.jpg)
,%20Vera.jpg)



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
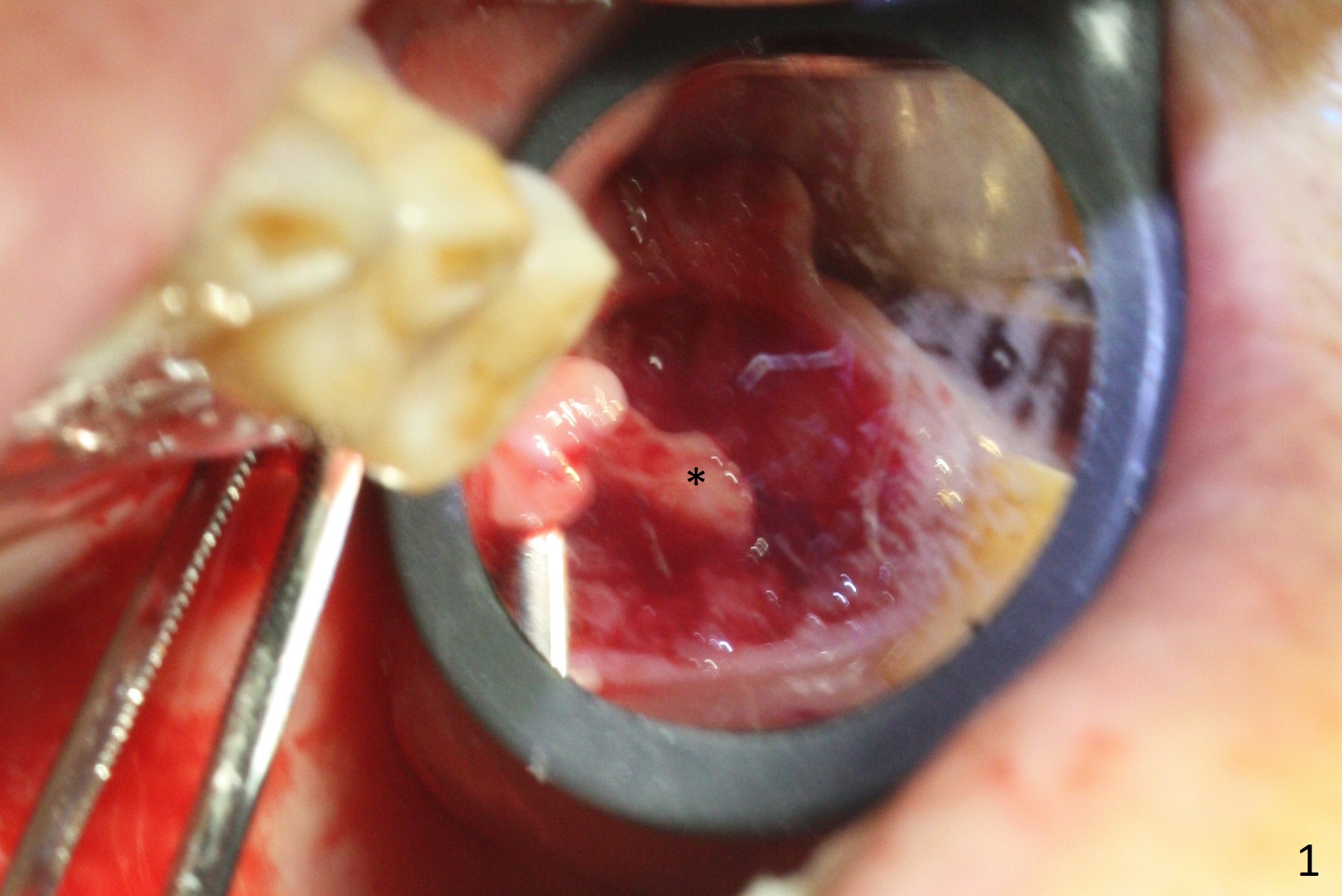
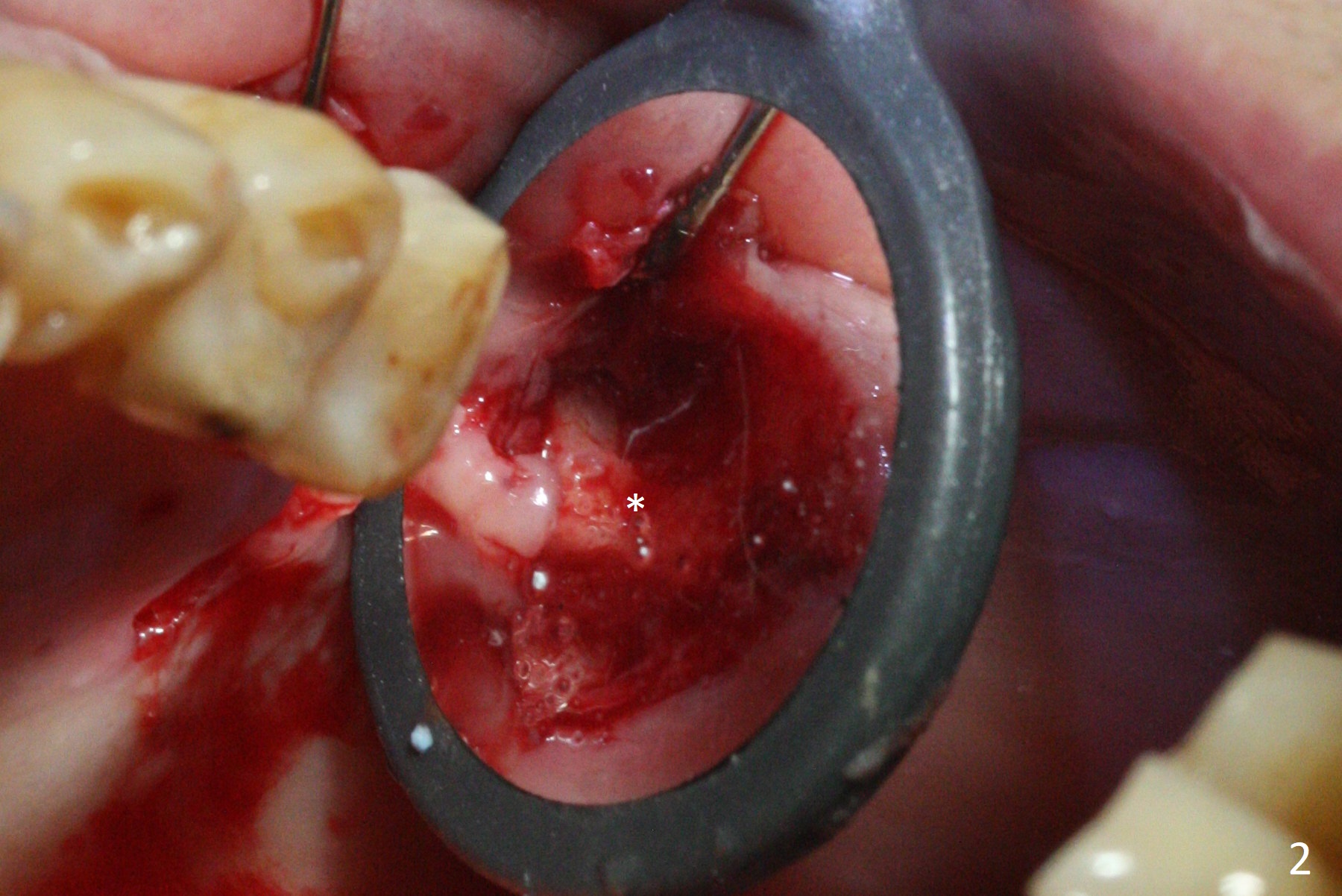
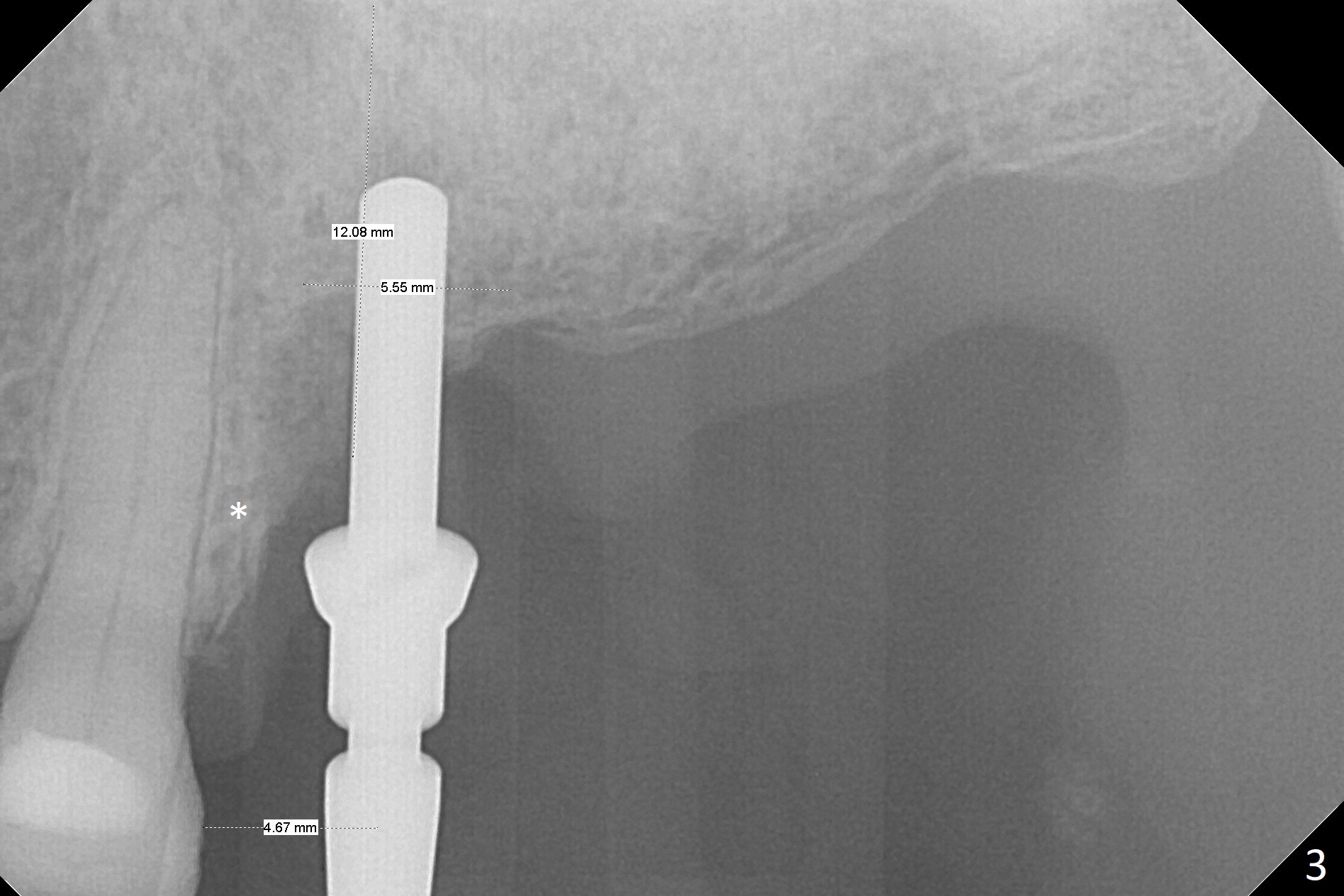
Stopper is Non-applicable when the Bone is Uneven
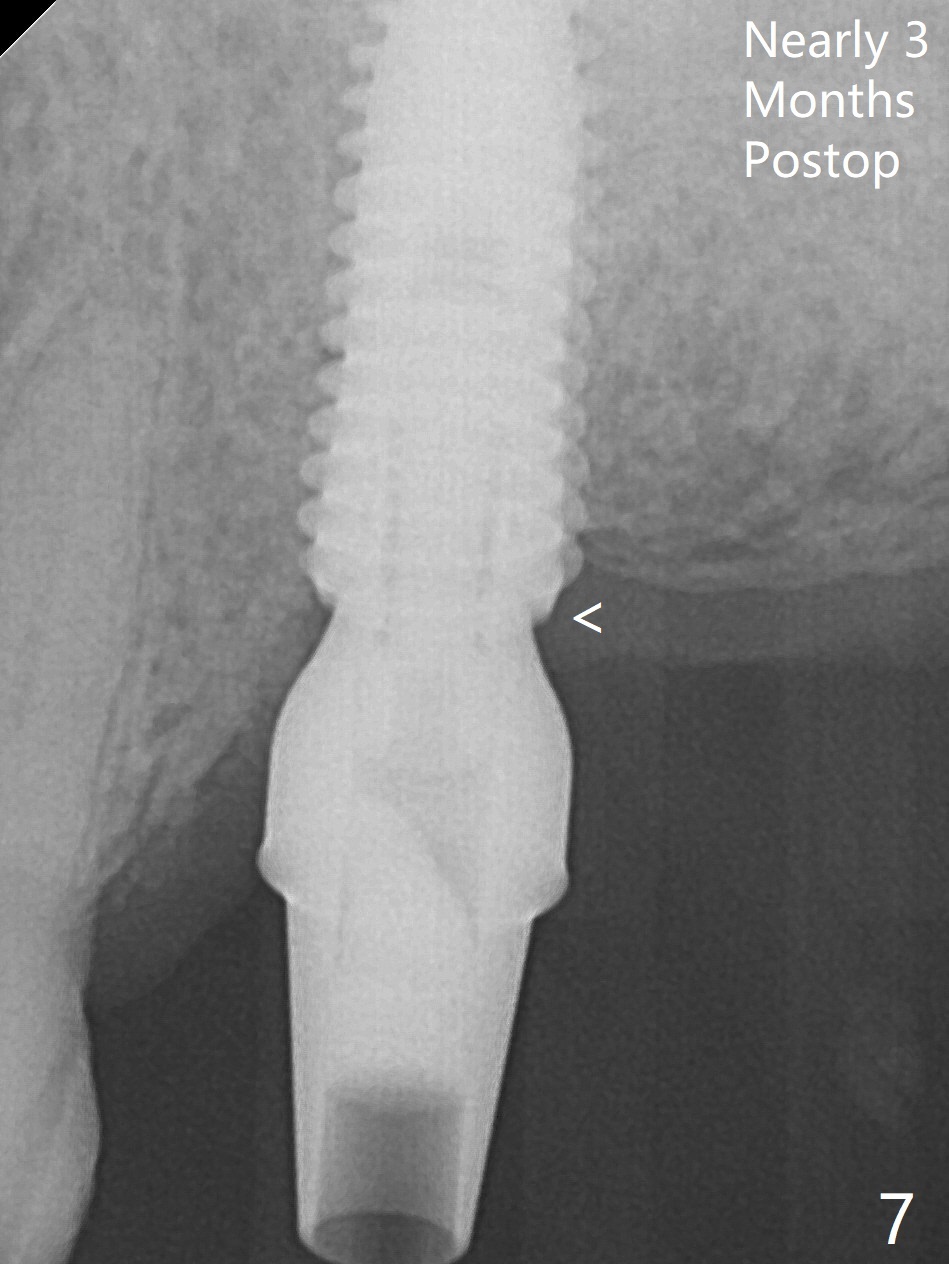
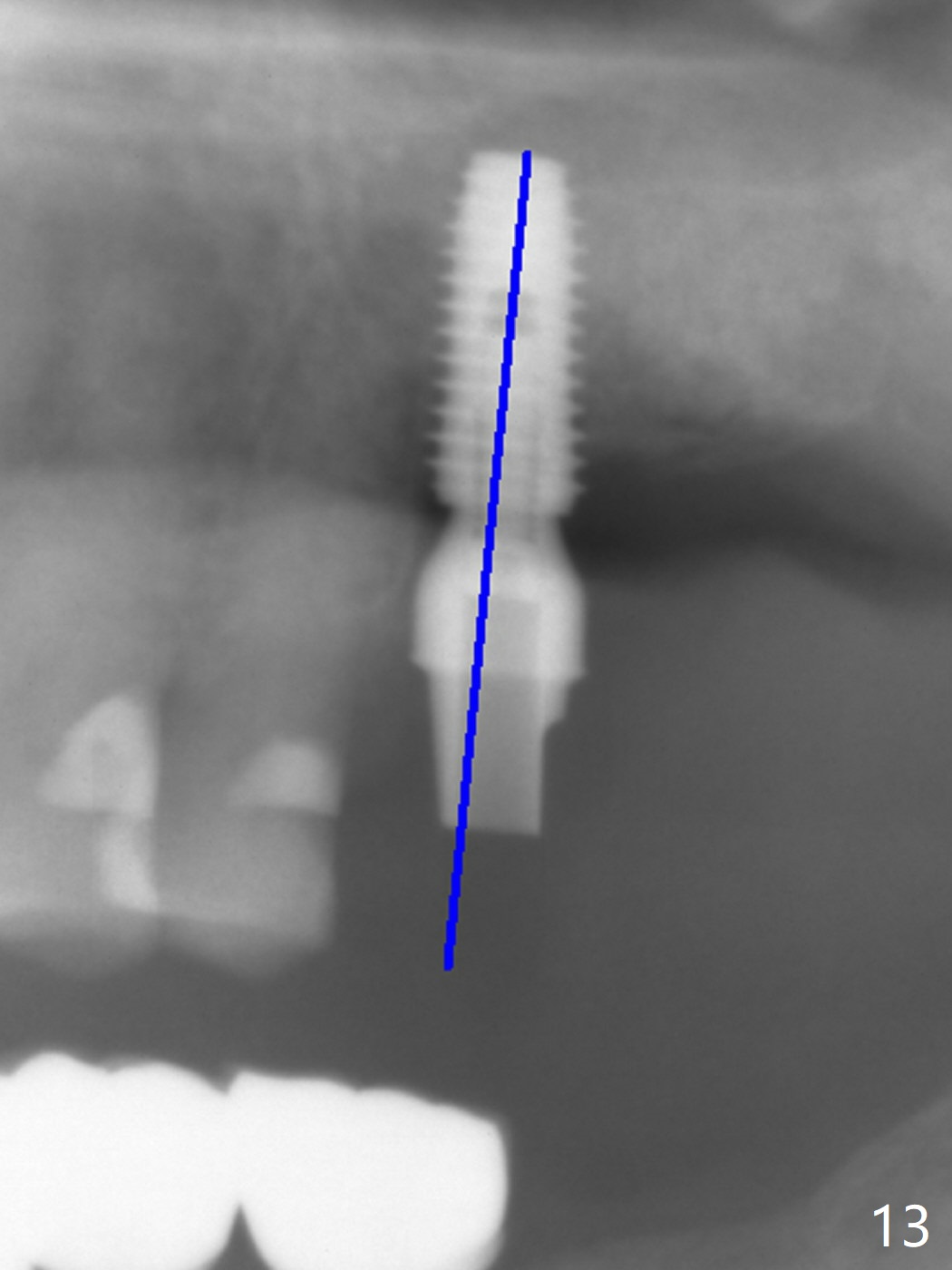
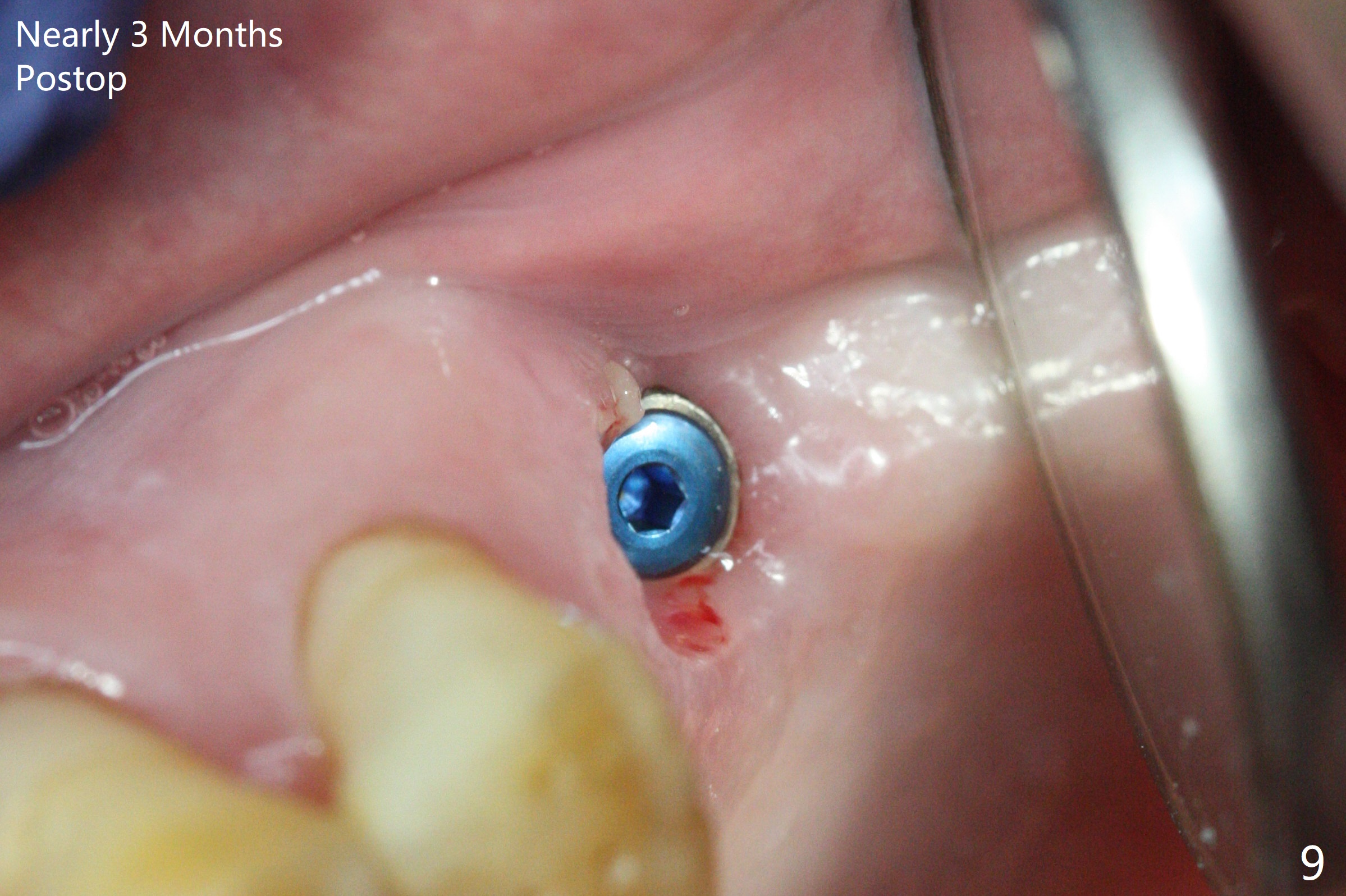
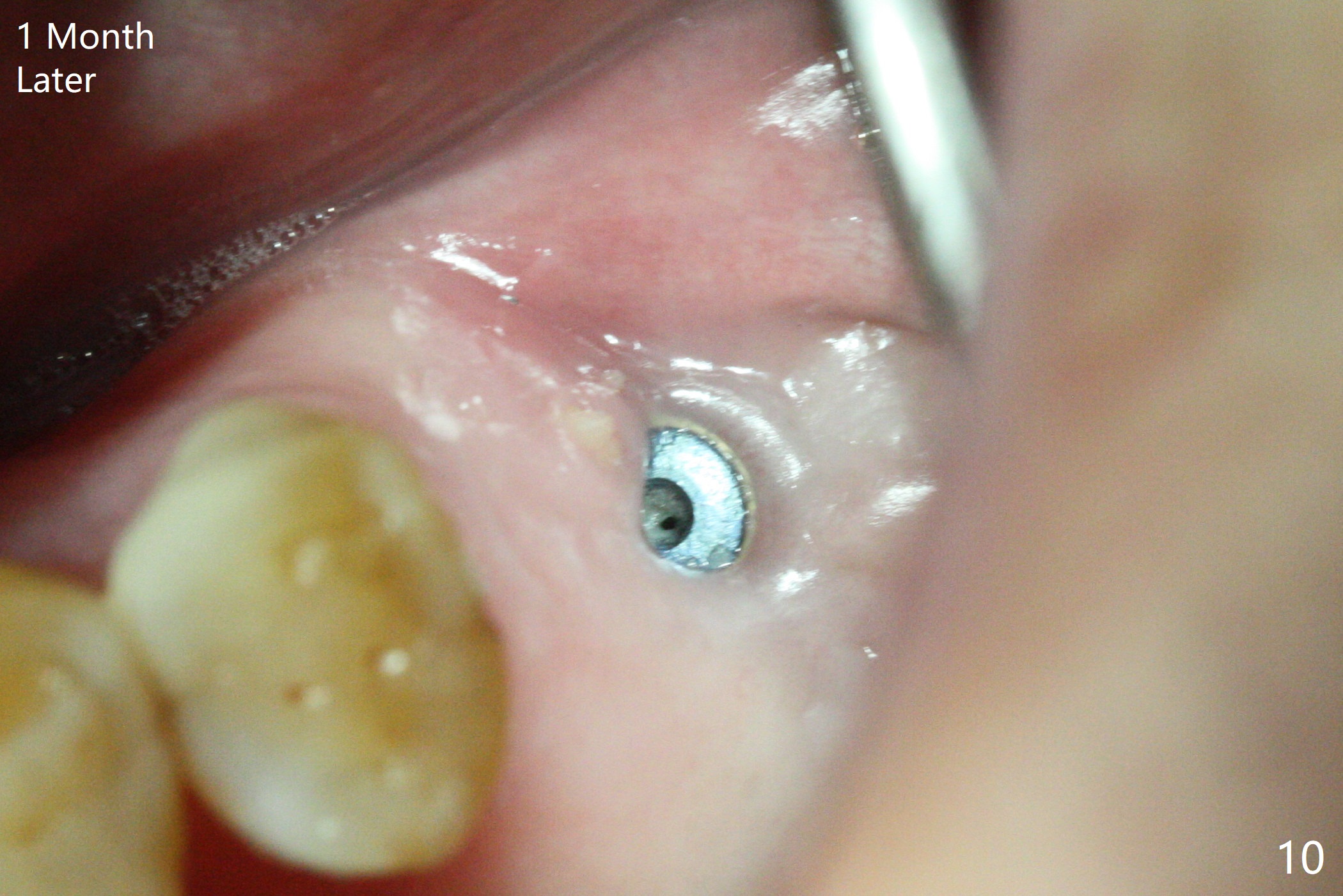
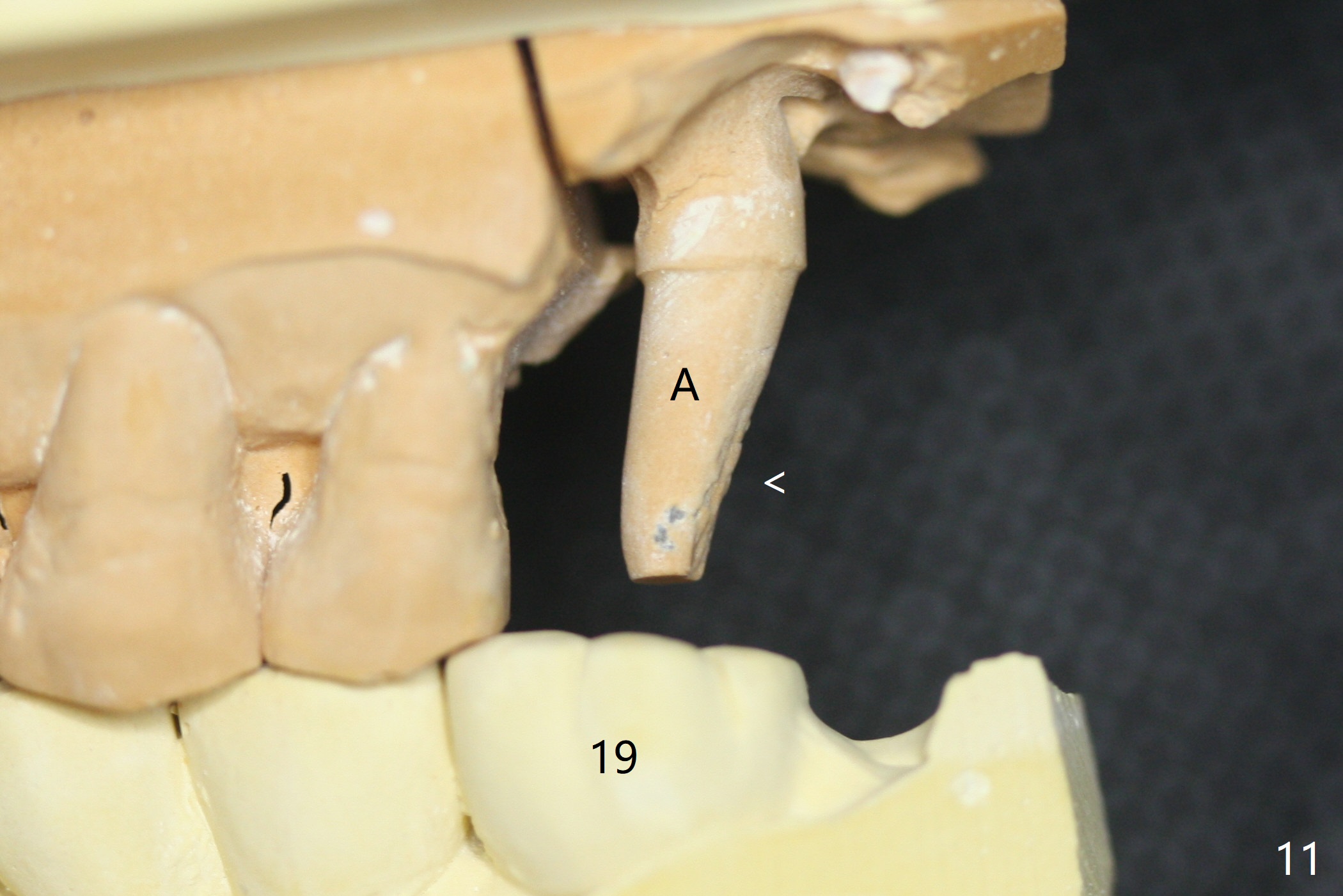
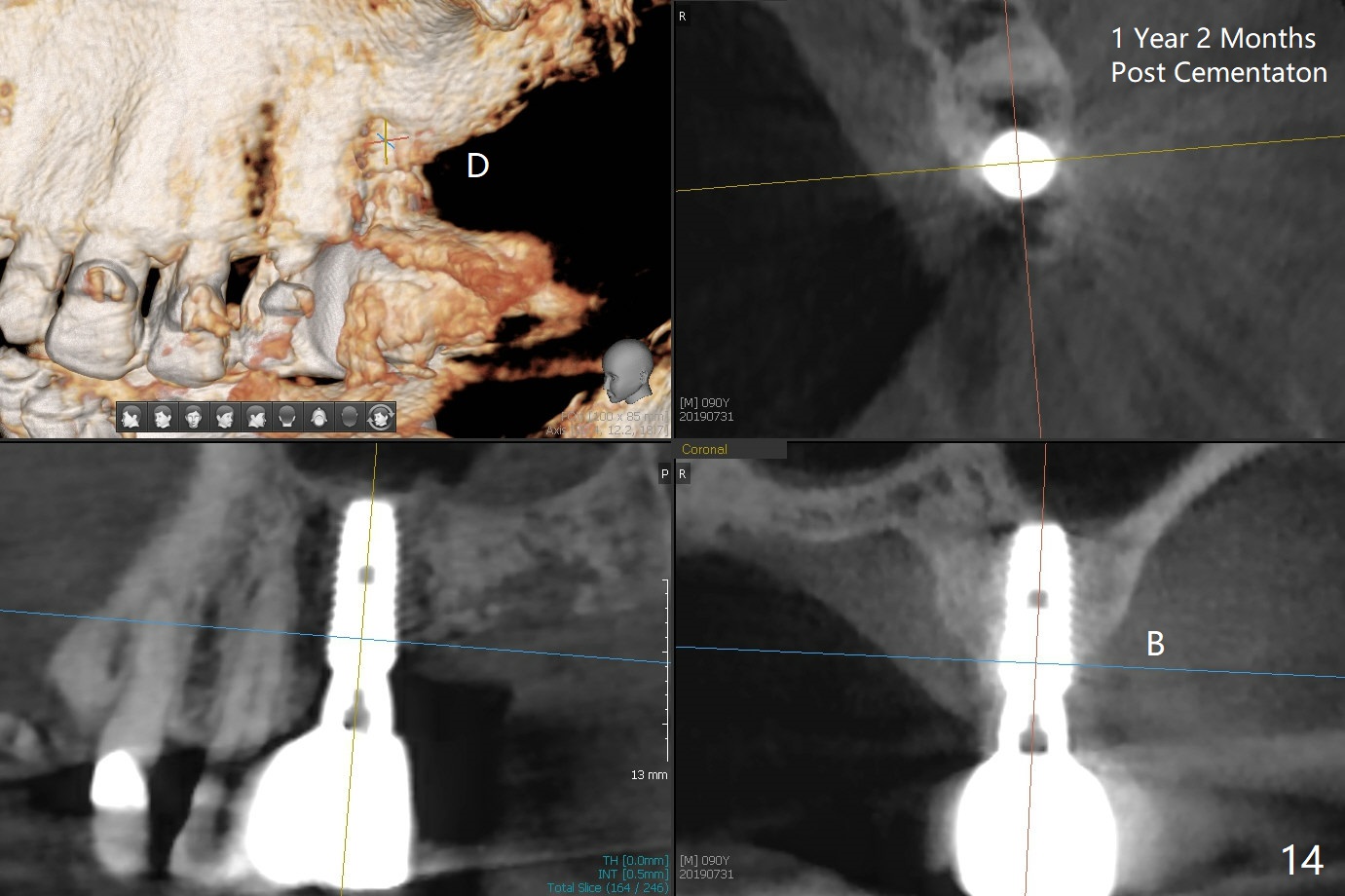
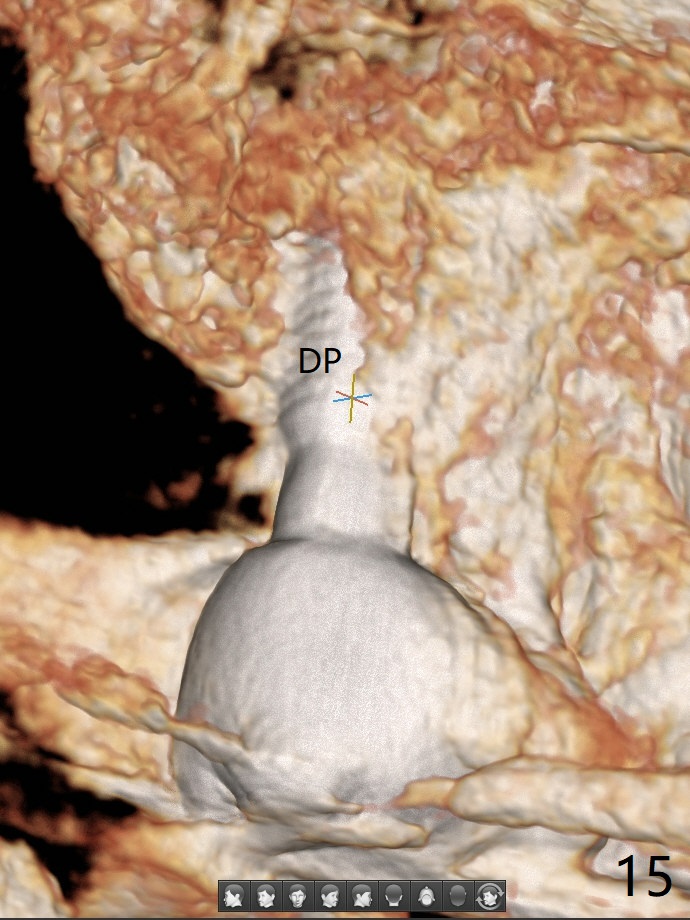
The septum is found to be pointed after extraction of the tooth #14 (Fig.1 *). The septum is flattened with Rongeur (Fig.2 *) prior to osteotomy. Because of interference of the mesial bone (Fig.3 *), osteotomy does not reach the depth with use of stopper. Without the latter, a 5x11.5 mm implant barely penetrates the sinus floor (Fig.4 (no postop nasal hemorrhage)). Also due to the mesial bone interference, a 6.5 mm abutment is not seated. Finally a 5.5x7(5) mm abutment is placed for an immediate provisional. Periodontal dressing is applied to cover the buccal repaired gingiva (Fig.5 *). There is minimal thread exposure after removal of the provisional nearly 2 months postop (Fig.6). The provisional does not return for easy self cleansing. In fact this is not an easy task, because of the posterior position (Fig.8 (after Piezo scaling)). The distal implant remains exposed; the abutment is removed and a healing screw is placed (Fig.9). The implant should have been subcrestal distally (Fig.7 <, nearly 3 months postop). One month later, the implant seems to be buried (Fig.10). The straight abutment is changed to an angled one (4.5 x15 degree A (5) mm) before impression retake (Fig.11,12 (<, dashed line: access hole)). The implant should have been placed more mesial (Fig.13). Surgical guide is needed. There is no implant exposure clinically or in CBCT sections 1 year 2 months post cementaton (Fig.14), although 3 D image suggests missing distopalatal plate (Fig.15).
Return to Upper Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments Xin Wei, DDS, PhD, MS 1st edition 11/30/2017, last revision 07/31/2019