.jpg)
.jpg)








|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|||
|
|
|
||||
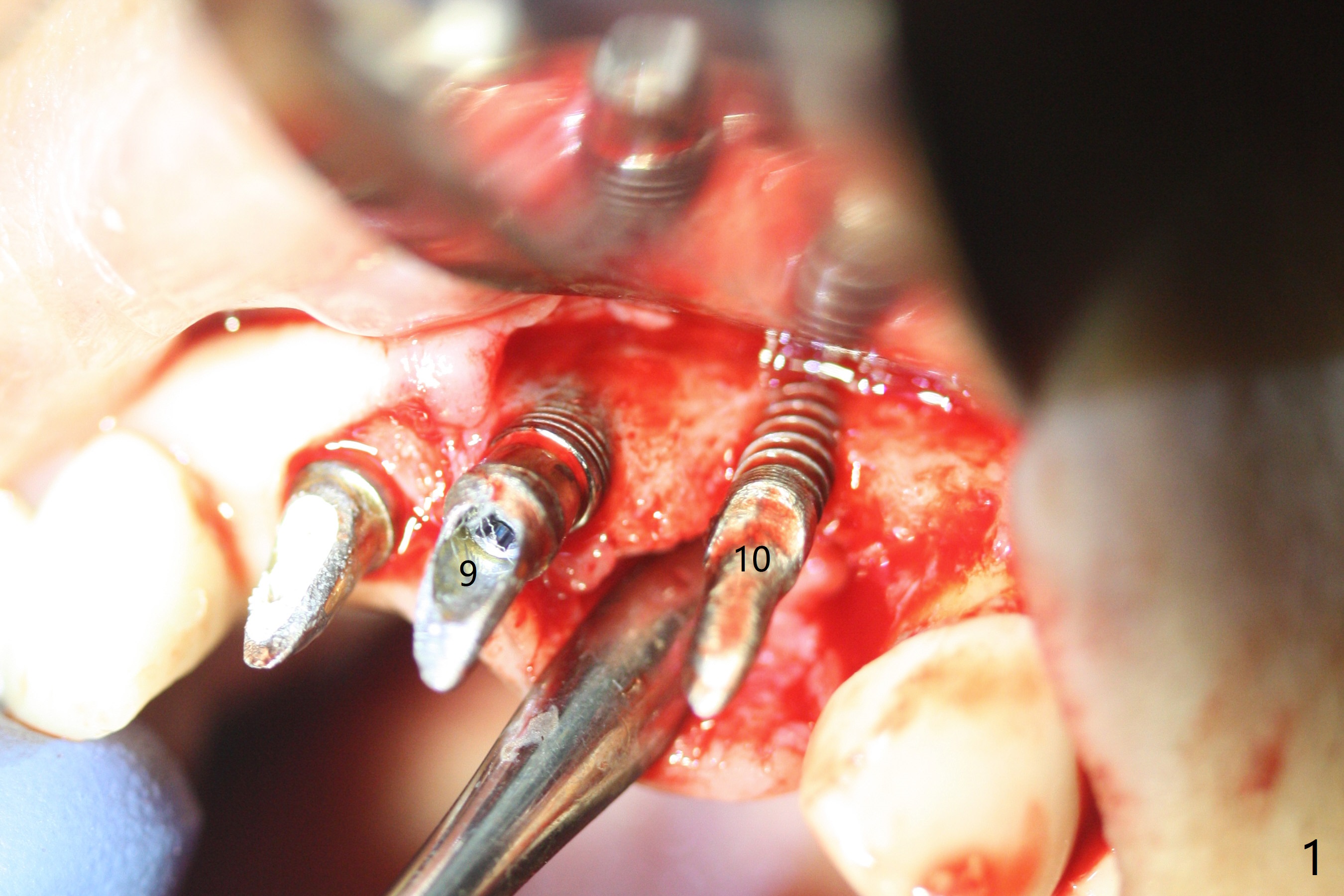
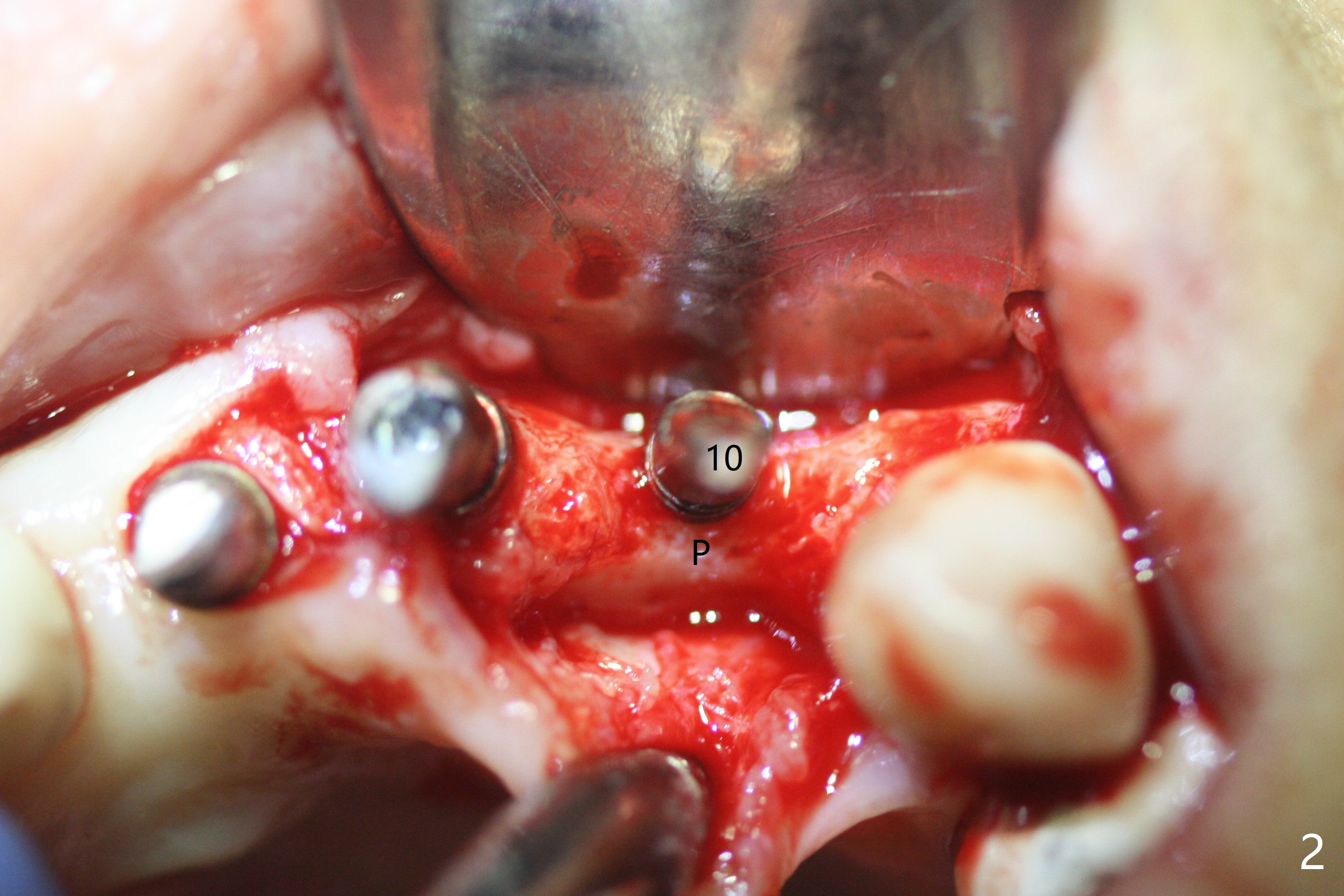
Guided/Free Hand Immediate Re-Placement I
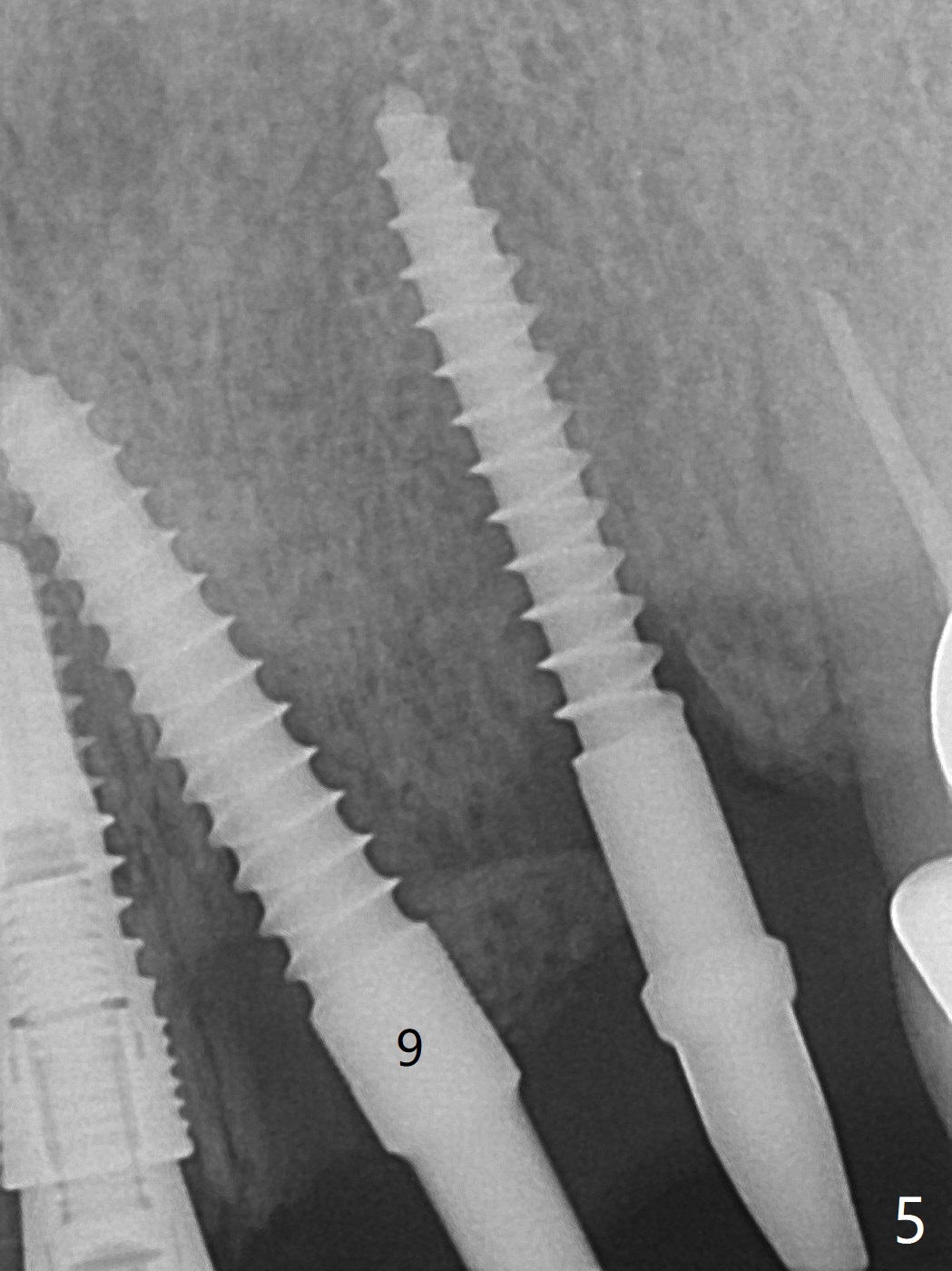
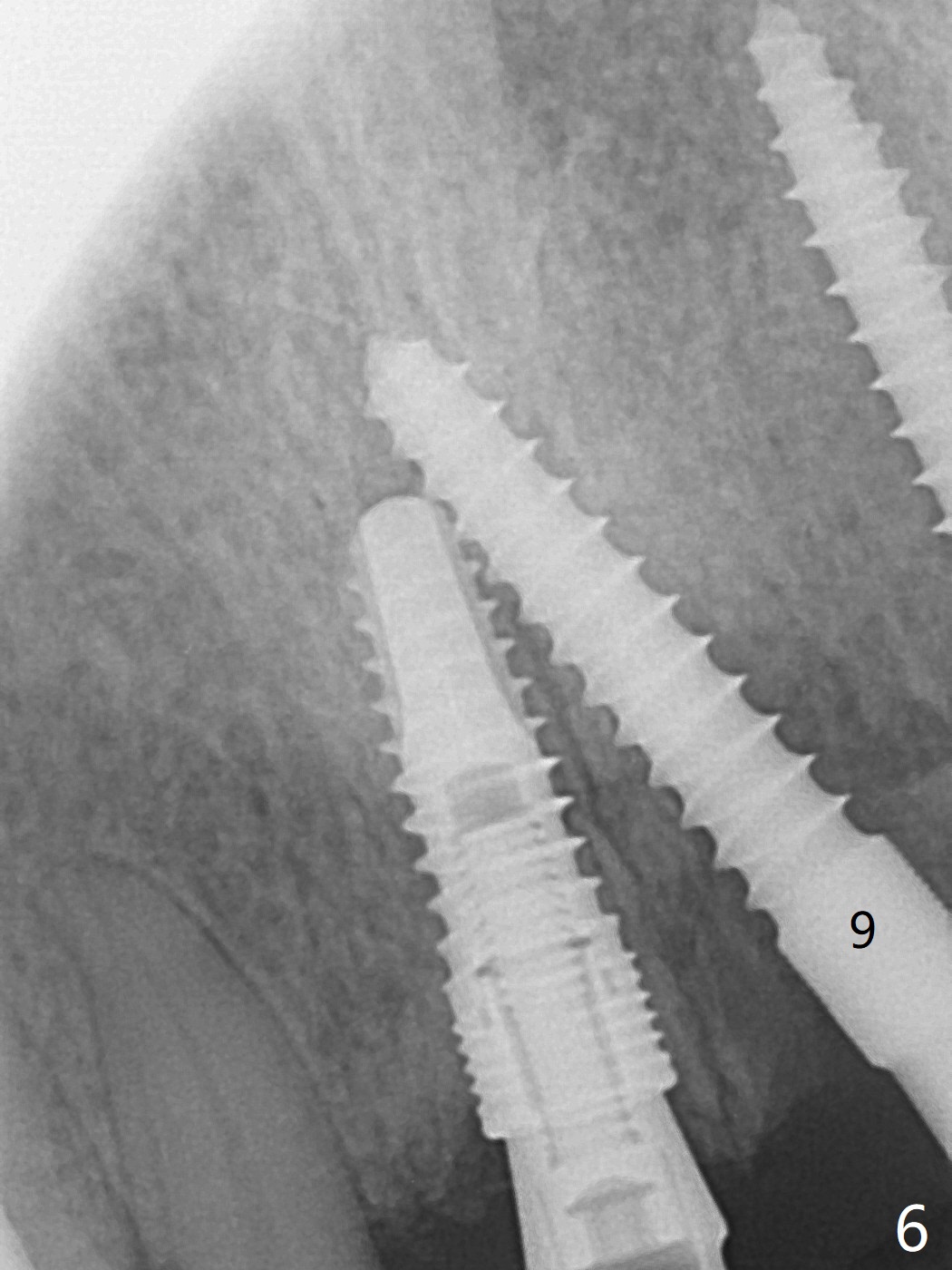
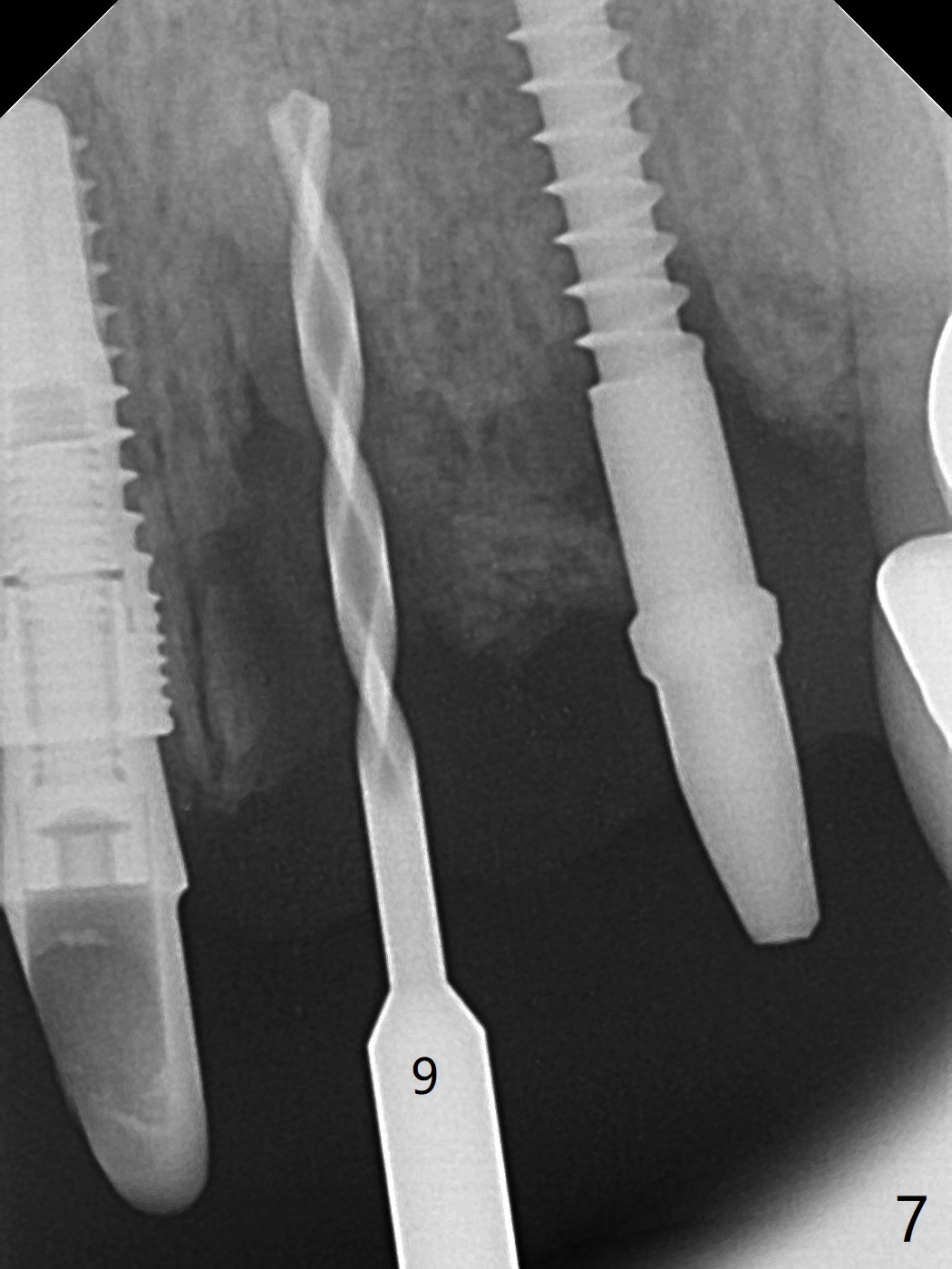
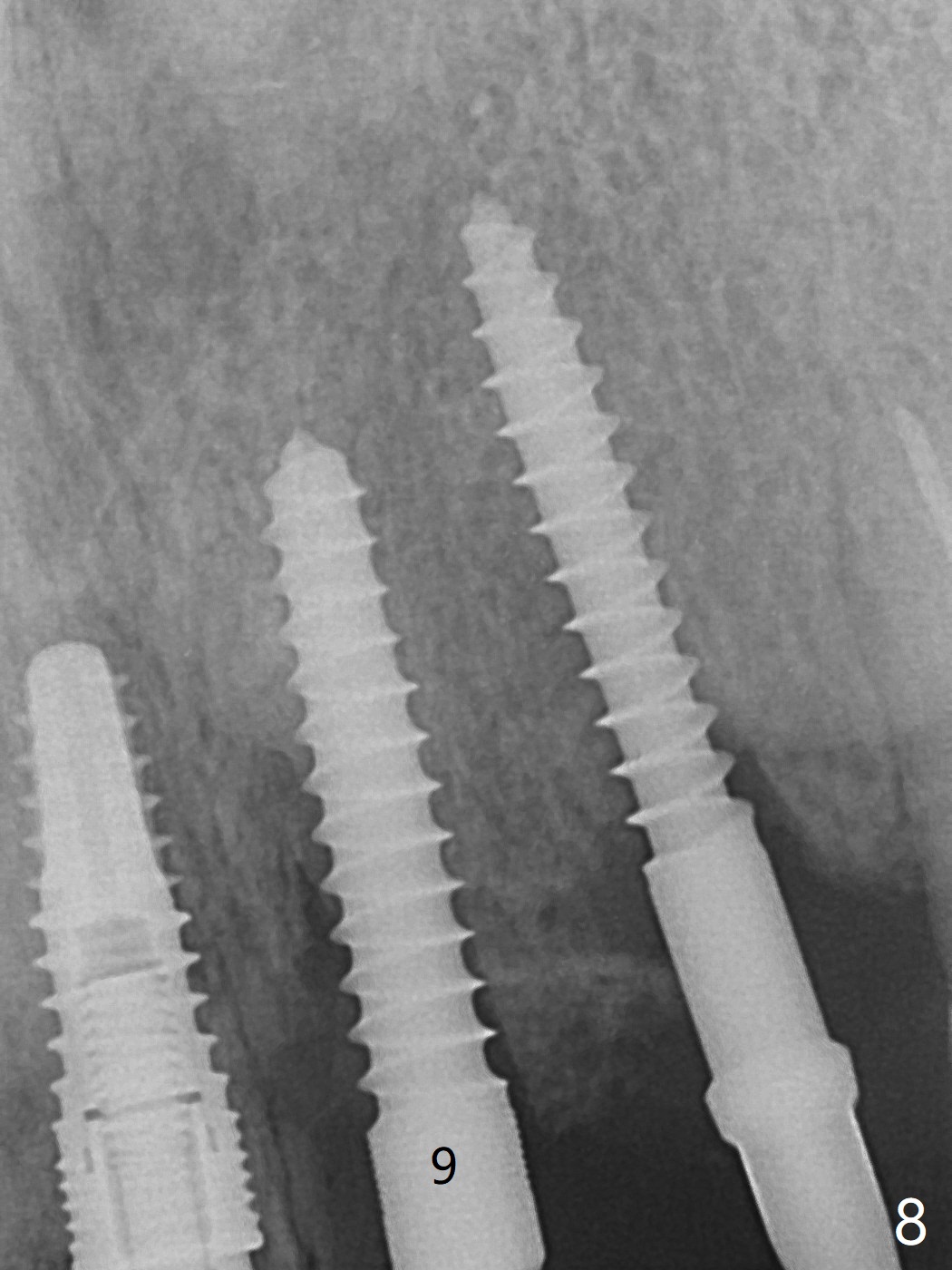
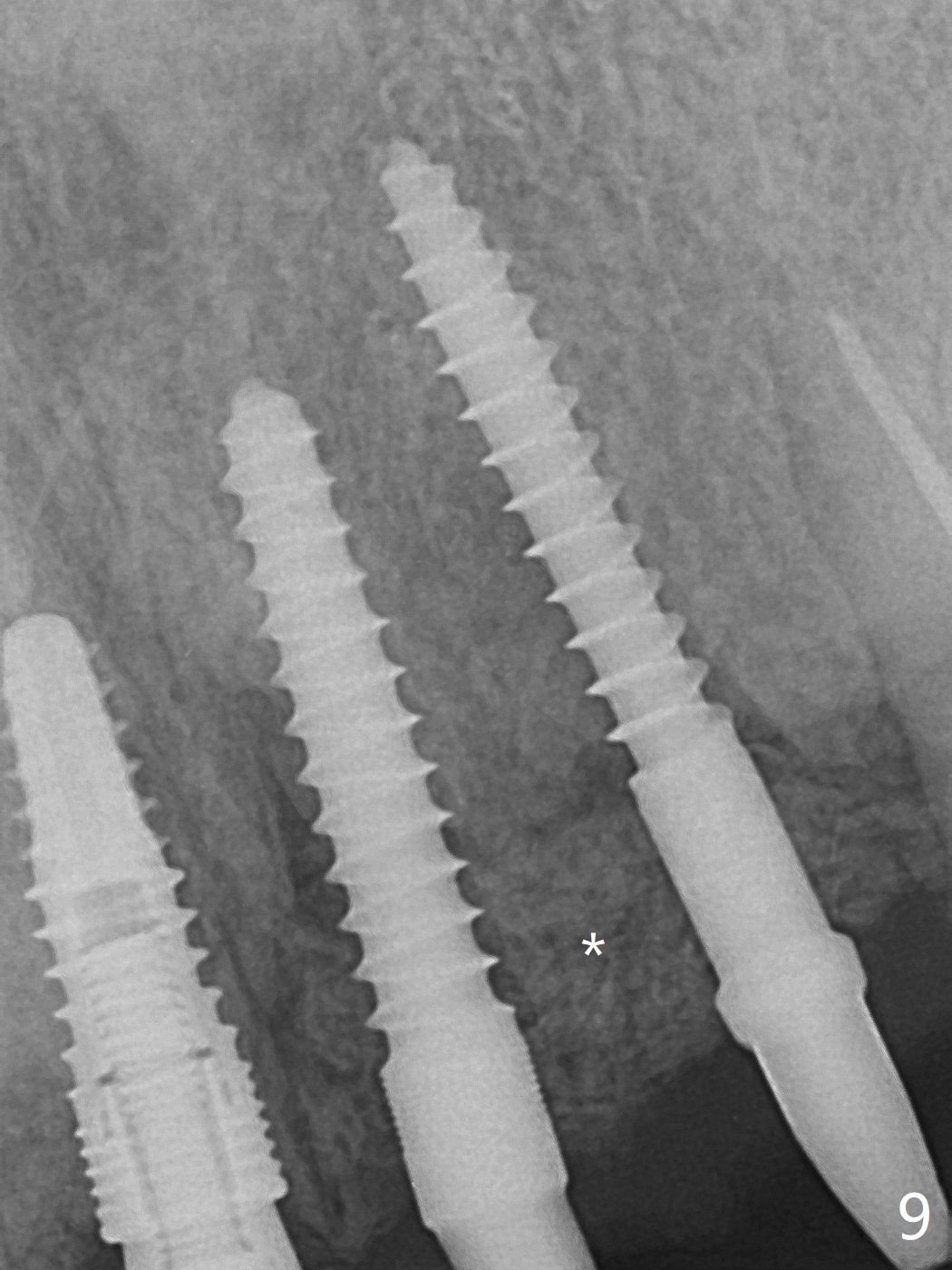
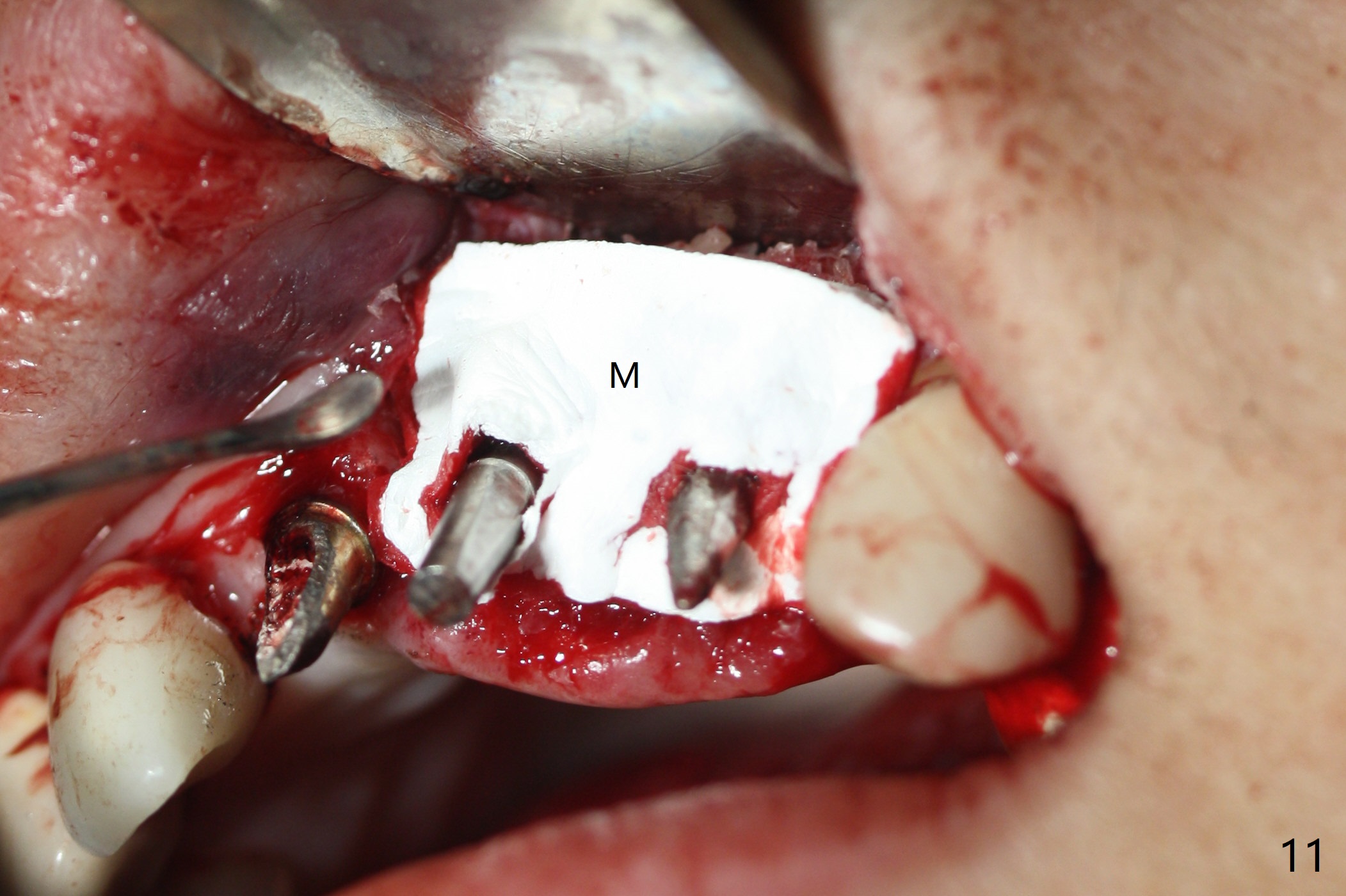
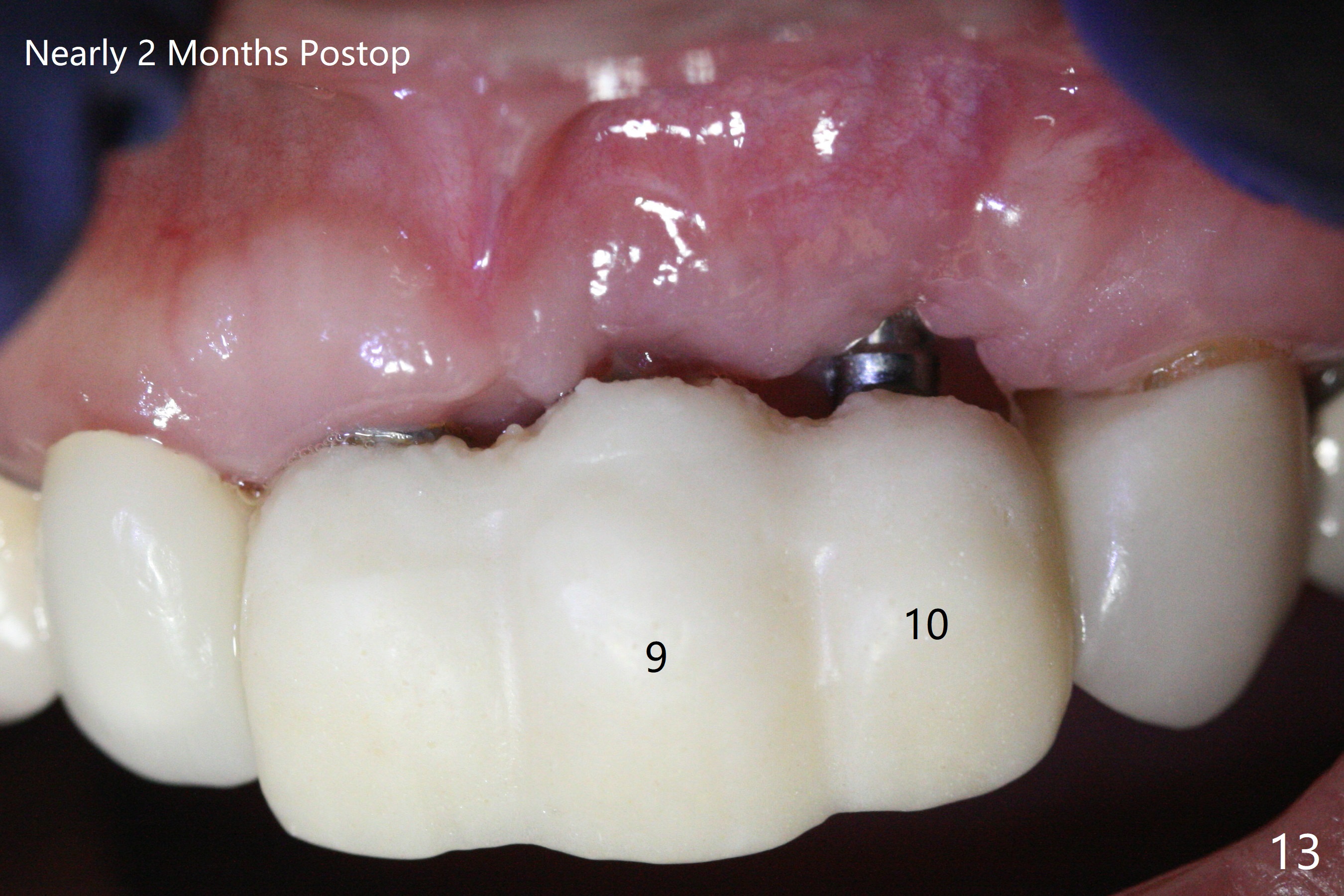
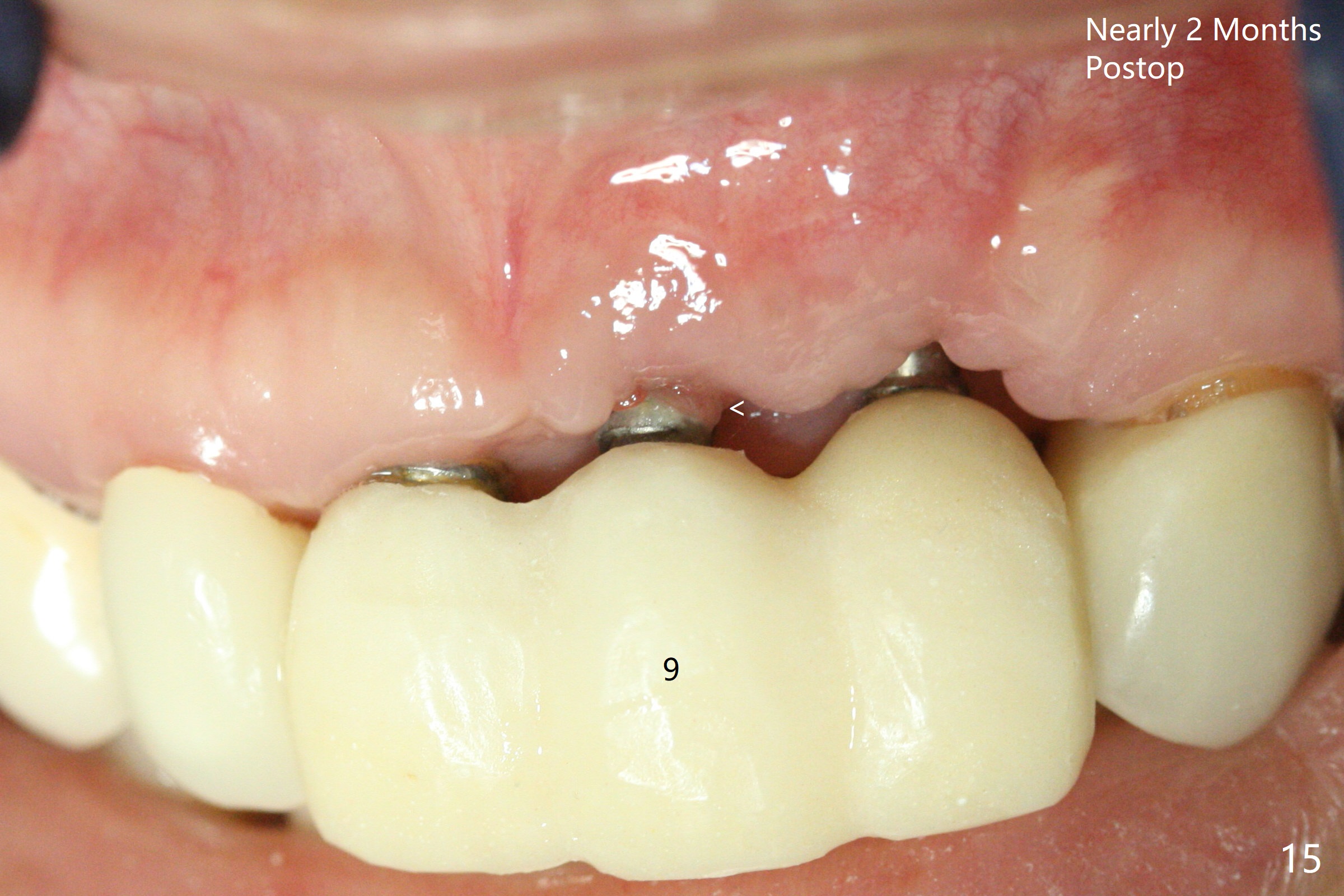
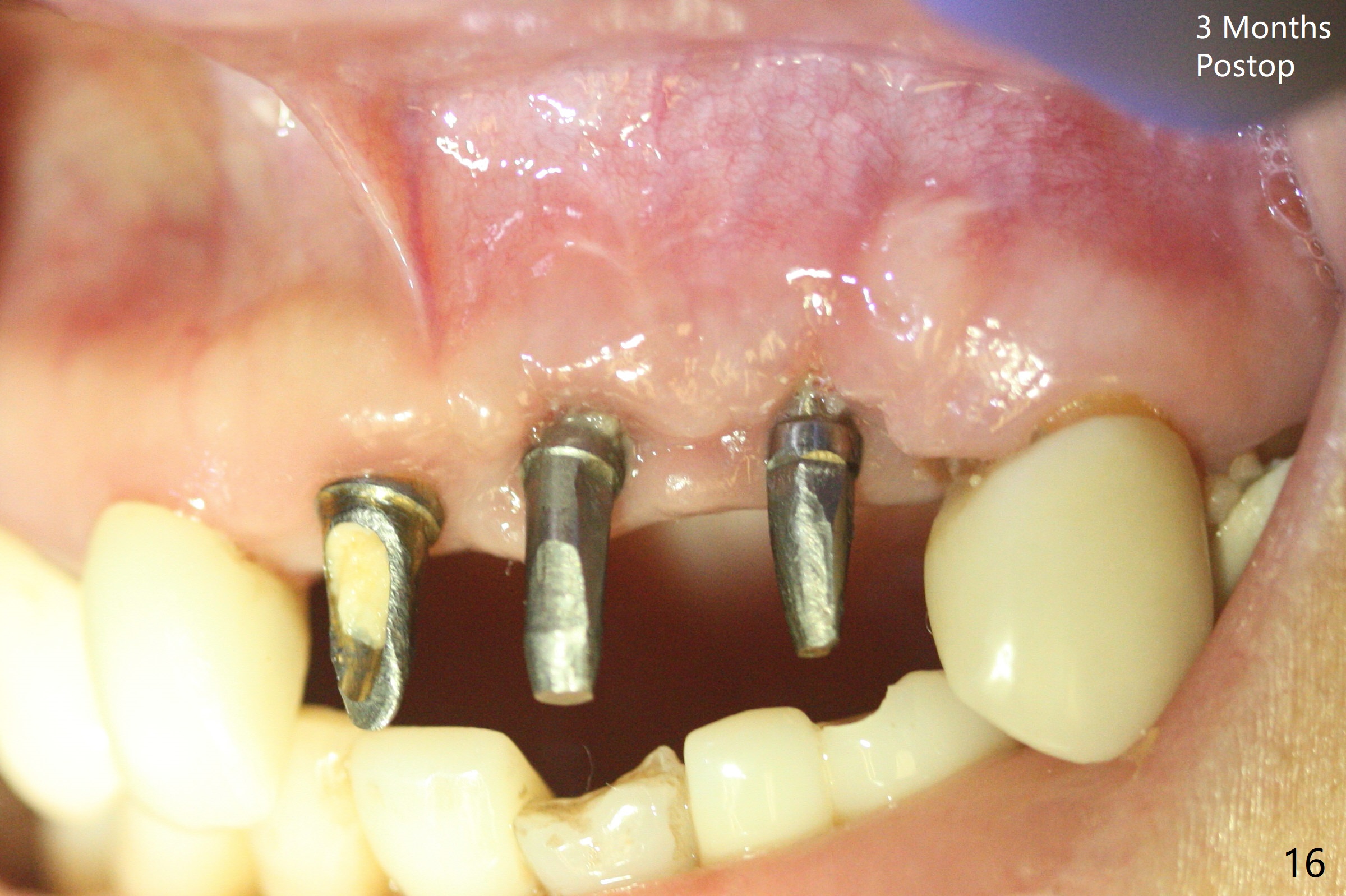
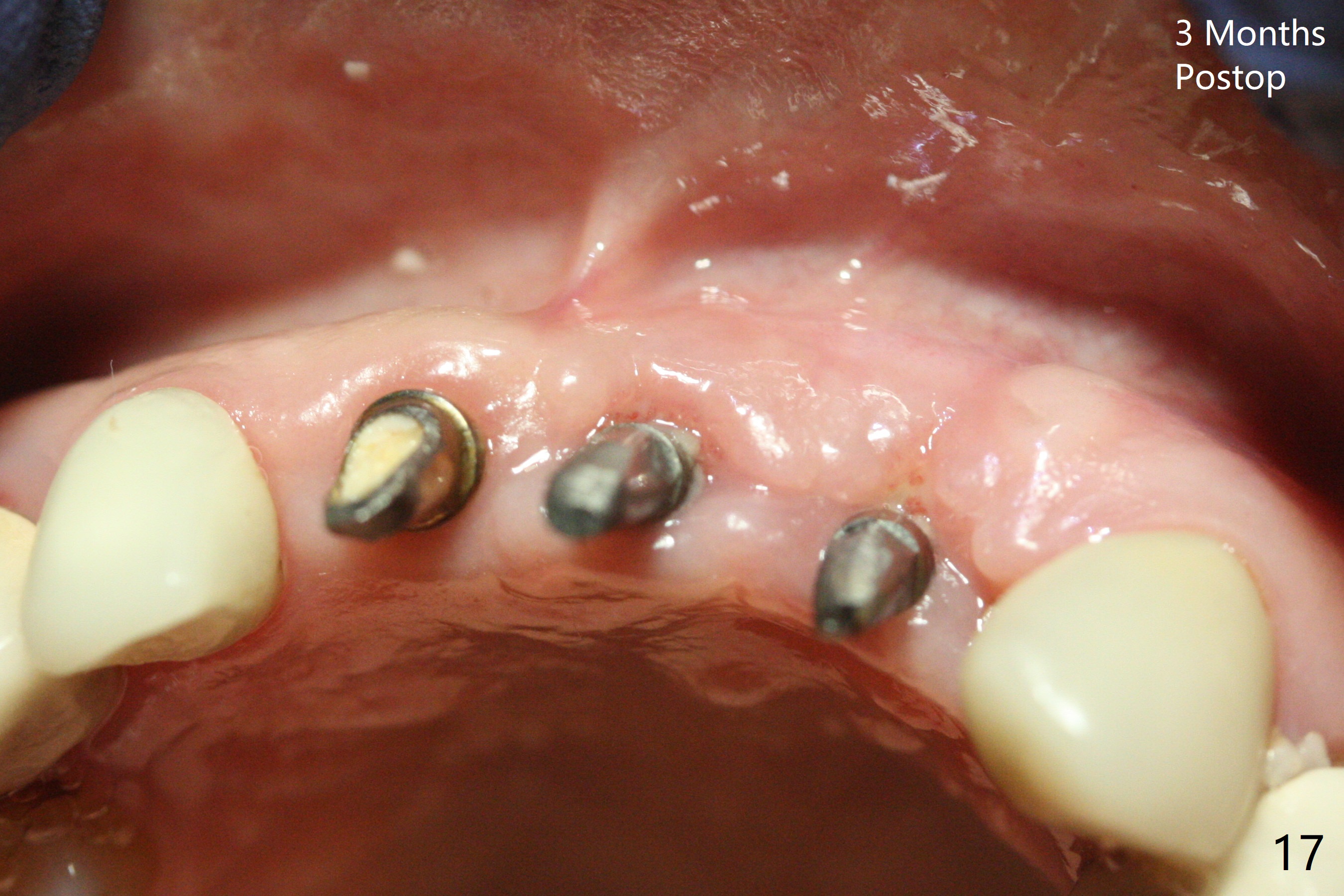
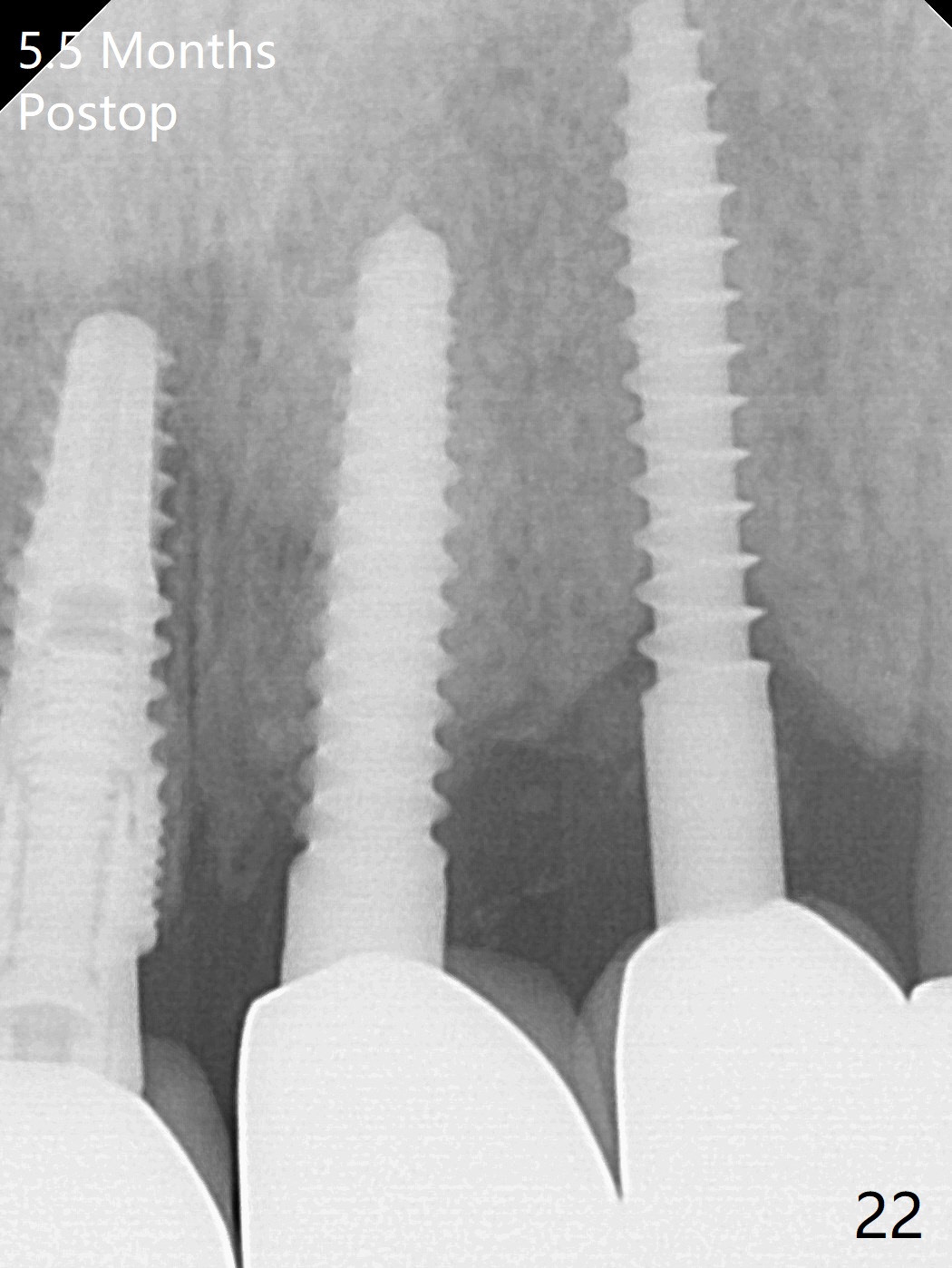
Incision shows exposure of microthreads at #9 and major threads at #10 due to buccal placement (Fig.1). There is bone palatal to the implant at #10 (Fig.2 P), to which a new implant will move. After implant removal, a narrower 1-piece implant (2.5x14(4) mm) is placed palatally at #10 (Fig.3,4) in combination of guide and free hand. At the site of #9 after implant removal, the guide is not used; a 3x17 mm angled 1-piece implant is placed with bad trajectory (Fig.5,6). After re-adjustment (Fig.7), the implant is placed at the right orientation (Fig.8). It appears that the guide is helpful. Allograft is placed mainly buccally (Fig.9,10 *), followed by a piece of collagen membrane (Fig.11). After tension release, flaps are approximated (Fig.12). The buccal gingiva at #9 and 10 recede nearly 2 months postop (Fig.13). Less recession at #9 is associated with more inflammation (Fig.14). The margin of the provisional is adjusted for gingival margin down growth and easy self cleaning with Water Pik (Fig.15). One month later, the gingival inflammation reduces, while there is no obvious buccal collapse (Fig.16,17). Impression is taken after laser gingivectomy nearly 4 months postop (Fig.18). While the gingiva around the implant at #9 is inflamed (periimplantitis?), the gingival cuff at #10 is well formed 5.5 months postop immediately before cementation (Fig.19). The buccal concavity at #10 is minimal (Fig.20). The gingival inflammation at #9 will be hopefully resolved after cementation of the final restorations (Fig.21). There appears to be new bone formation around the coronal implant threads 5.5 months postop (immediately post cementation, Fig.22). The microthreads at #9 may be not covered by the bone, the reason for the gingival erythema. The redness at #10 is asymptomatic 5.5 months post cementation (Fig.23).
Return to
Upper Incisor Immediate Implant,
Trajectory
18-20
Xin Wei, DDS, PhD, MS 1st edition
01/18/2019, last revision
02/01/2020