,%20not%20completely%20seated.jpg)
.jpg)
.jpg)




|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|||||
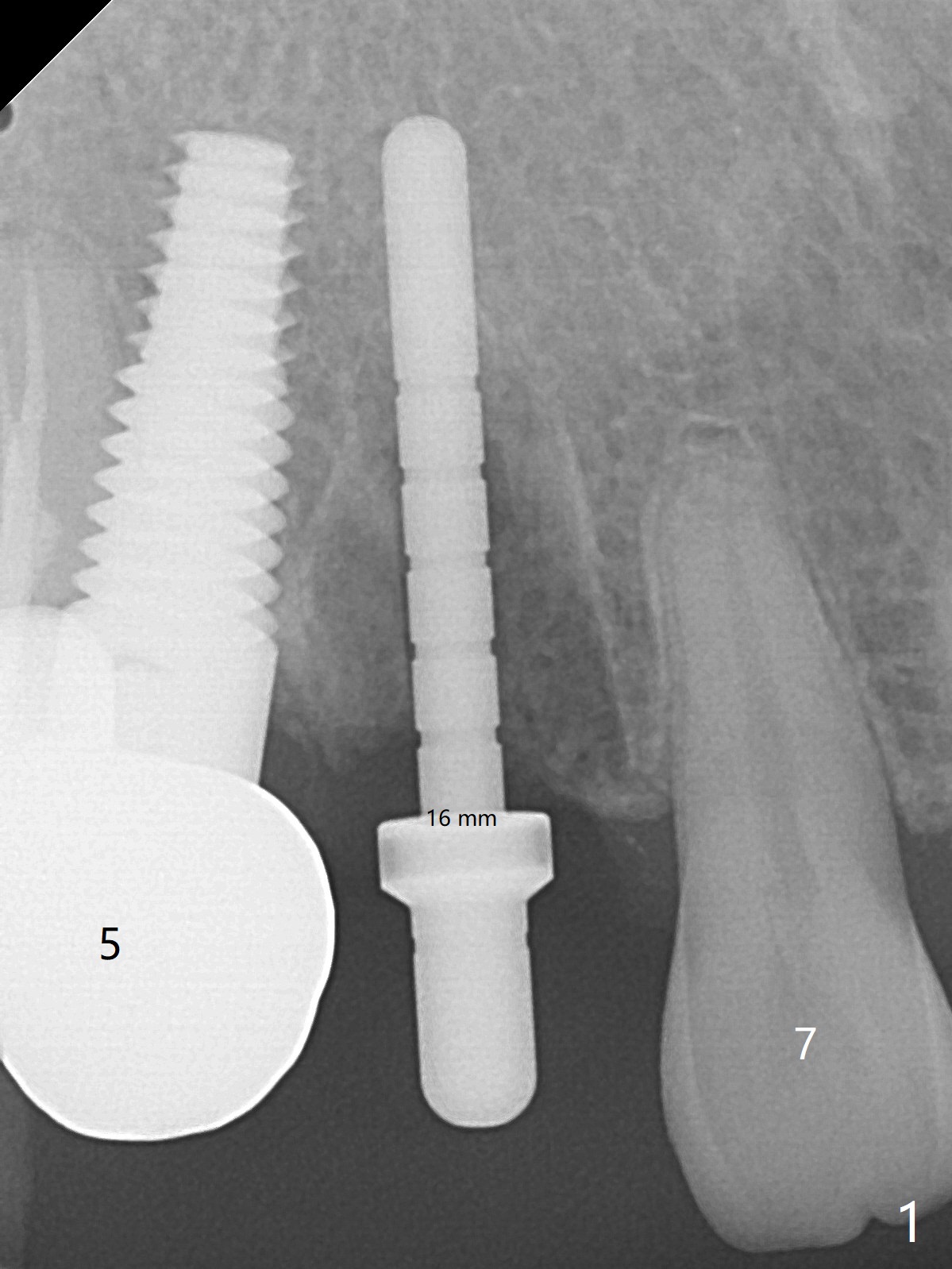
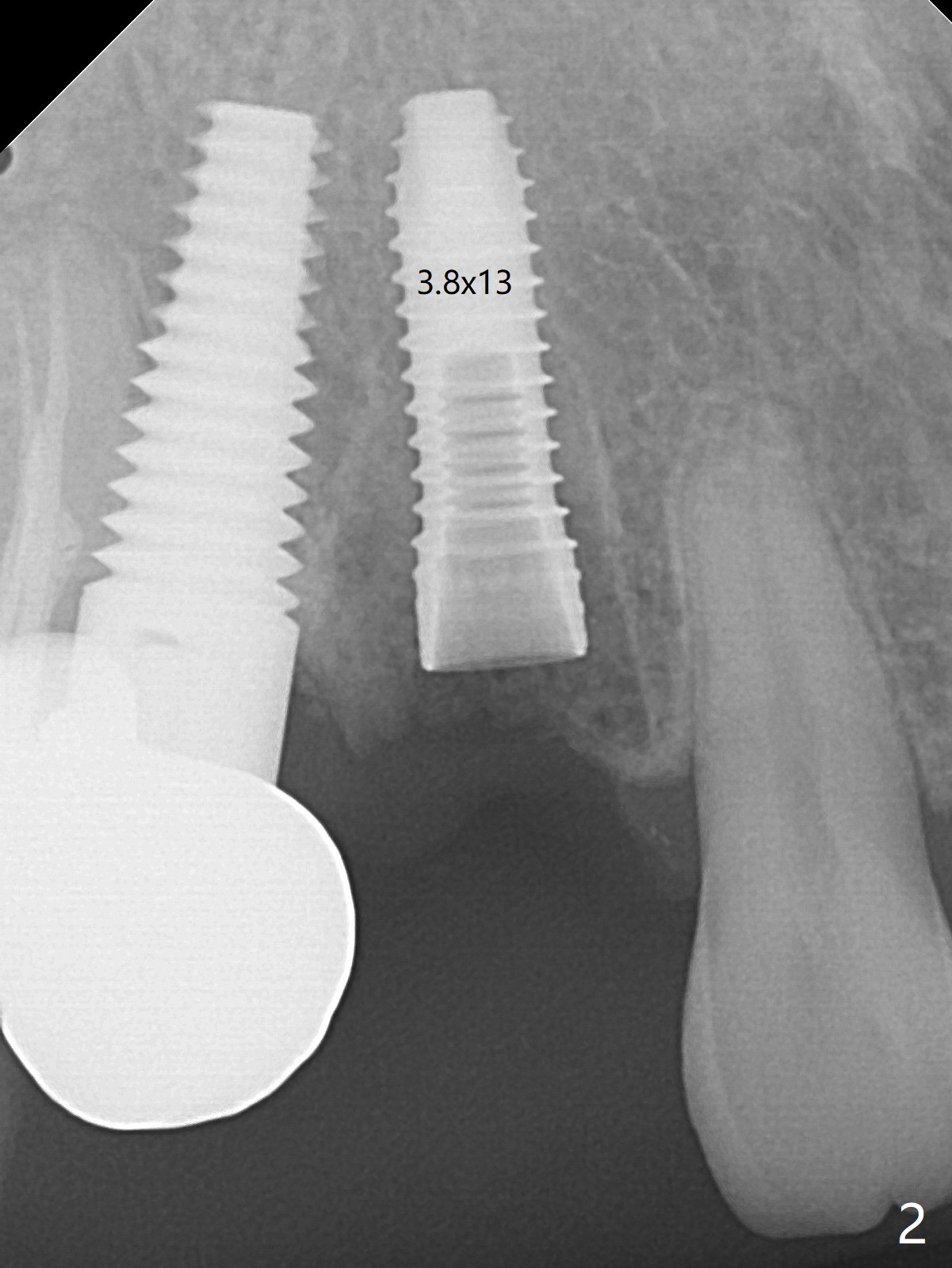
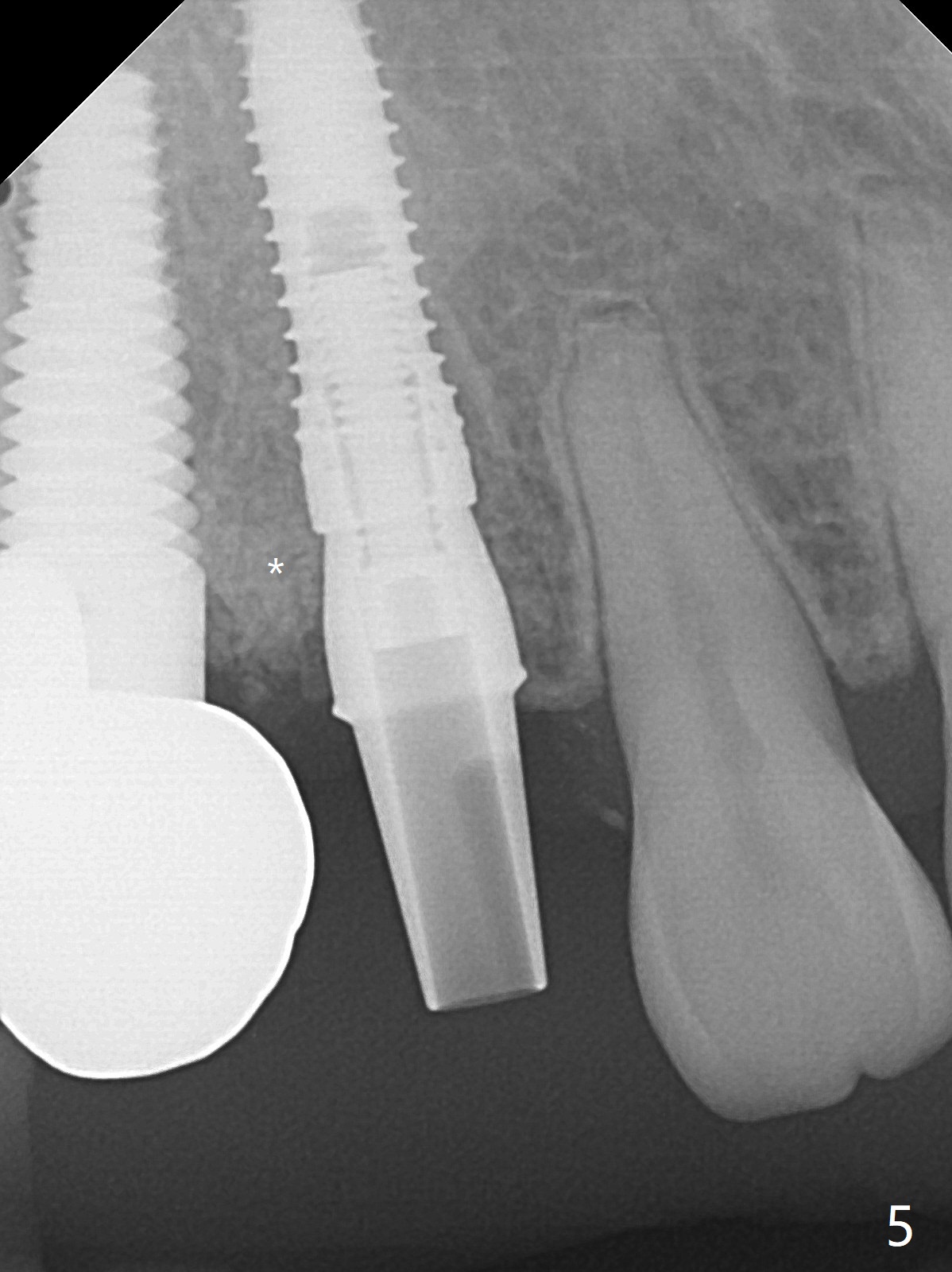
Fractured Post/Intact Socket
When the recemented crown at #6 is removed, the post is found to have been fractured. When the tooth is extracted, the socket walls are found intact. After moving the initial osteotomy (Fig.1) mesial, a 3.8x13 mm implant is placed (Fig.2). Clinically it appears supracrestal lingually. So the implant is placed deeper, but a cemented abutment is incompletely seated (Fig.3 <). When a longer abutment is used (easy grasping), it is seated completely (Fig.4). Then sticky bone is packed (Fig.5 *). When an immediate provisional is fabricated and seated, PRF membranes are inserted into the remaining gap between the gingiva and the provisional. Free hand surgery takes time and more intraop X-ray. It is inconvenient with nervous patients. The socket heals 2 weeks postop (Fig.6). The provisional will be next relined and reseated. It is difficult to insert gingival retraction cord 3.5 months postop because of the deep mesial margin. When an abutment with longer cuff is placed, the packing is easier (no biologic width violation, Fig.7 (^: resorbed mesial crest), as compared to Fig.5). When the crown is cemented (un-esthetic due to failure of use of temporary abutment), the metal shows at #5 with gingival recession because of buccal placement (Fig.8-10). Bone resorption is severe between #5 and 6 (Fig.7), as related to large gingival embrasure (Fig.9 *). When #5 crow is redone, move the gingival margin apical and fabricate provisional.
Return to
No Deviation
Xin Wei,
DDS, PhD, MS 1st edition 07/17/2020, last revision
11/20/2020