
|
|
|
|
|
|
|
|
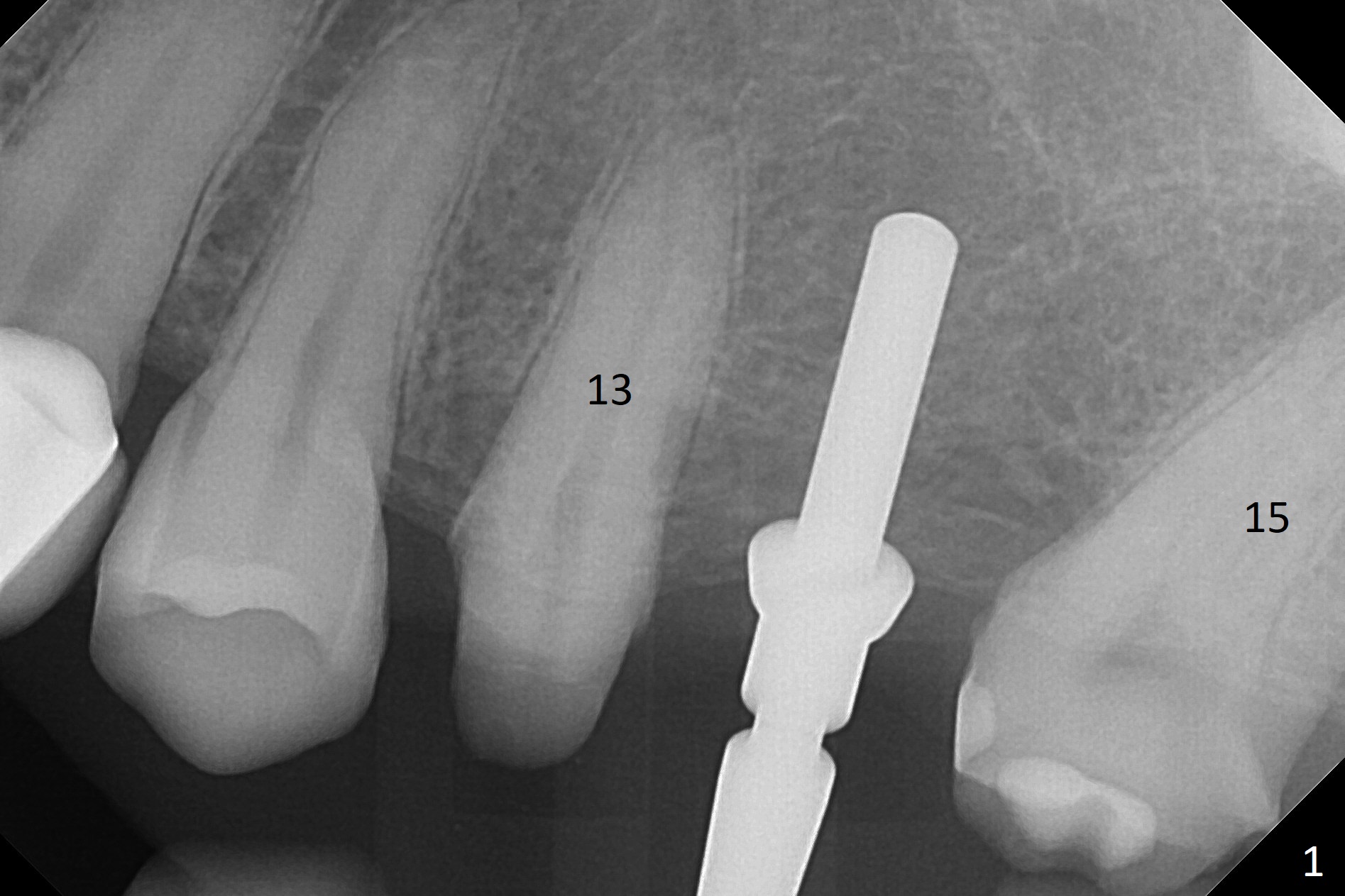
What is Wrong with FPD?
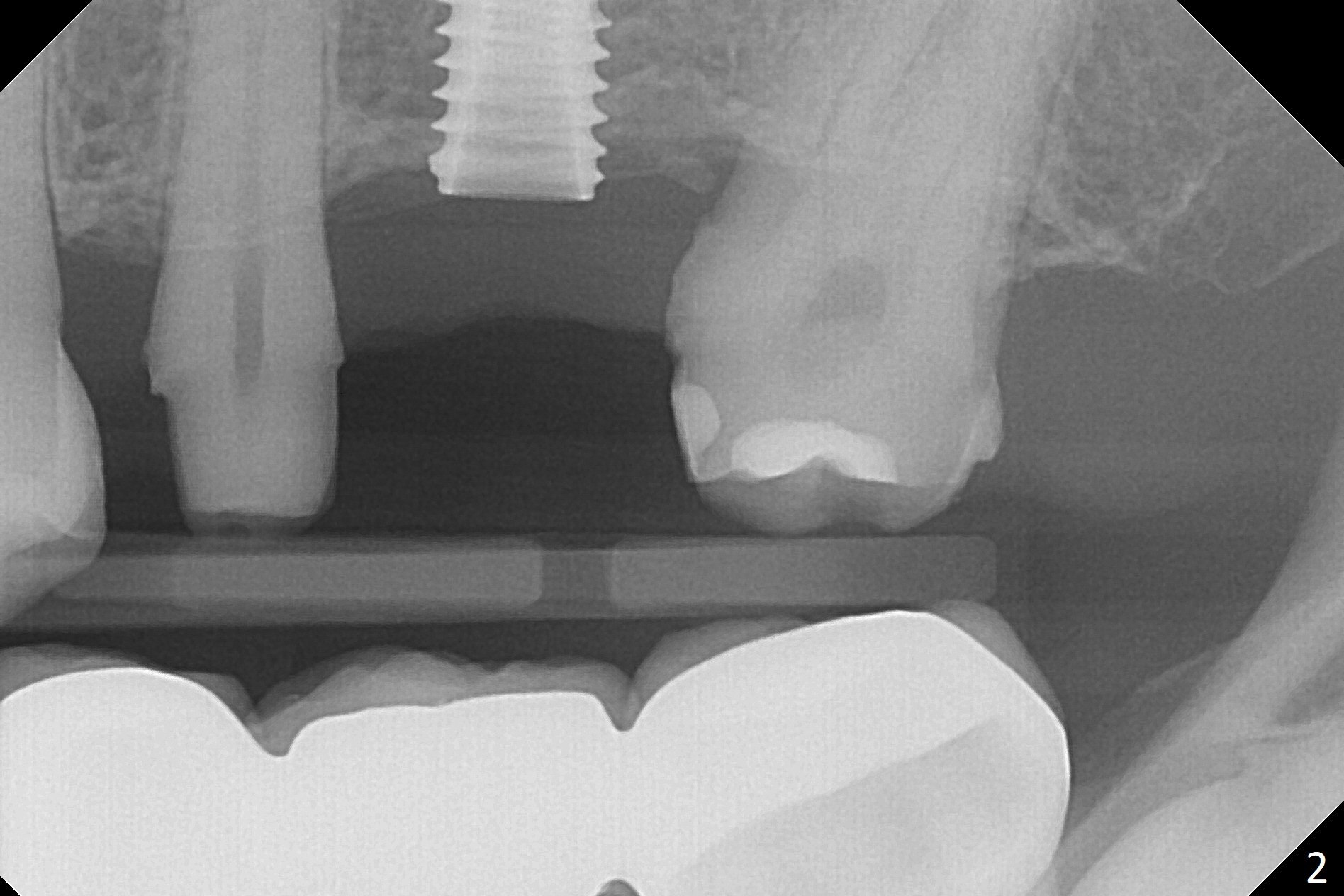
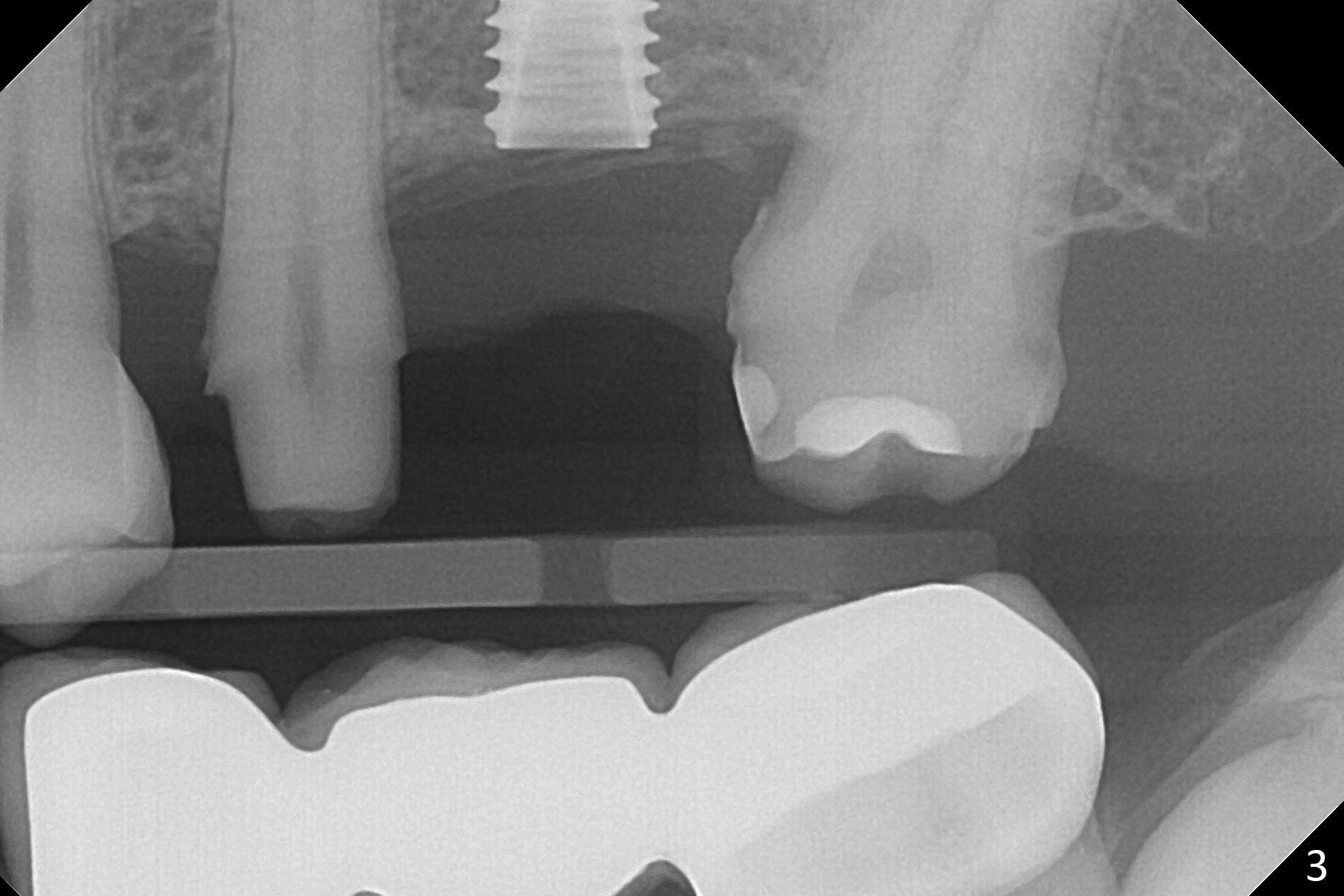
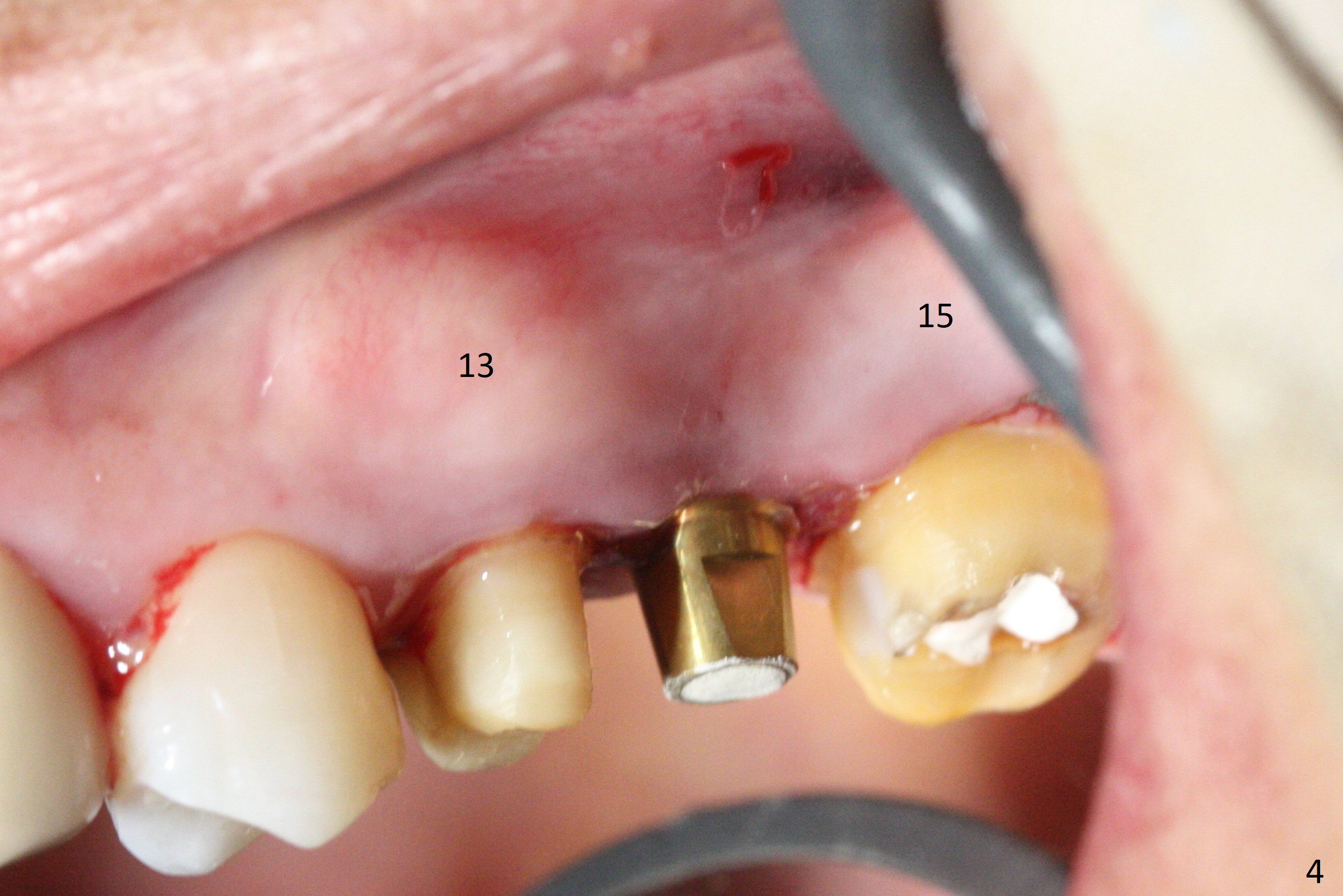
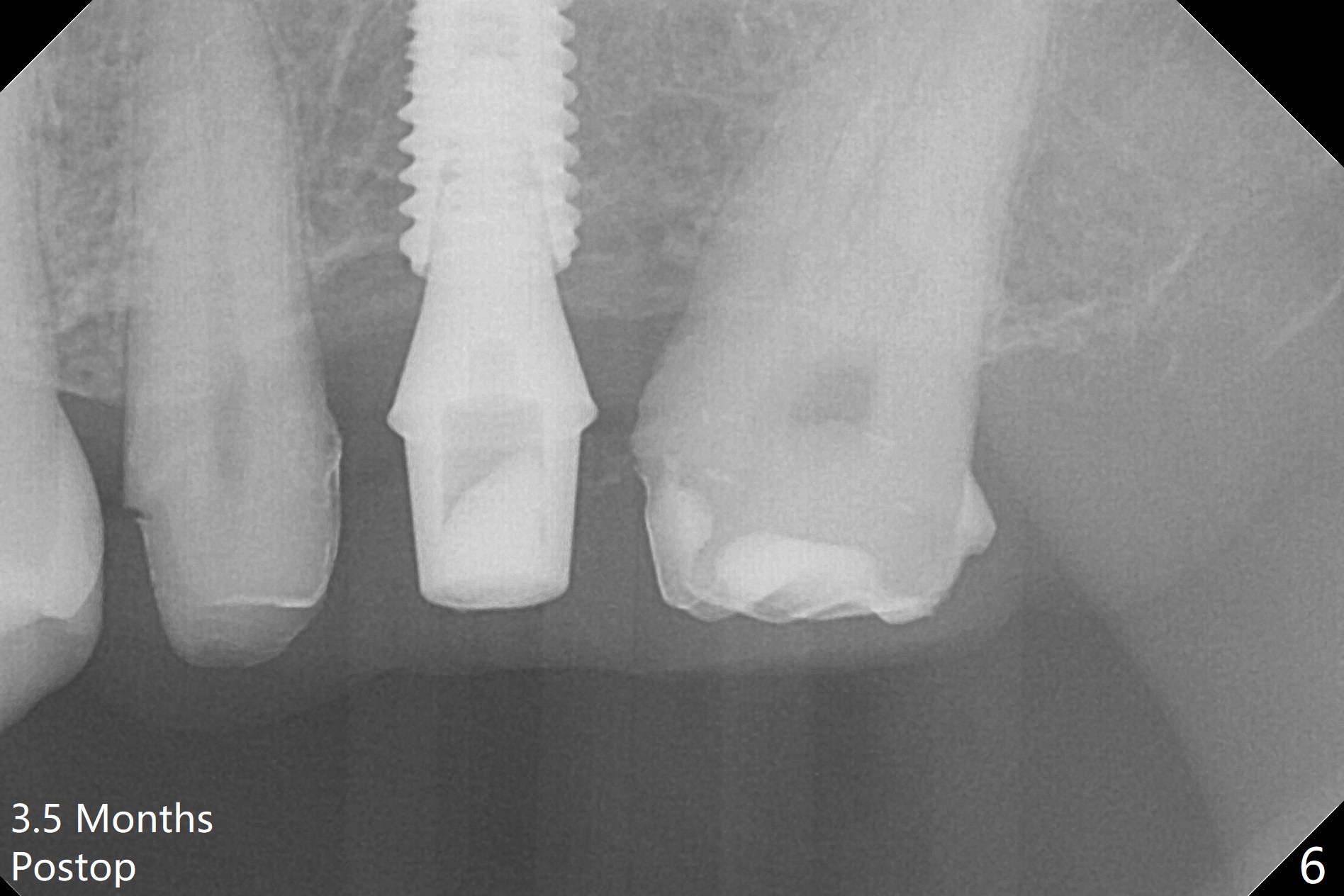
#13-15 FPD has not been used properly because of discomfort for 2 years. Before its removal, the discomfort derives from probing of the distal of #13 and mesial of #15, corresponding to calculus in the proximal areas. SRP is performed in UL quadrant after FPD removal. Bone density at the crest of the edentulous area is normal, while that of the medulla is low. After determination of trajectory and depth of initial osteotomy (Fig.1 (5 mm straight incision)), the site is underprep for a 4.5x13 mm Implant. Following adjustment, the implant is placed slightly subcrestal (Fig.2,3). It is possible that the discomfort of the previous FPD is due to overload, as suggested by the prominent buccal plate at #13 and 15, as compared to that of #12 (Fig.4 (5.2x4.5(3) mm cementation abutment at #14). Postop follow up shows that the tooth #15 may need RCT. The implant seems to enter the sinus (Fig.5 (2.5 months postop)) and be ready for restoration 3.5 months postop (Fig.6).
Return to Upper Molar Immediate Implant, Armaments Xin Wei, DDS, PhD, MS 1st edition 12/08/2017, last revision 09/02/2018