Guided Surgery Done with Confidence
With understanding tissue punch and engagement of drill as much as possible
into guide sleeve before pressing pedal, guided surgery is accomplished with
confidence (Fig.1,2). With
undersized drilling, there
is no thread exposure palatally, when a flap is raised. Vanilla graft is
placed, since it has been prepared before incision. No membrane is used.
It appears that the palatal bone expands while the implant is being placed.
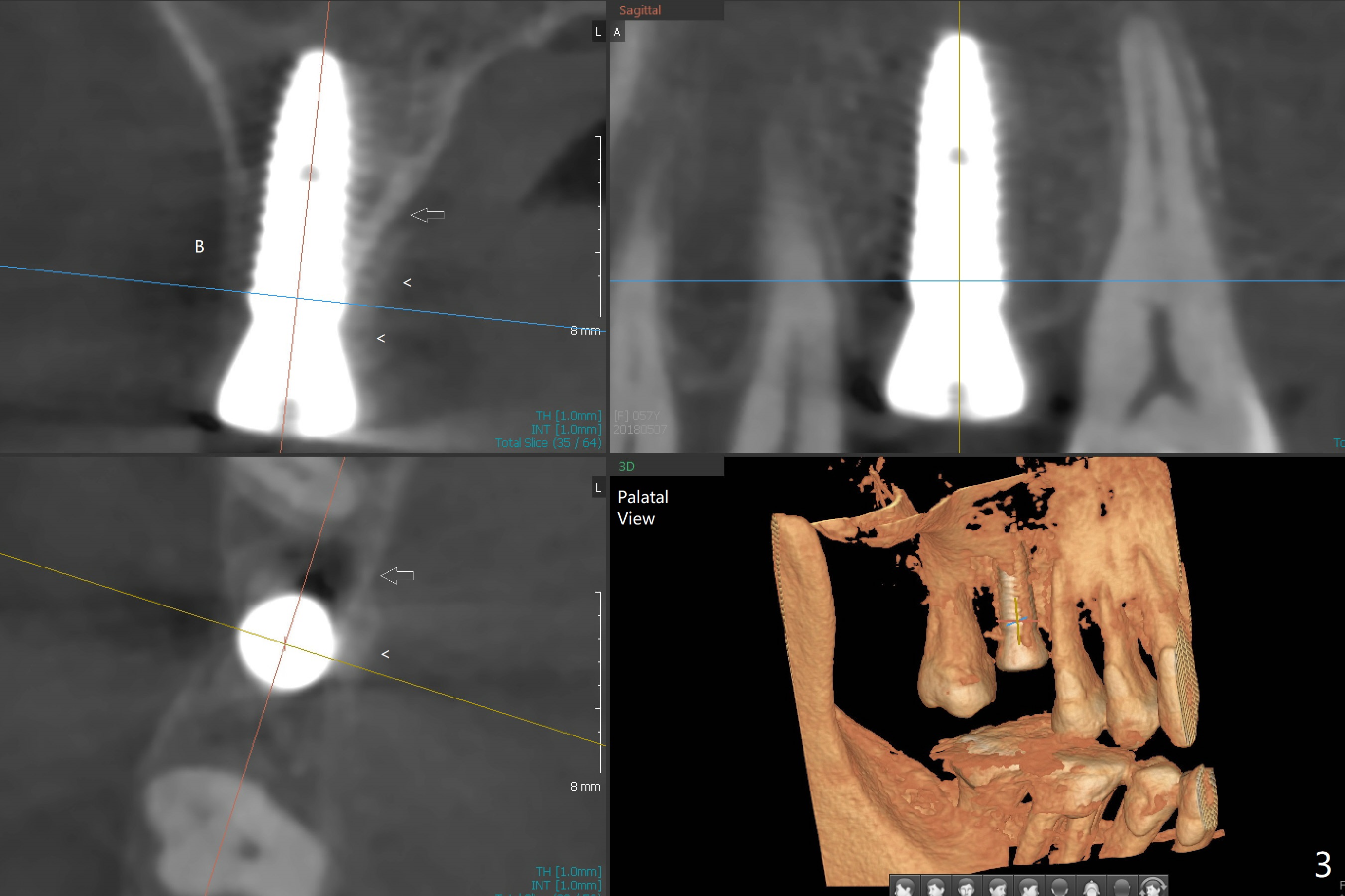
CBCT taken 10 days postop shows apparently the coronal end of the palatal plate
(Fig.3 arrows) and bone graft (<). Although postop pain is slightly more
associated with incision for bone graft, the wound heals with periodontal
dressing 10 days postop.
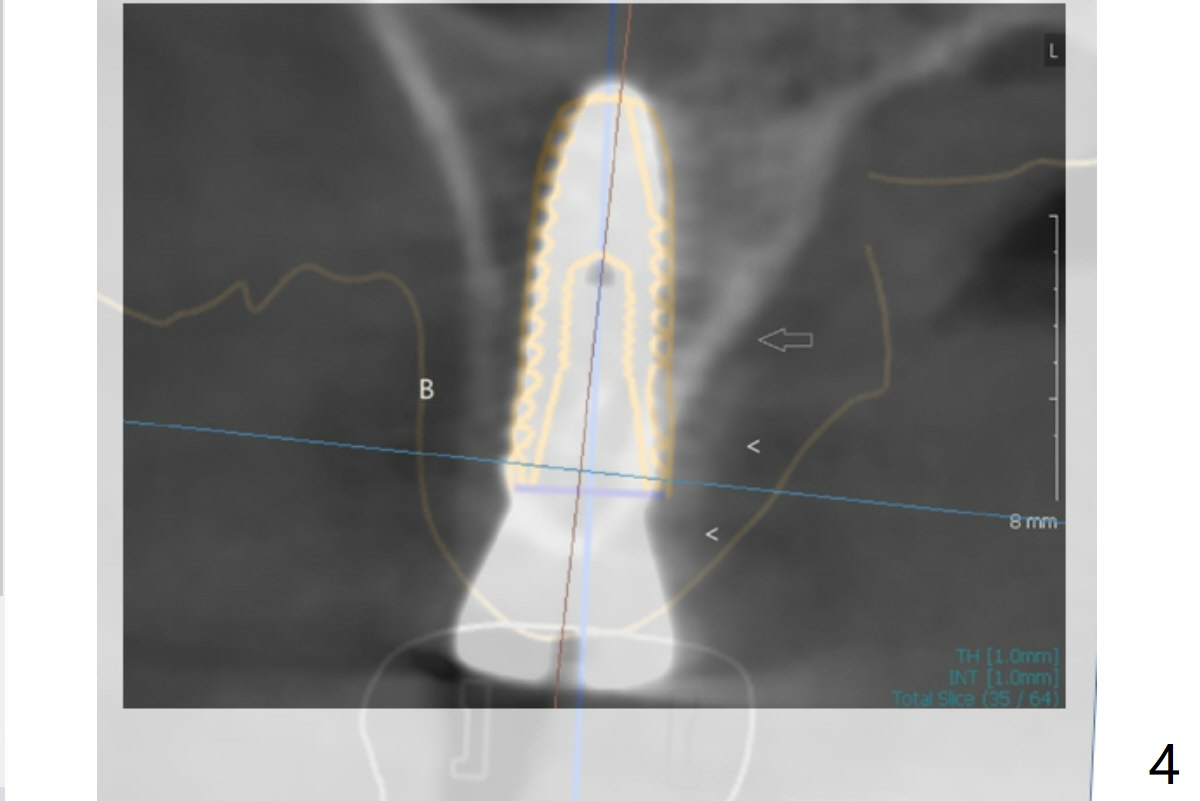
Again thank you for sharing your valuable experience and it is quite
interesting that bone expands when we did the undersized drilling. I just
double checked the planning and found out that the original design had
palatal thread exposure but when I see the screenshot, it is not. That is
quite interesting and we have not heard about that quite yet. I mean the
fact that undersized drilling has saved bone graft. Let's try in other
applicable cases again and it is verified as working, this could be a great
idea to minimize the possibility of unnecessary bone grafting. Jennifer
overlaps the images of the design and the postop CT (Fig.4).
There is mild crestal bone loss 4.5 months postop (Fig.5).
When the patient returns for periodic exam and prophy 6 months post
cementation, the crown is found to be loose, which is more likely
associated with heavy mastication (long roots) and poor crown/implant
ratio. Since the distal contact is light, the case returns to lab.
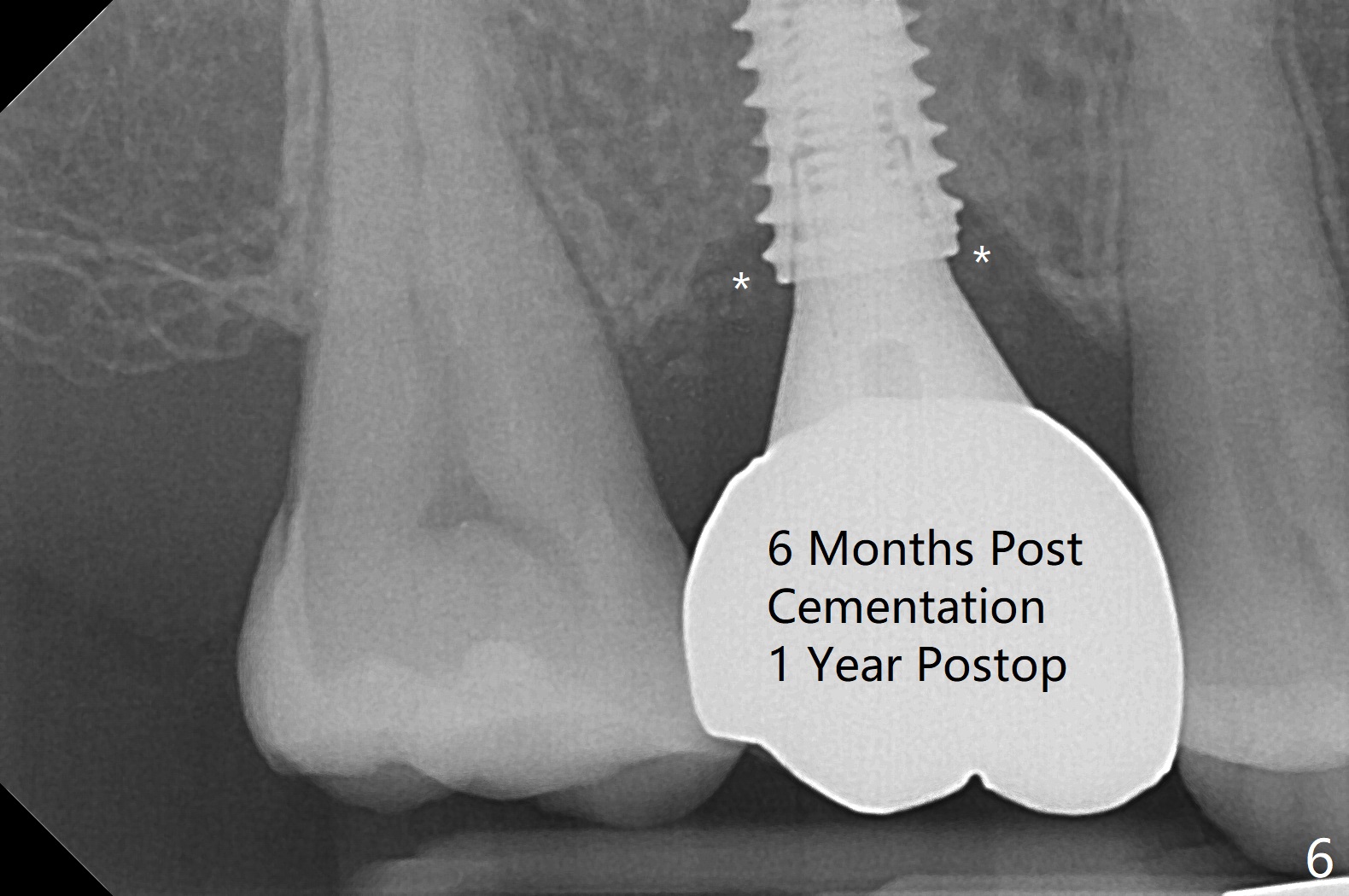
PA taken following reseating the repaired abutment/crown shows crestal bone
loss, which may be associated with the narrow ridge and/or the loose
abutment. The gingival cuff is less healthy
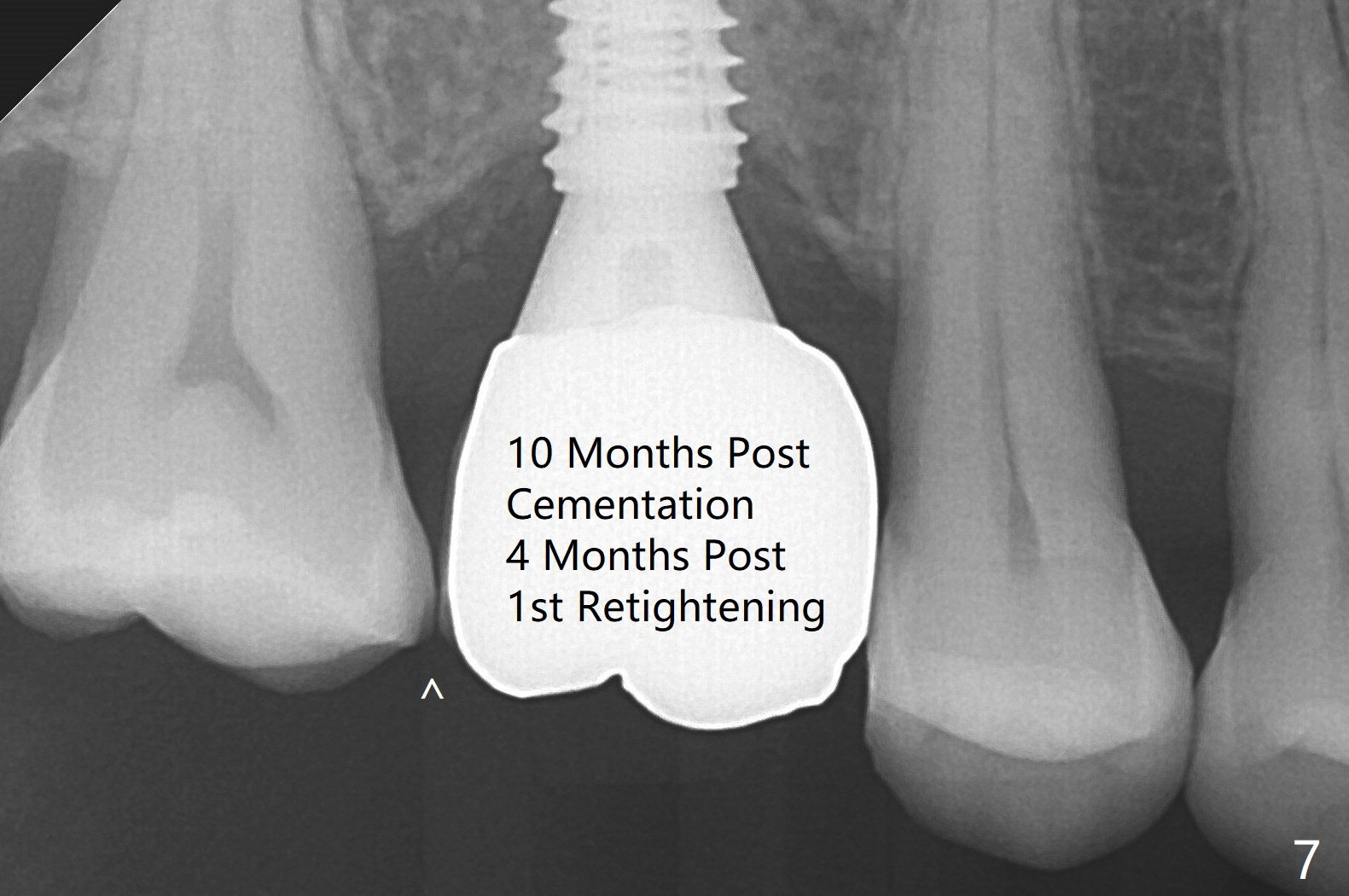
(Fig.6). The screw becomes loose again 4 months later.
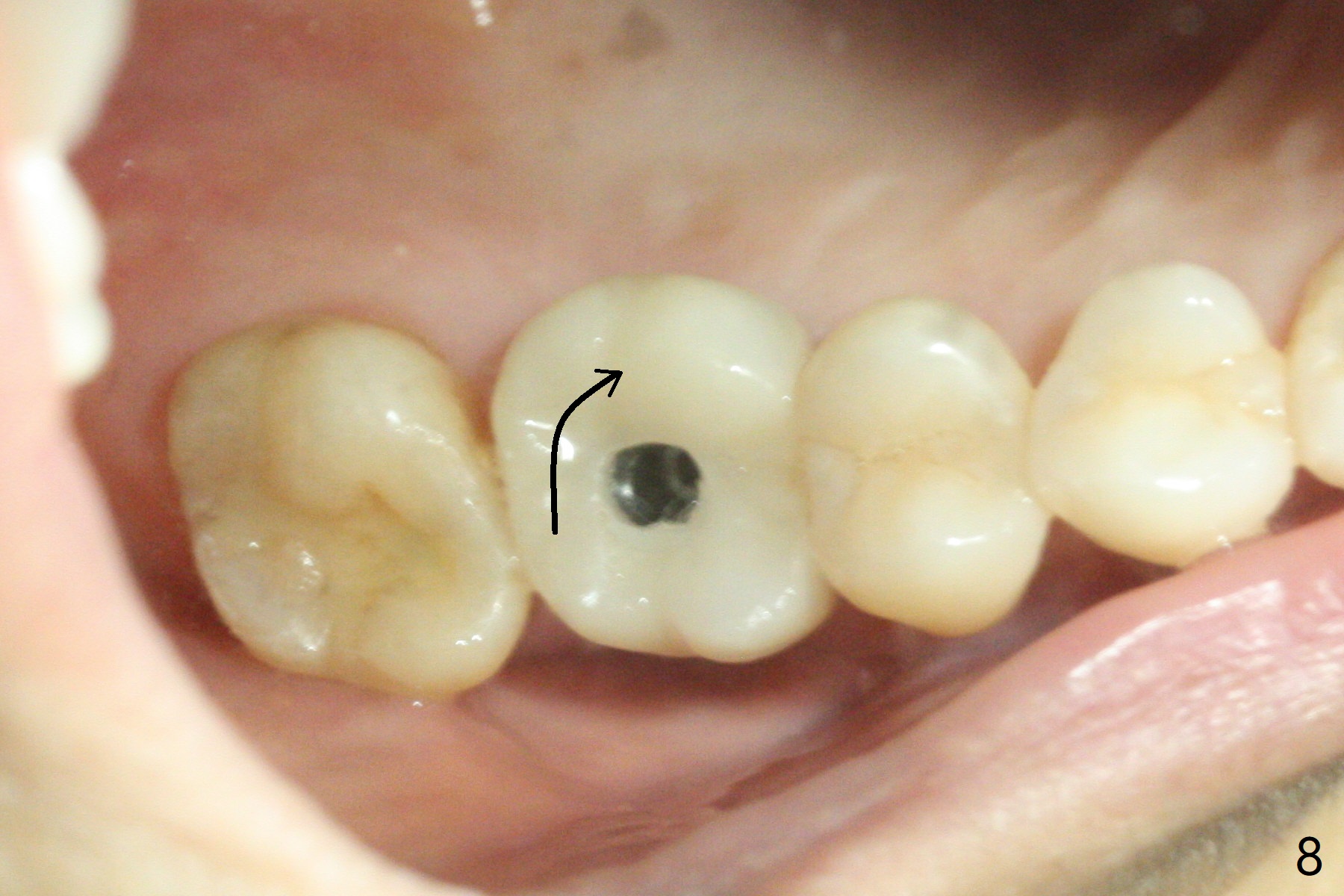
When it is retightened, the distal proximal contact turns open (Fig.7 ^).
The crown appears to turn with the underlying abutment (Fig.8). After
breaking proximal contacts, the crown/abutment is retightened and pick up
impression is taken. It is likely that the abutment was not seated
right when abutment-level impression was taken. The crown table is
slightly oversized (Fig.8). Three months later, the screw becomes loose for
the 3rd time (unilateral mastication, pain at #19 without RCT). The abutment hex is not worn. The crown is removed
and the abutment is reseated and torqued 30 Ncm. Impression is taken
for new crown. The latter is cemented without removing the
abutment (Fig.9 (note bone loss)). In fact the crown/abutment should have been torqued with
screw driver buried in place!
Return to
Upper
Molar Immediate Implant,
Armaments
Xin Wei, DDS, PhD, MS 1st edition 04/27/2018, last revision
12/11/2019