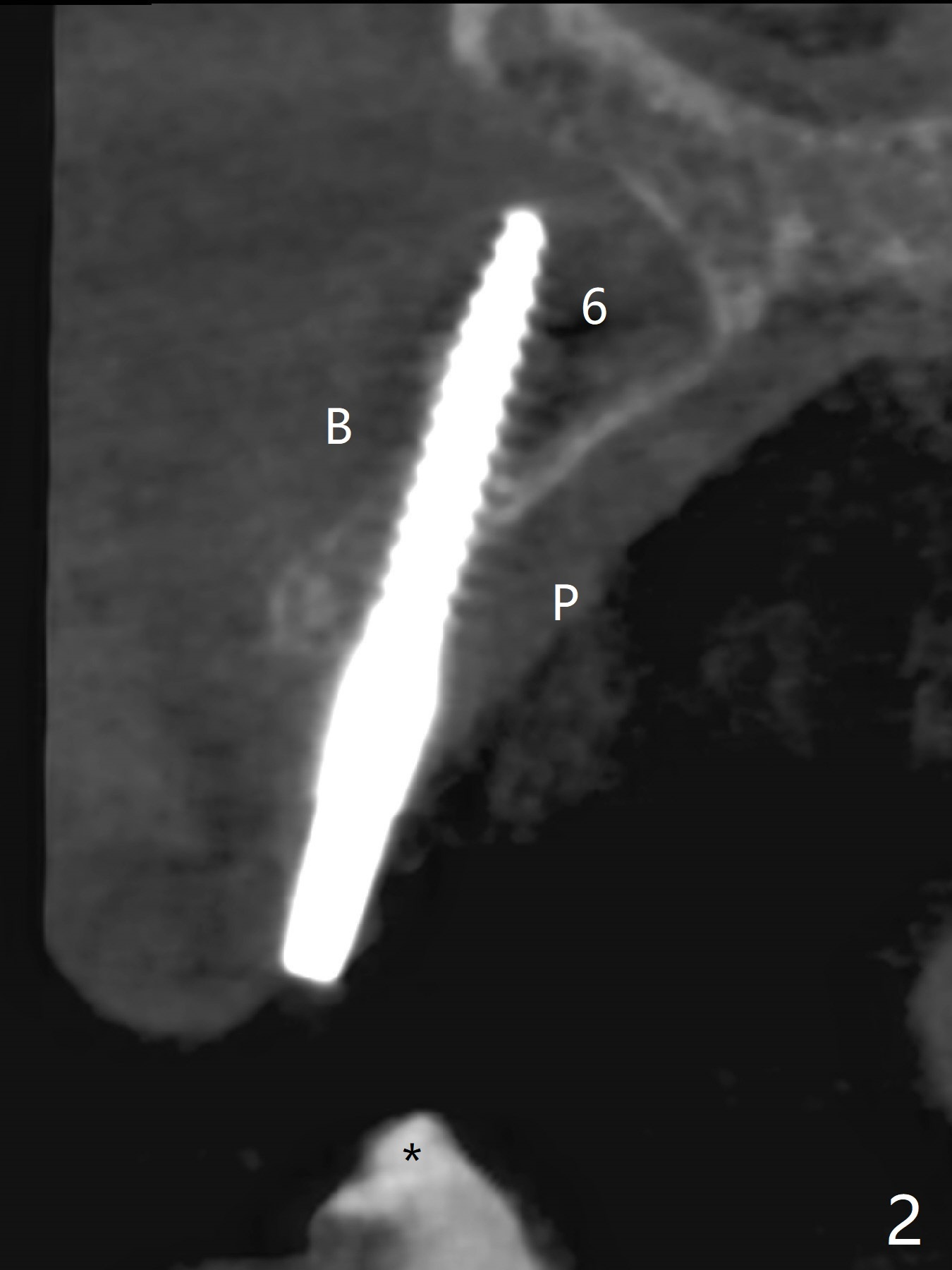
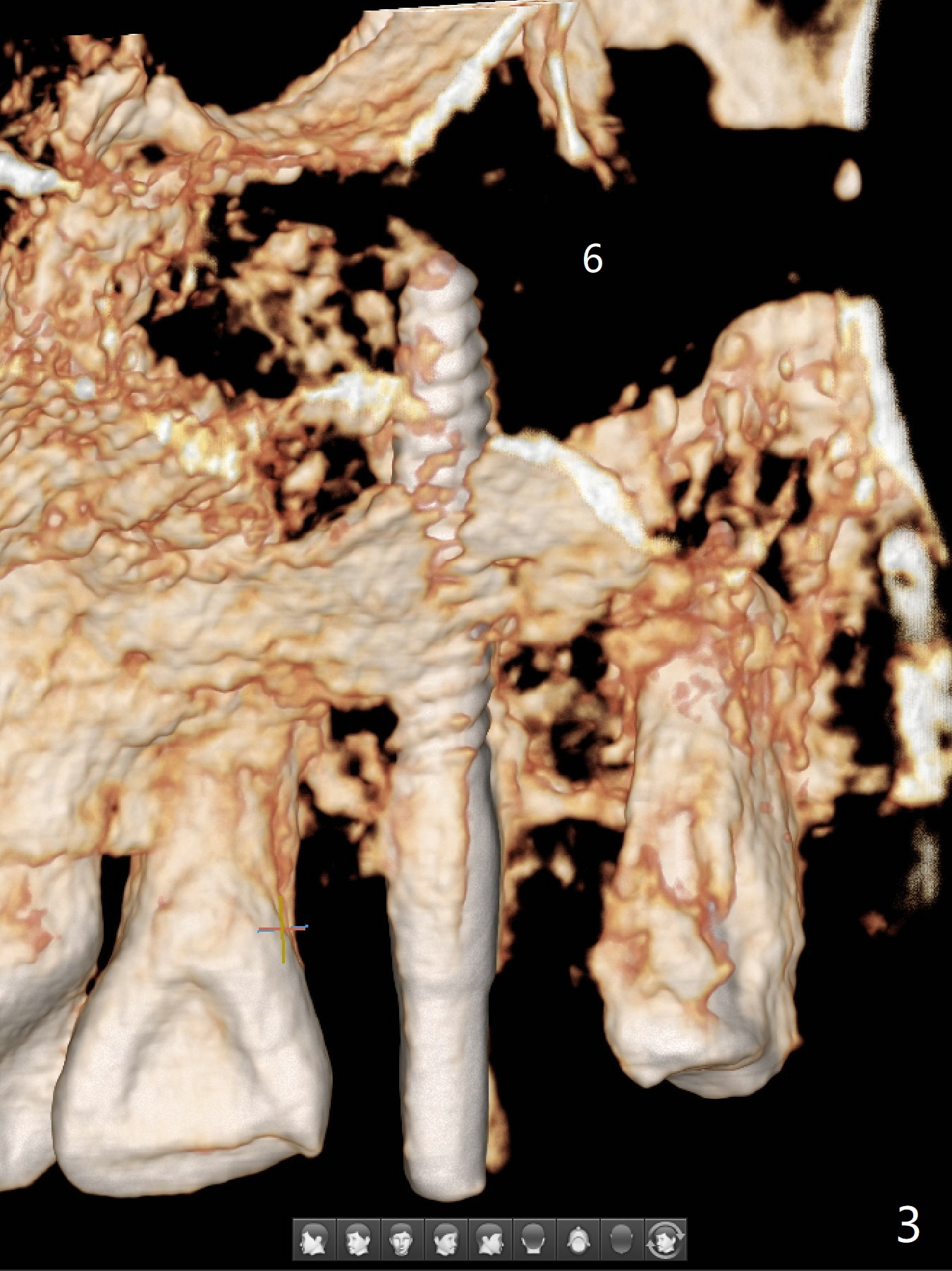
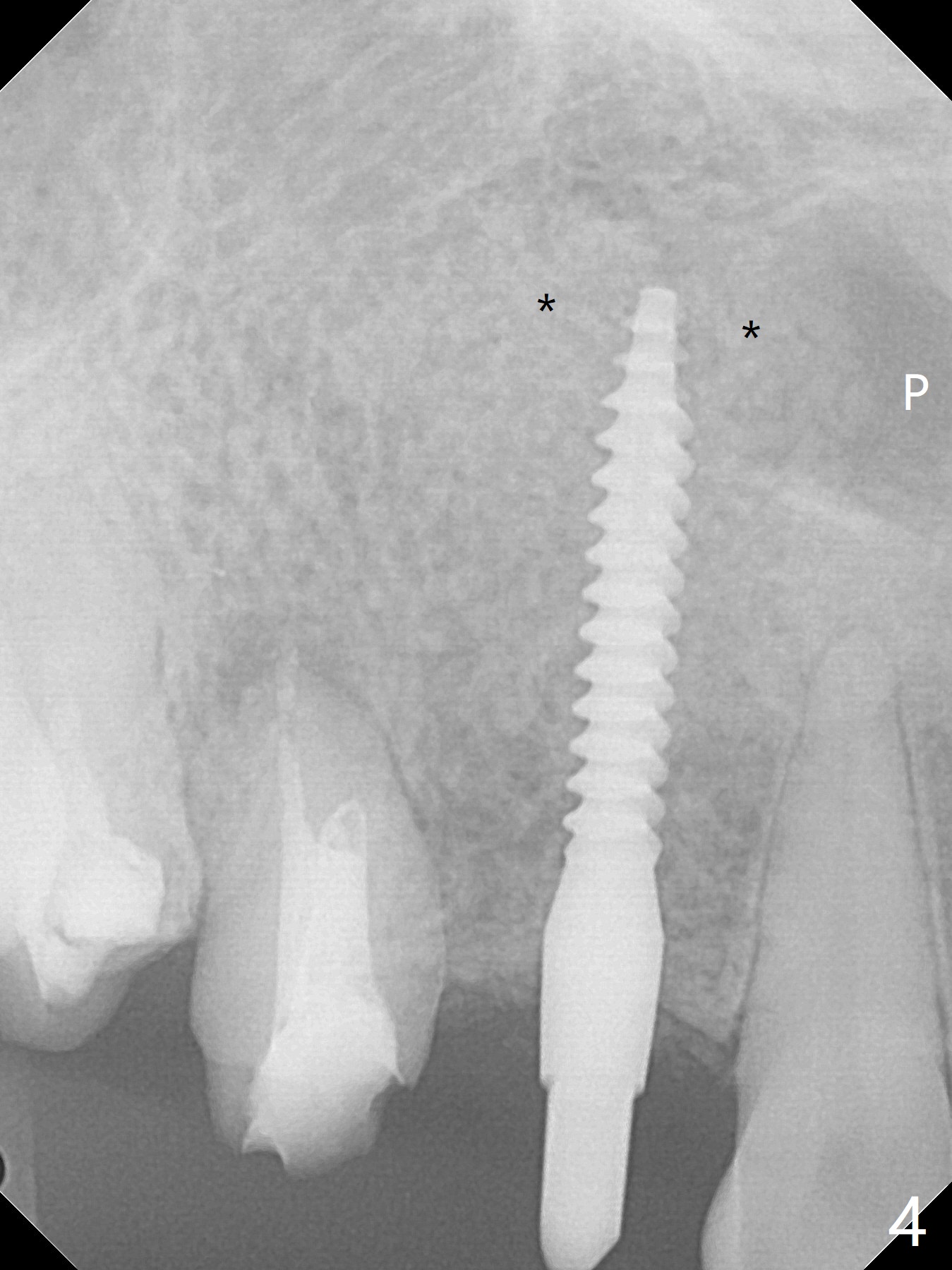
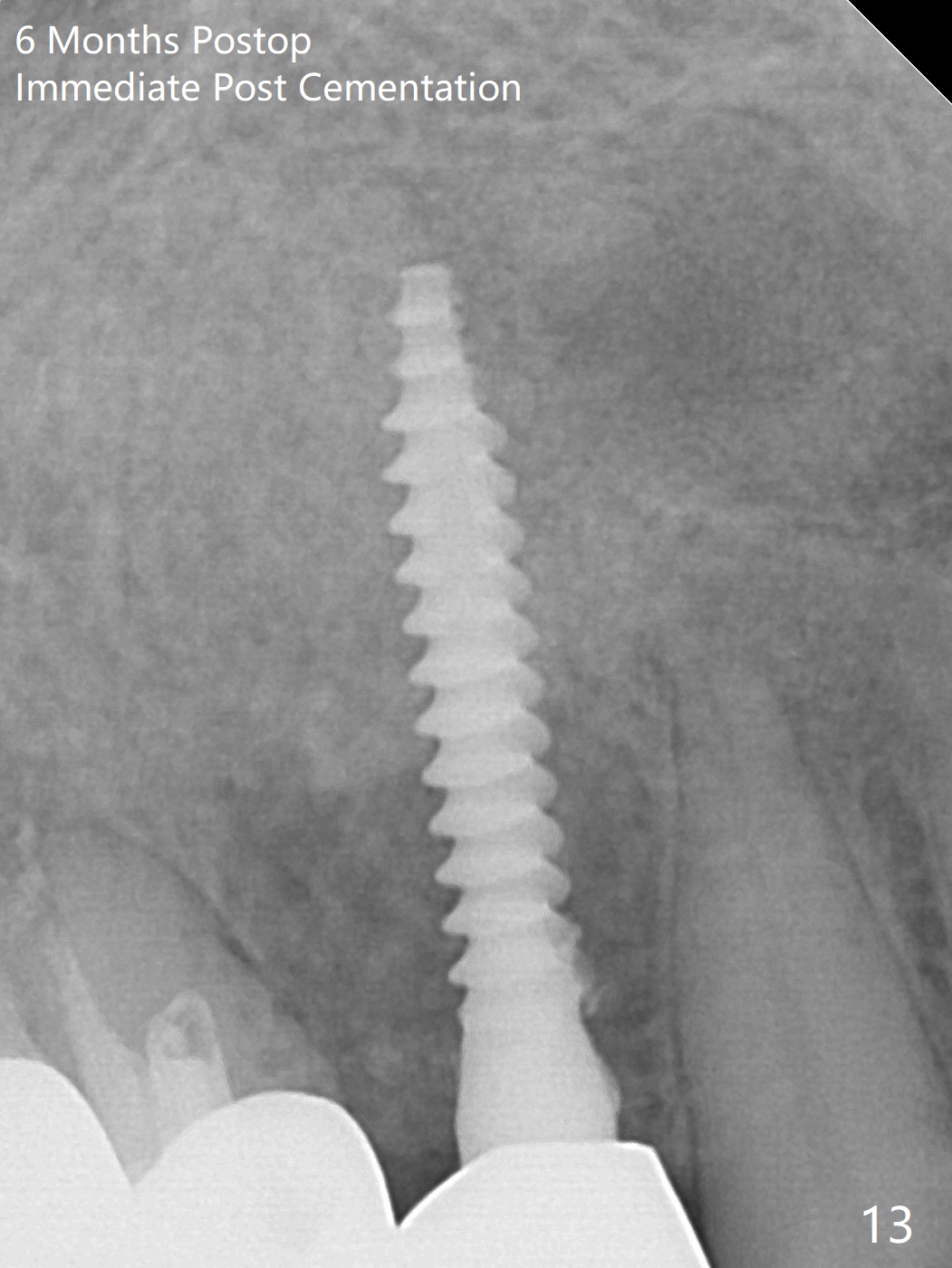
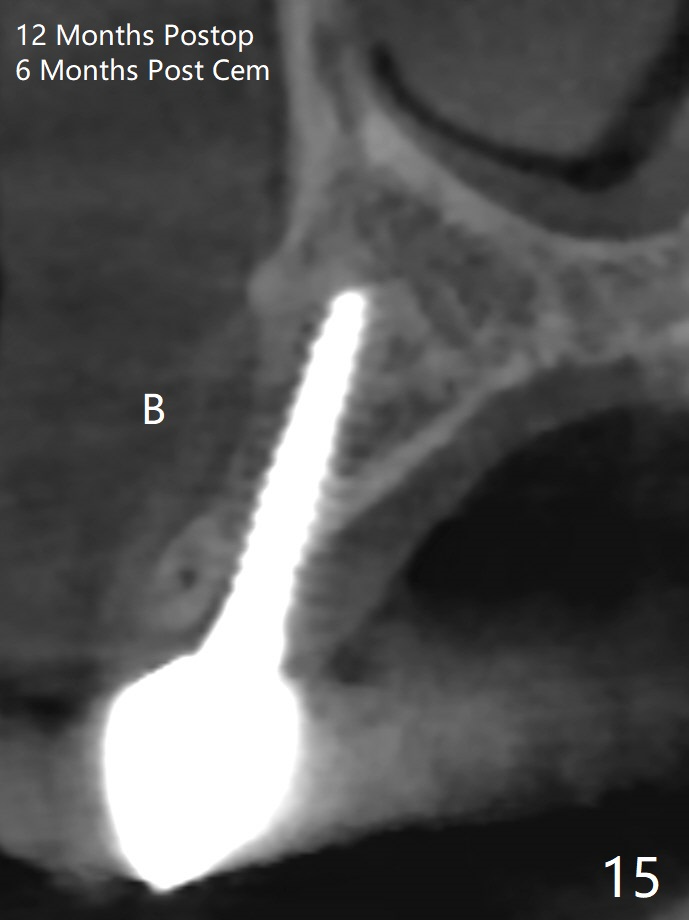
Guided Atypical Immediate Implant for Impacted Canine I
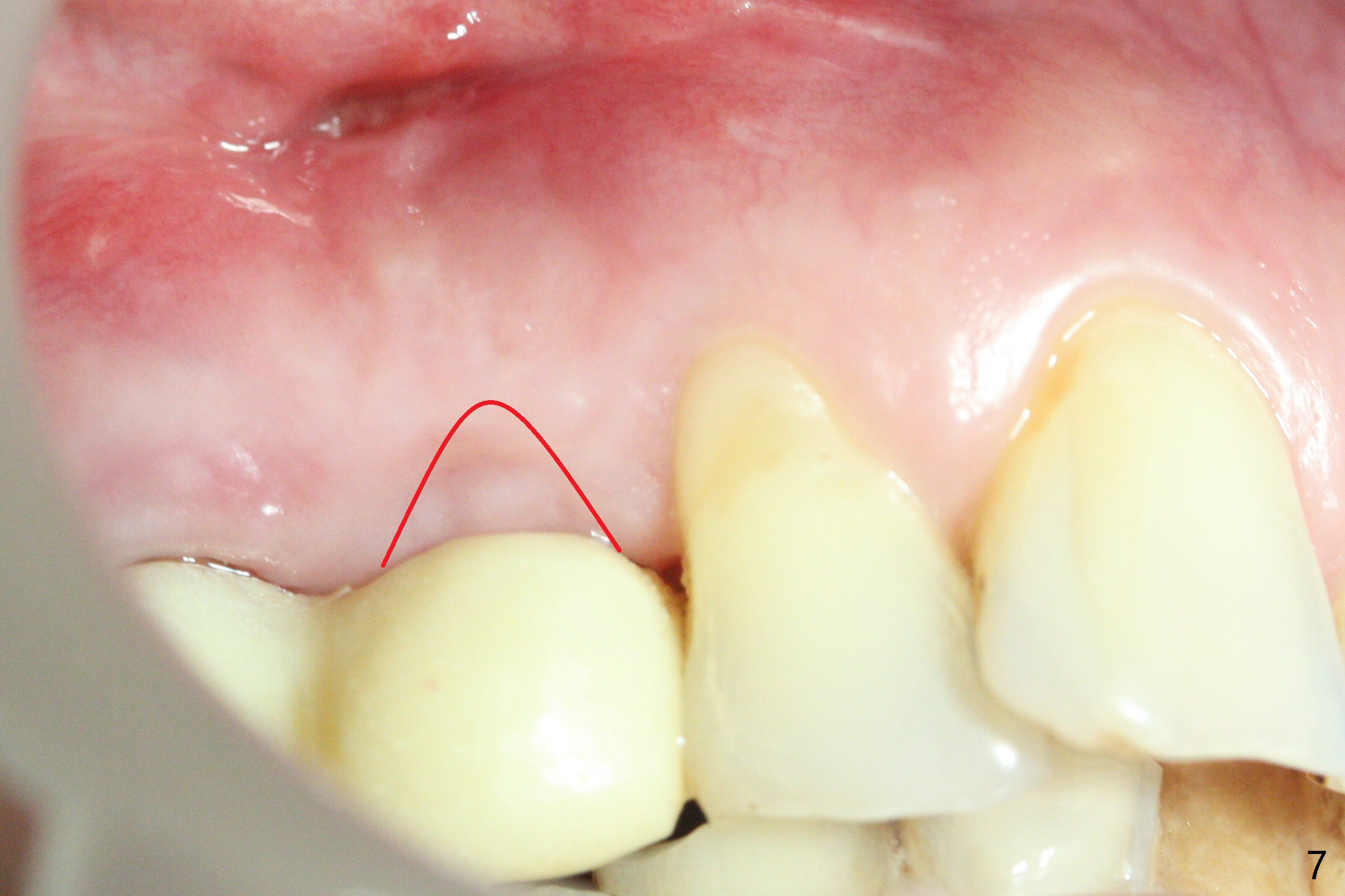
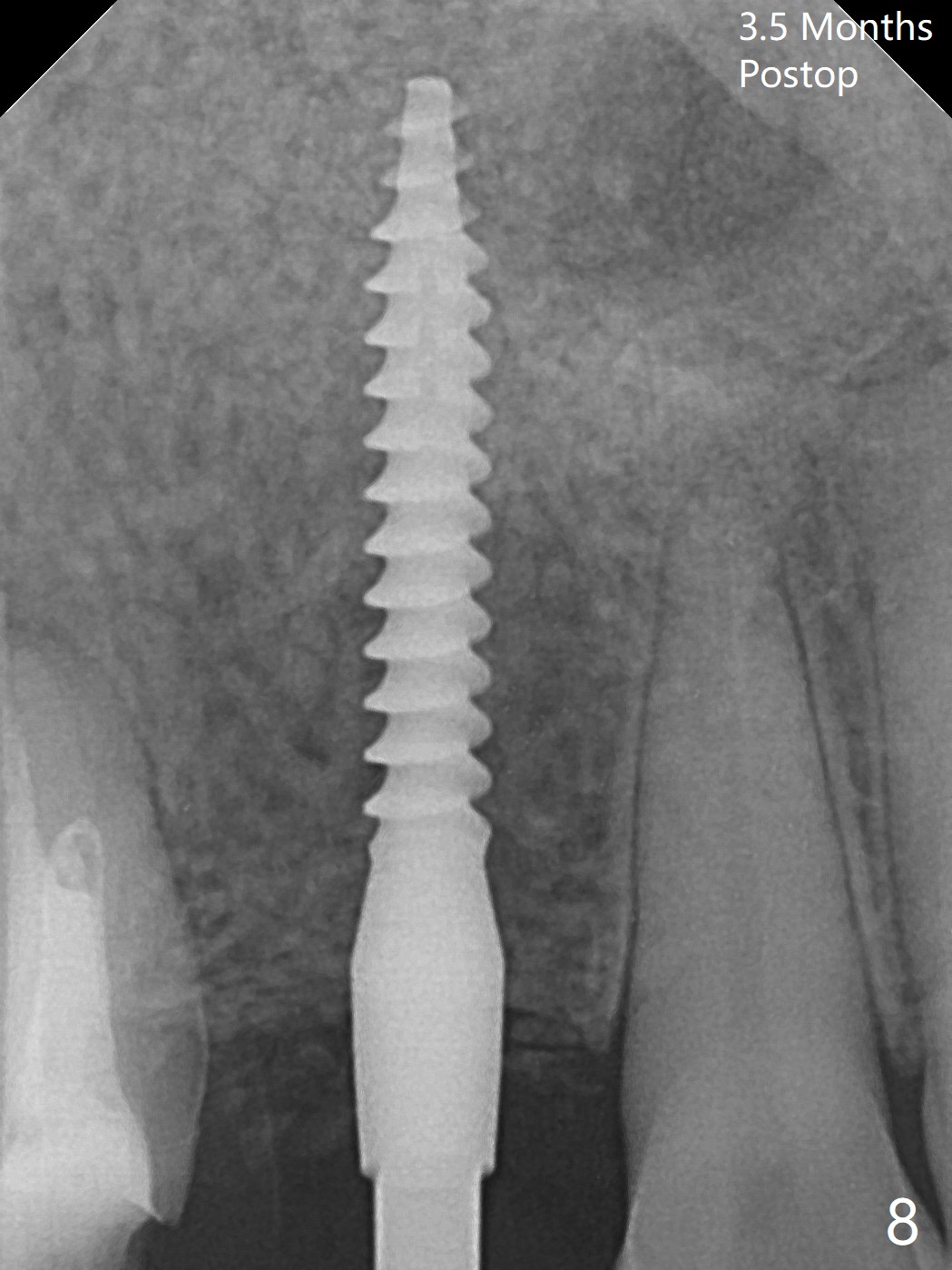
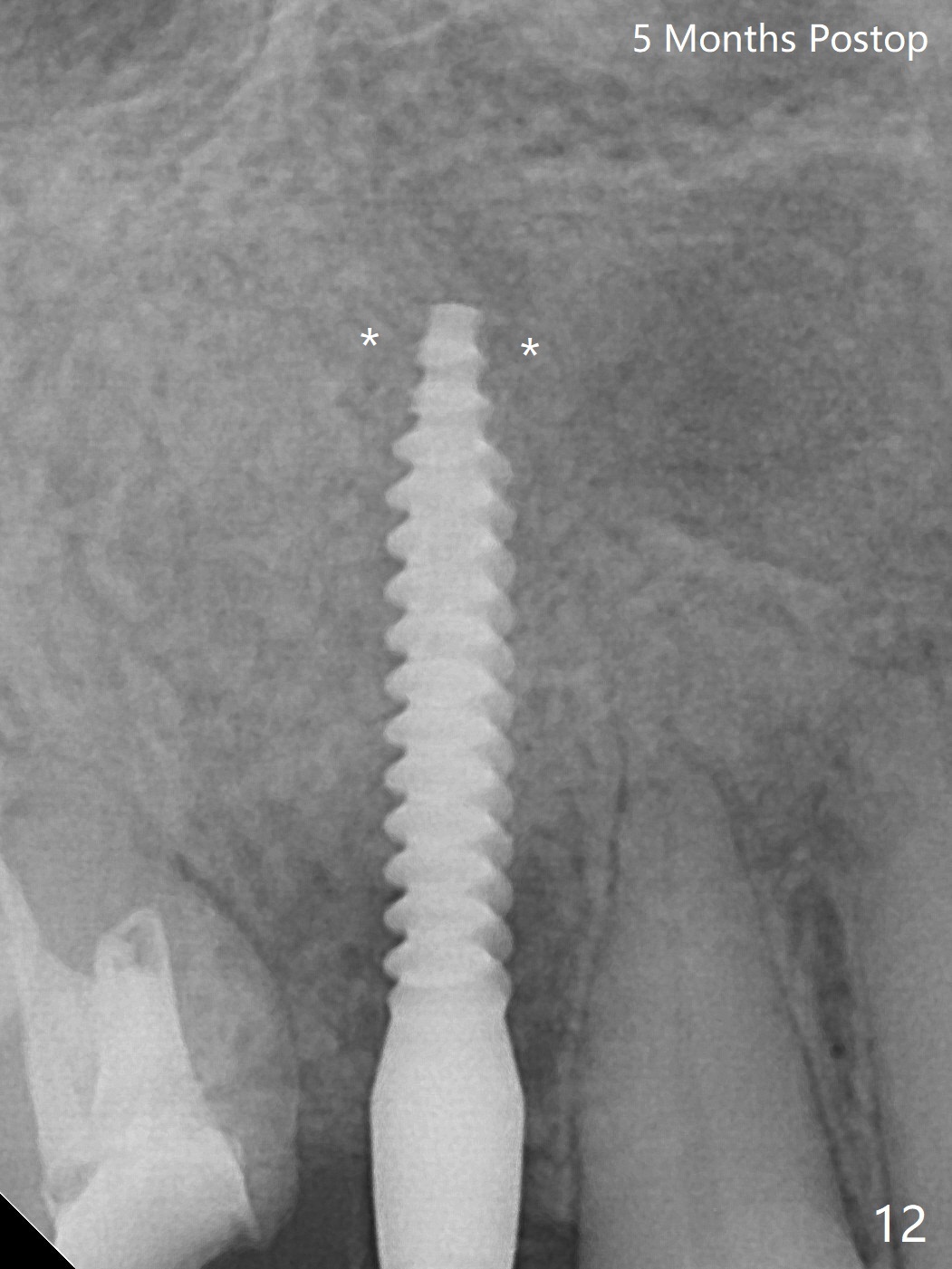
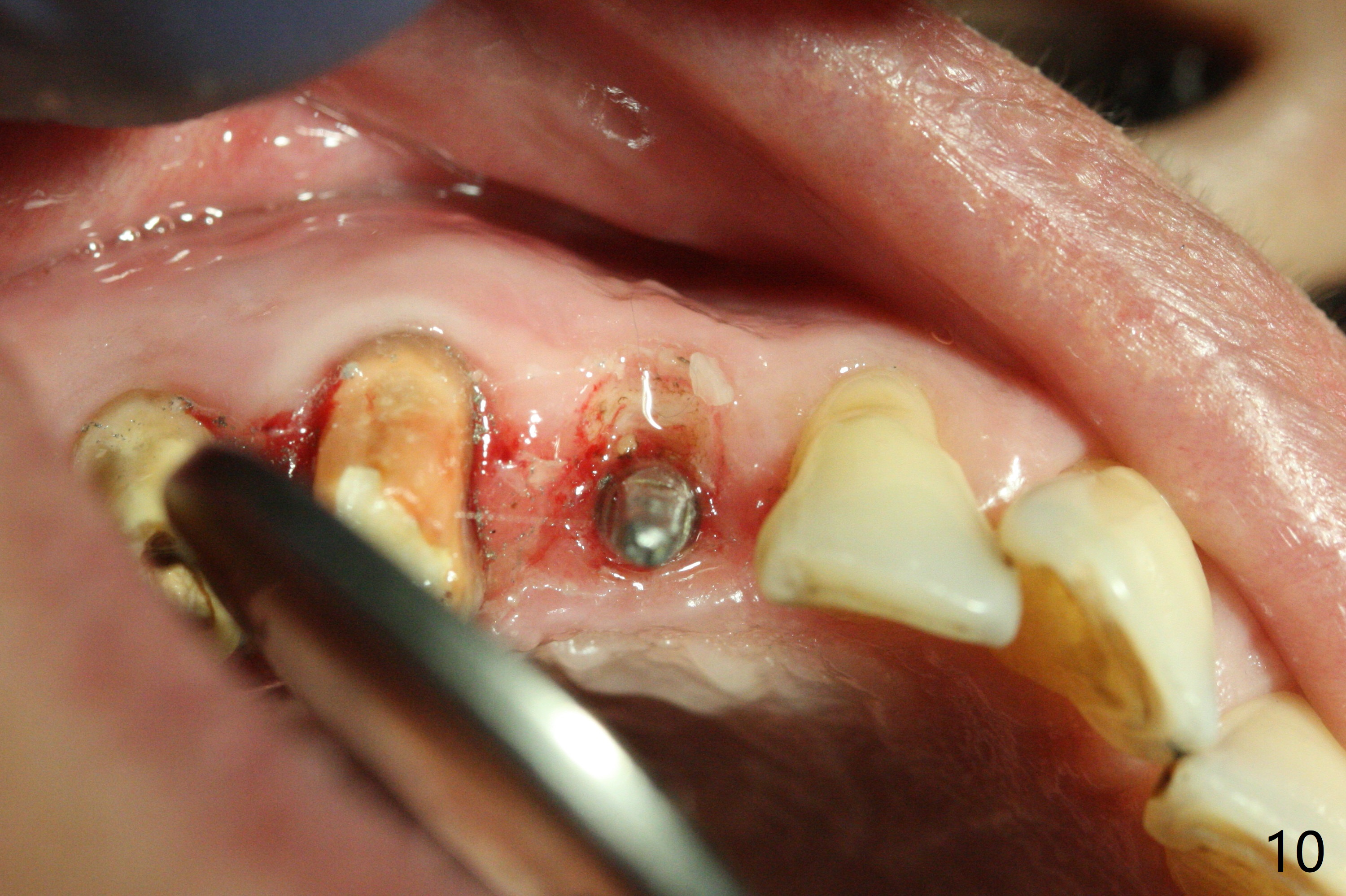
Osteotomy starts with guide and 2.2 mm drill for initial 3.5 mm palatal. A semilunar incision is made buccal to remove the impacted canine (#6 by sectioning). With direct vision buccal and palatal, the final osteotomy is finished free hand with 1.2 and 1.5 mm drills. Initially buccal perforation occurs, the osteotomy route is corrected later (Fig.1). When a 2.5x15 mm 1-piece implant is being placed, it perforates into the buccal concavity again. After redirection, the trajectory seems to be acceptable (Fig.2: CT coronal section). Three coronal implant threads are exposed partially palatal (Fig.3: CT 3-D palatal view). The implant is then turned 2-3 times with insertion torque reaching 40 Ncm. The incision is closed with suture following Osteogen plug placed in the most coronal portion of the socket (Fig.4 P) and allograft (*) in the remaining socket around the apical portion of the implant as well as palatal. The incision does not heal 1 month postop (Fig.5). PRF membrane will be placed next visit. Next visit the wound in fact is healing (Fig.6). PRF is unnecessary. The patient will return for impression 3 months postop. To be cosmetically pleasing, prepare local anesthetic and Laser for gingivectomy (Fig.7 red curved line). There is no bone loss around the implant 3.5 months postop (Fig.8). With topical, minor gingivectomy with laser creates papillae mesial and distal to the implant (Fig.9, 10 (incisal view)). After reline, there is appearance of a canine (Fig.11). The patient returns for impression 5 months postop; there is bone around the apex of the implant (Fig.12 *). The hard and soft tissues remain healthy when final restoration is delivered (Fig.13,14). The buccal plate reforms and #6 socket heals 12 months postop (6 months post cementation, Fig.15).
Return to Upper Canine Immediate Implant Trajectory 2 15 Xin Wei, DDS, PhD, MS 1st edition 01/14/2019, last revision 01/24/2020