,%2013%20old%20abutment,%20laser%20gingivectomy.jpg)
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
How to Avoid Touching Neighboring Root?
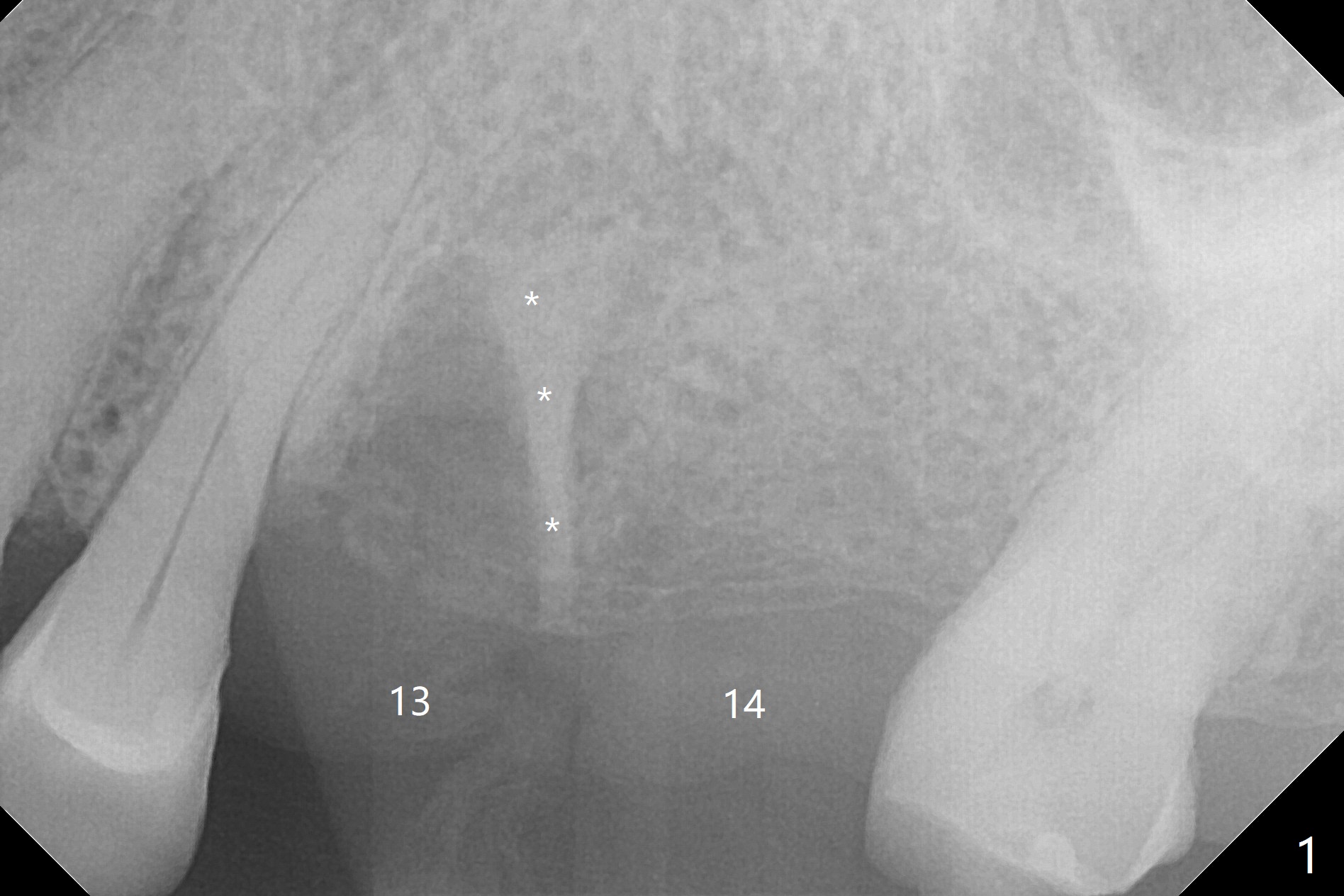
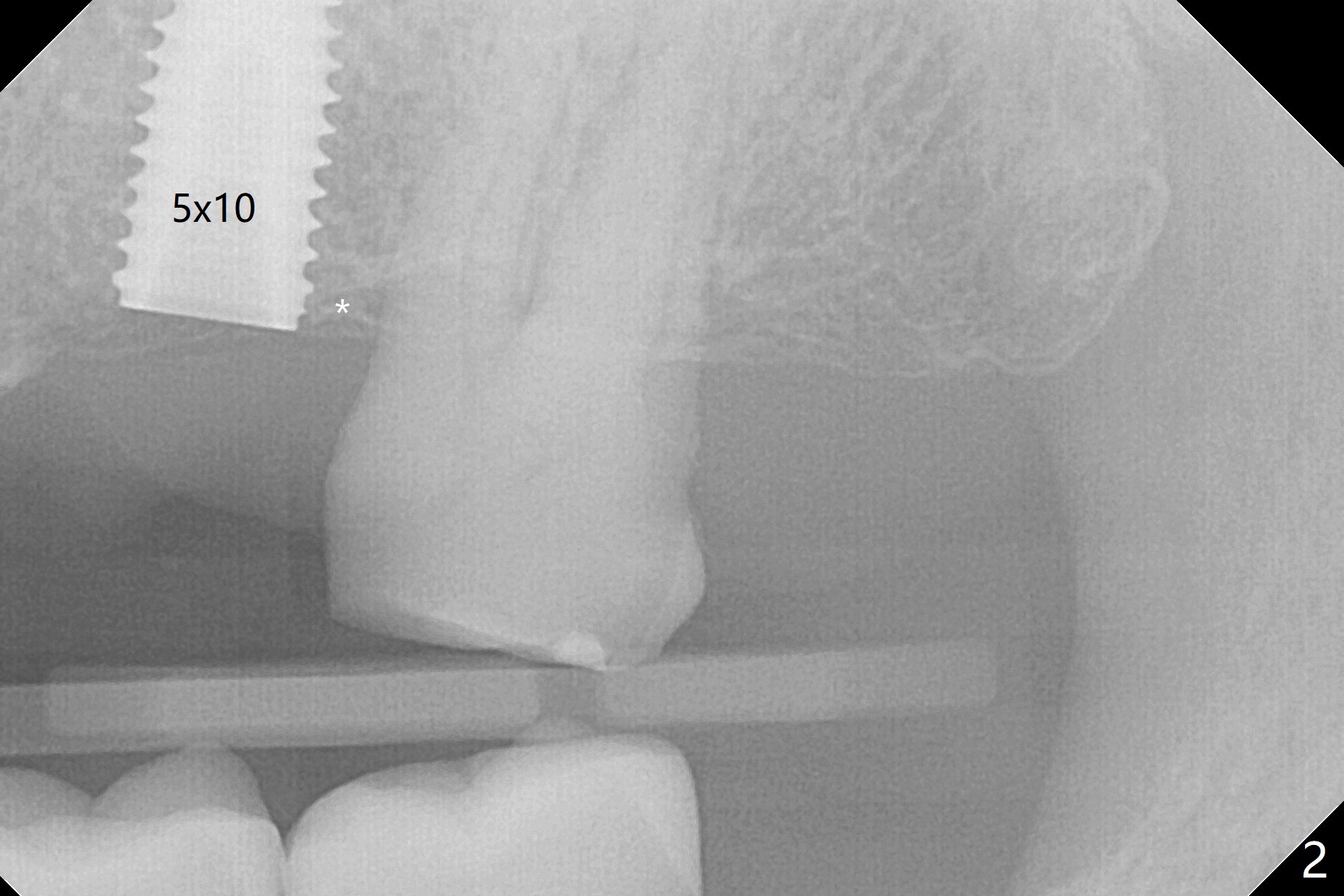
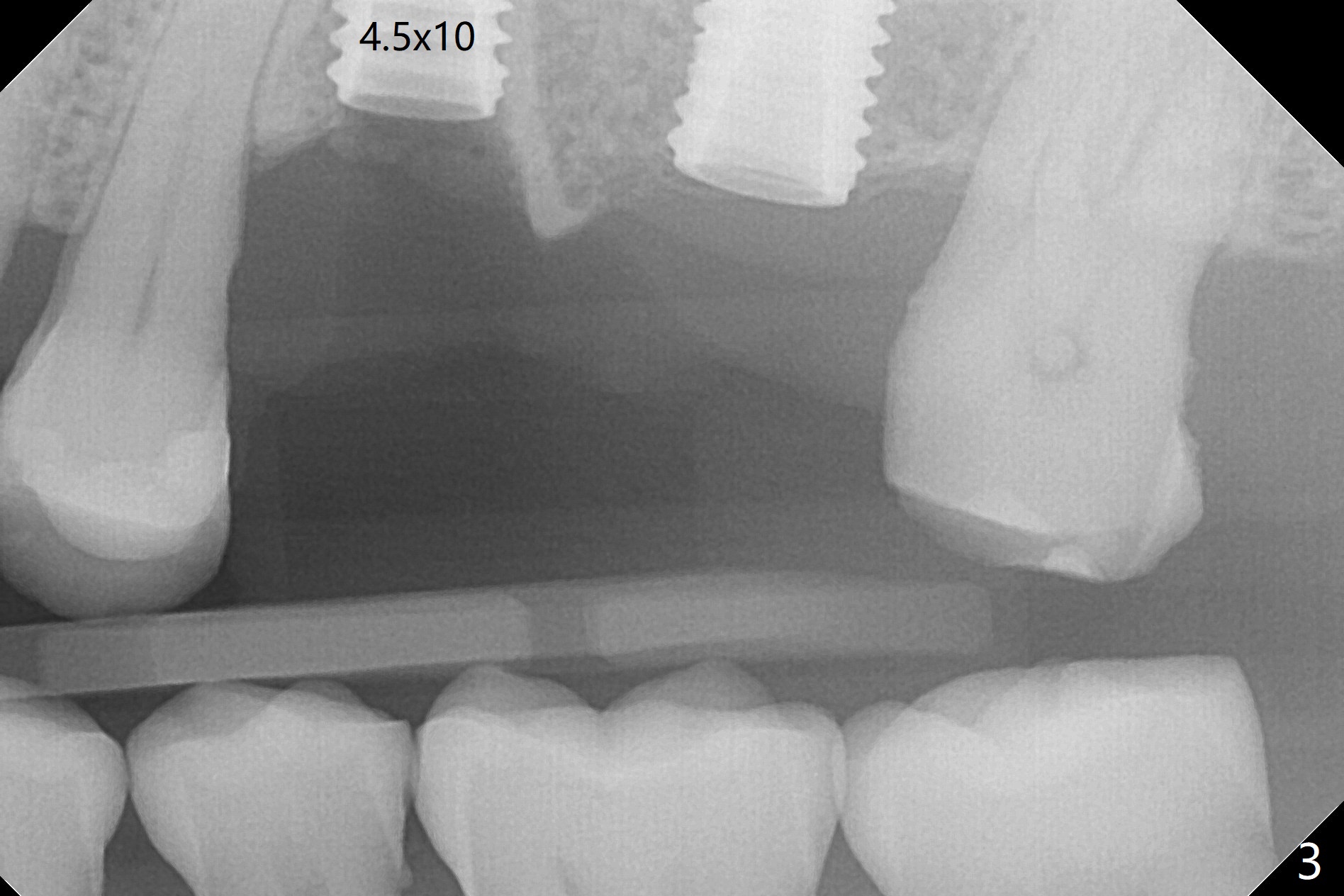
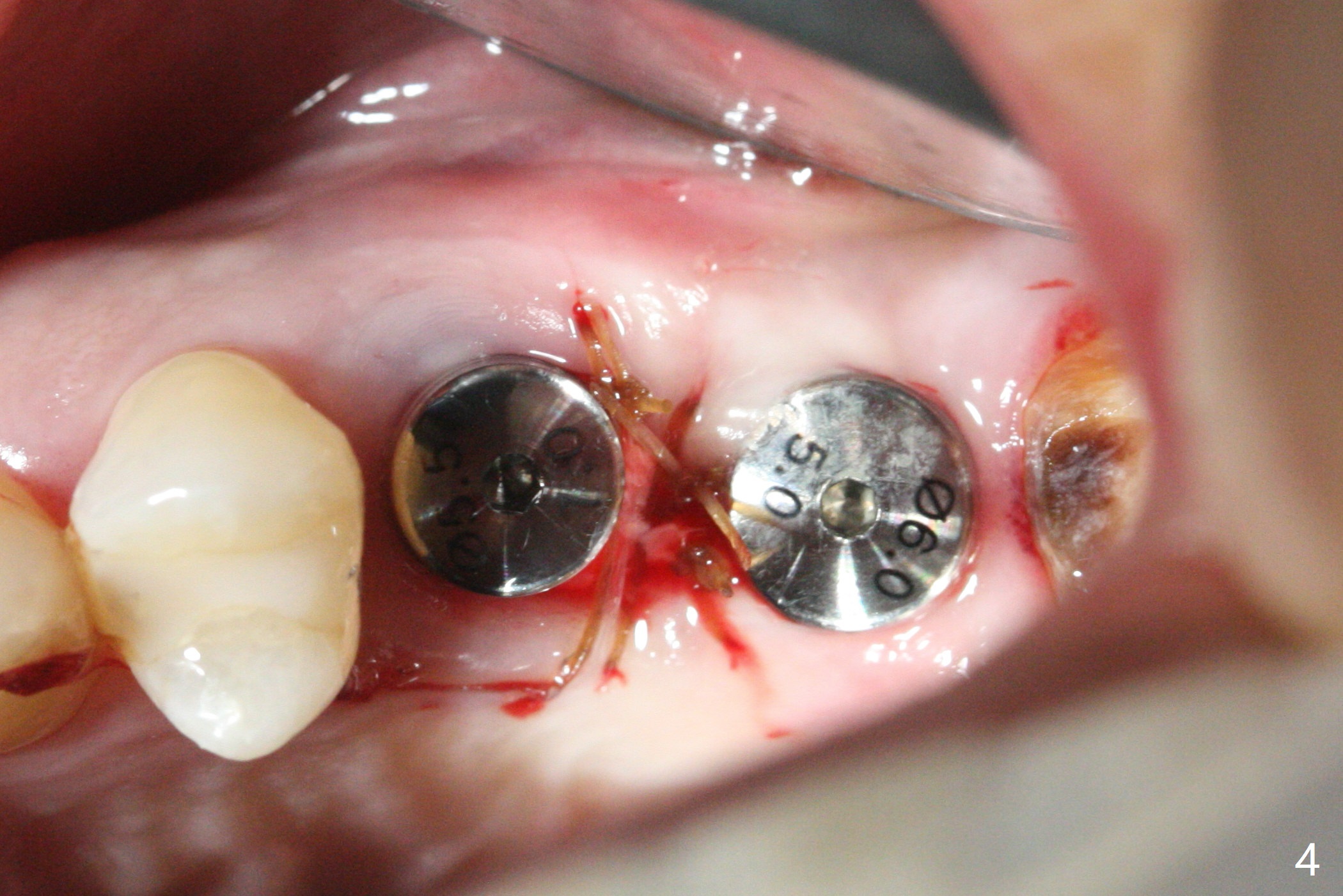
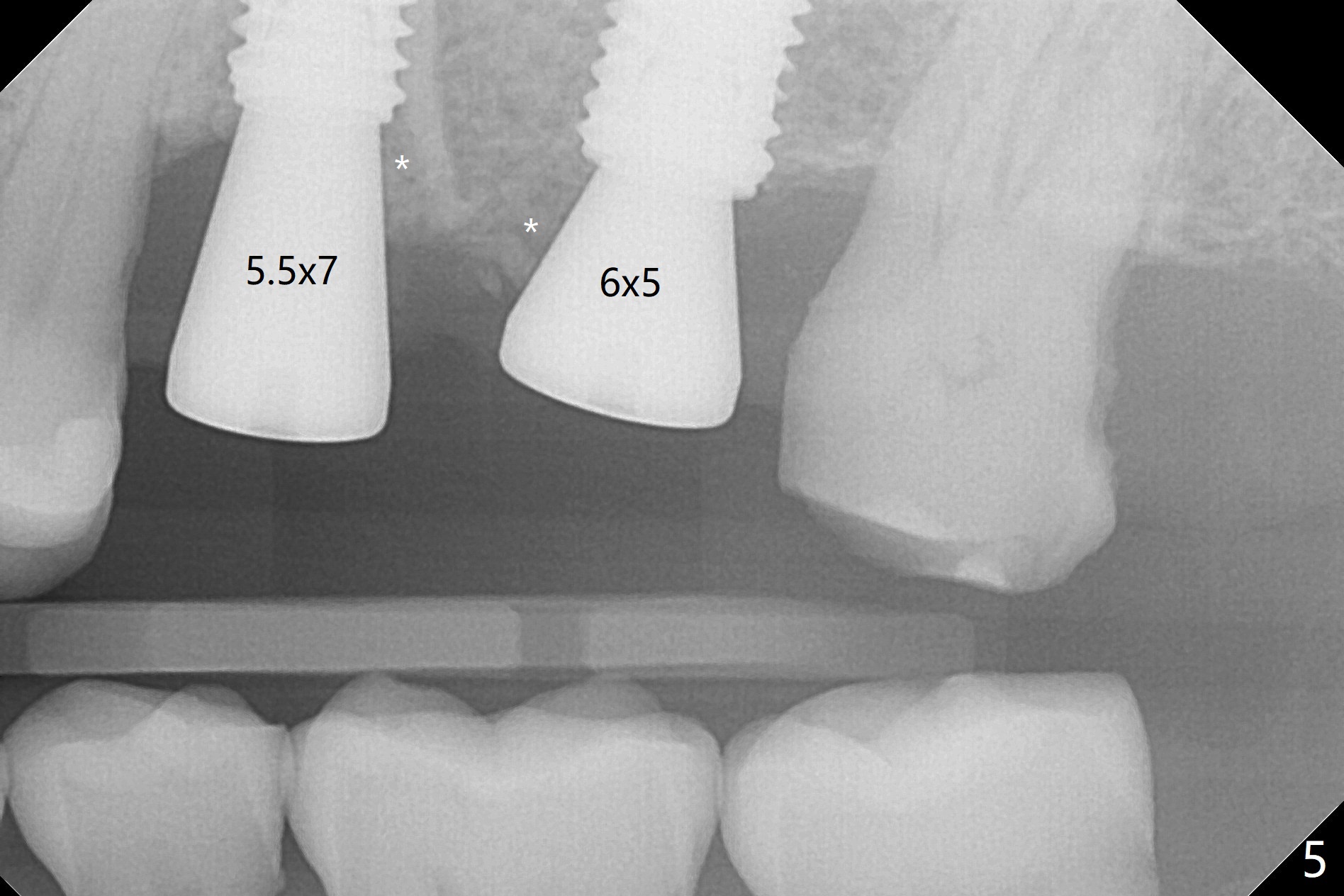
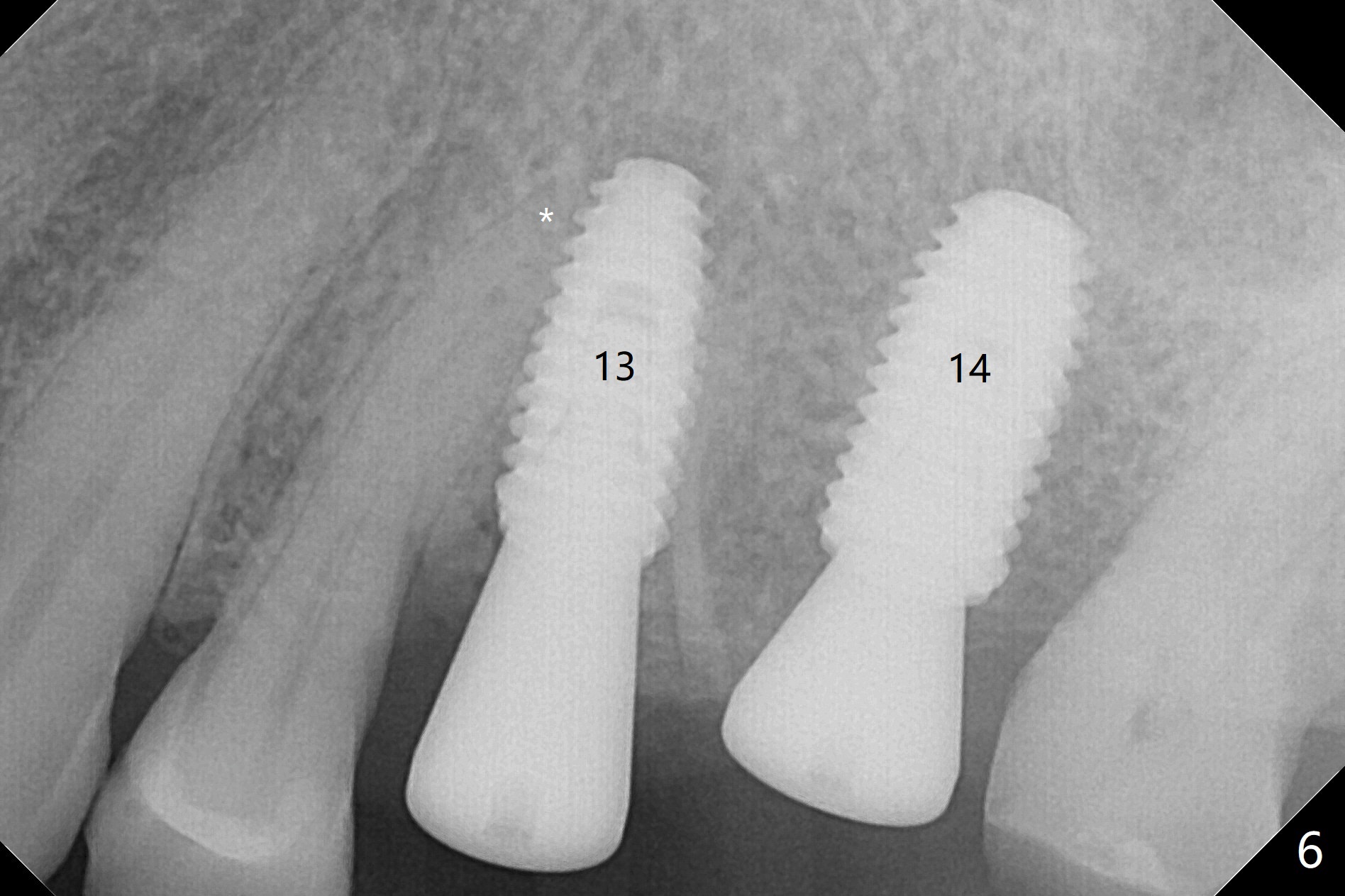
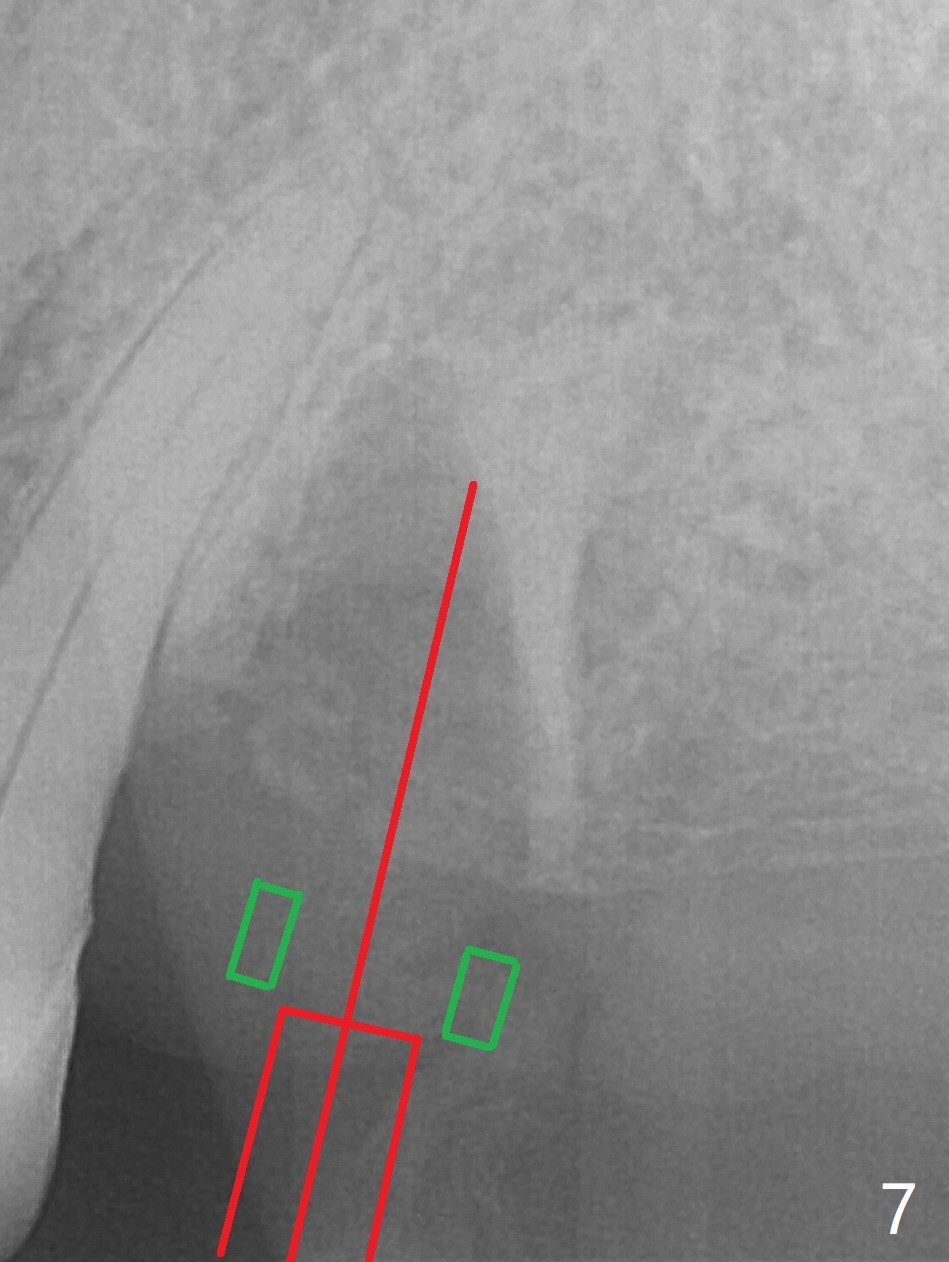
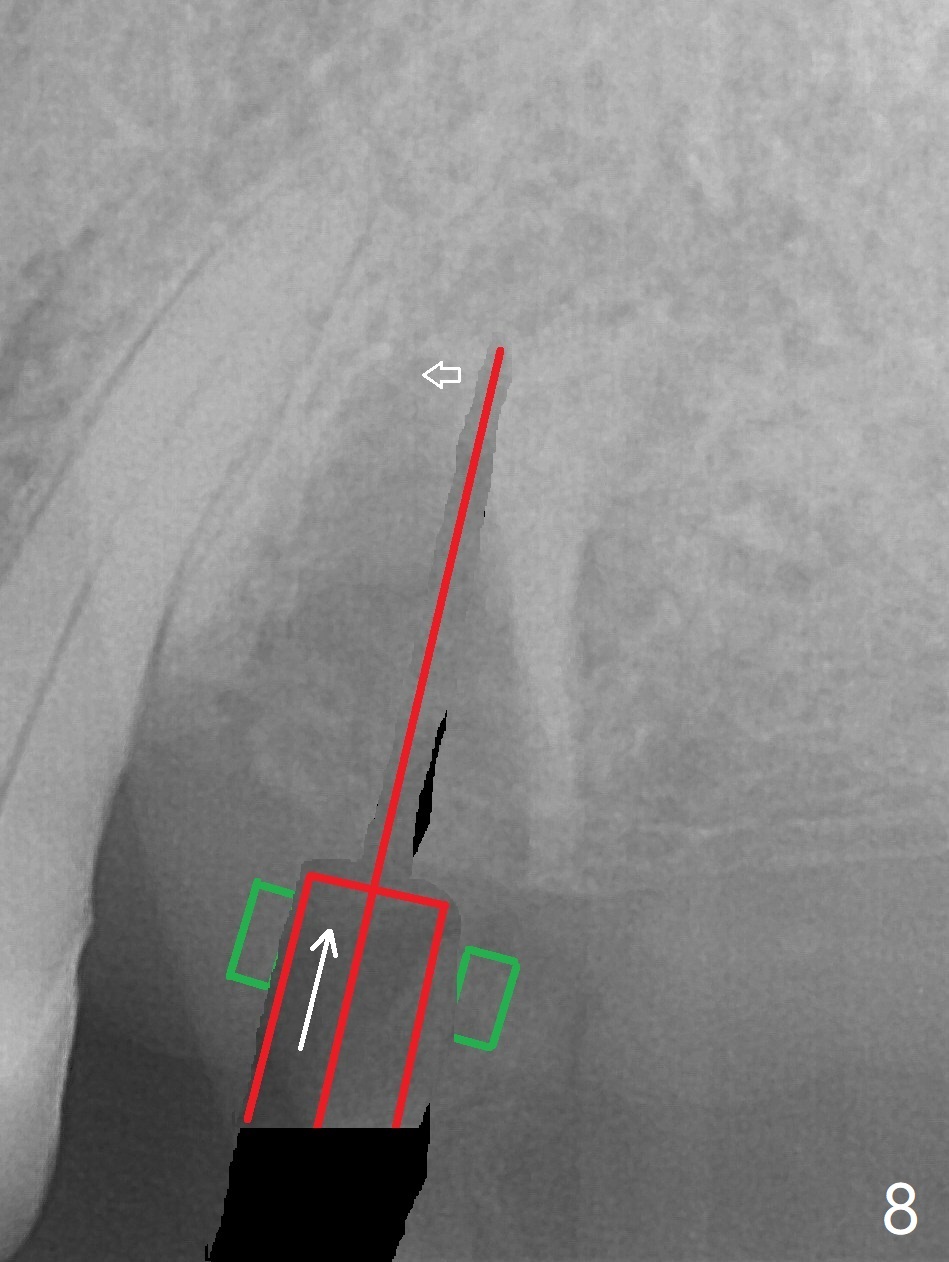
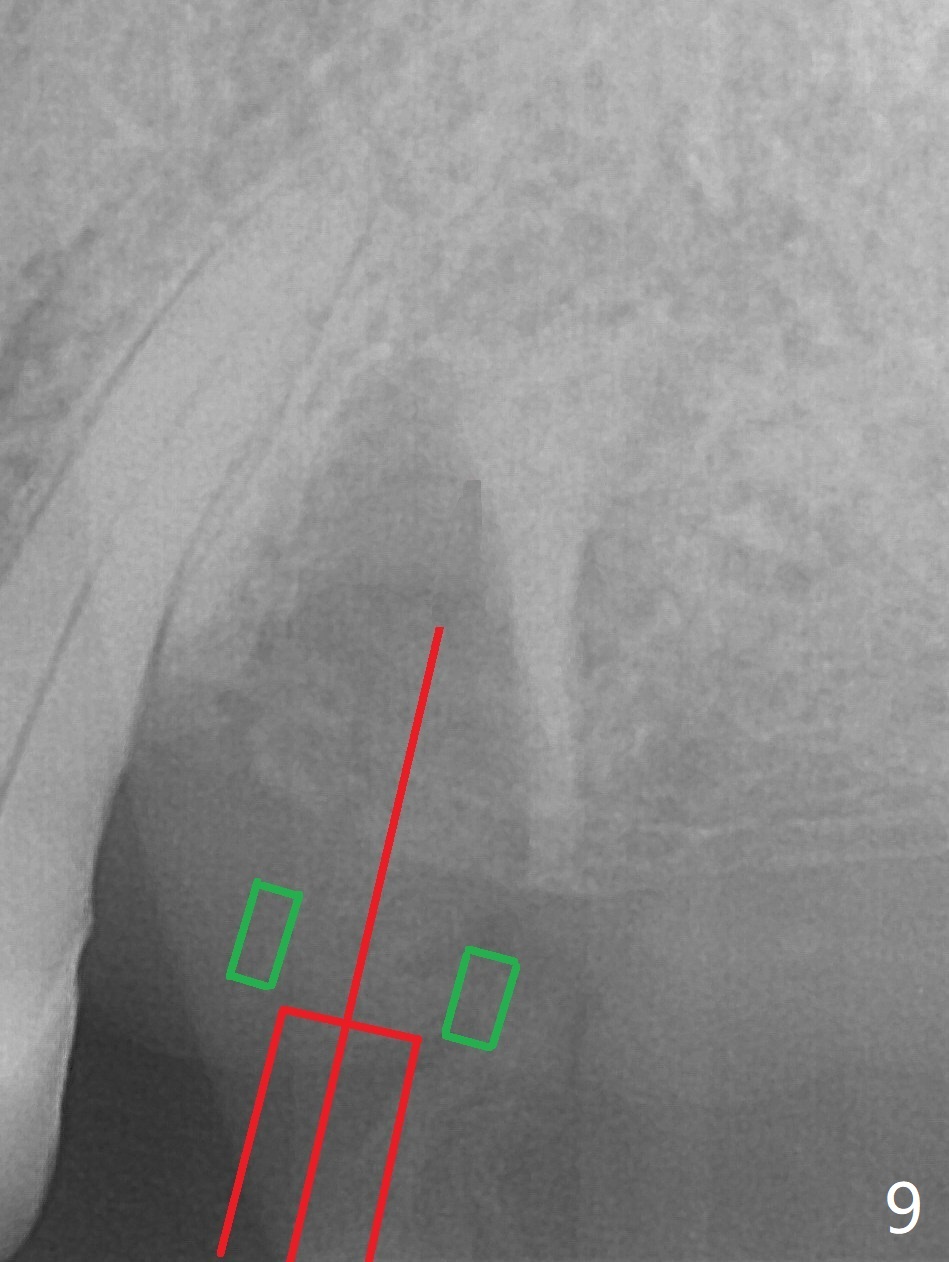
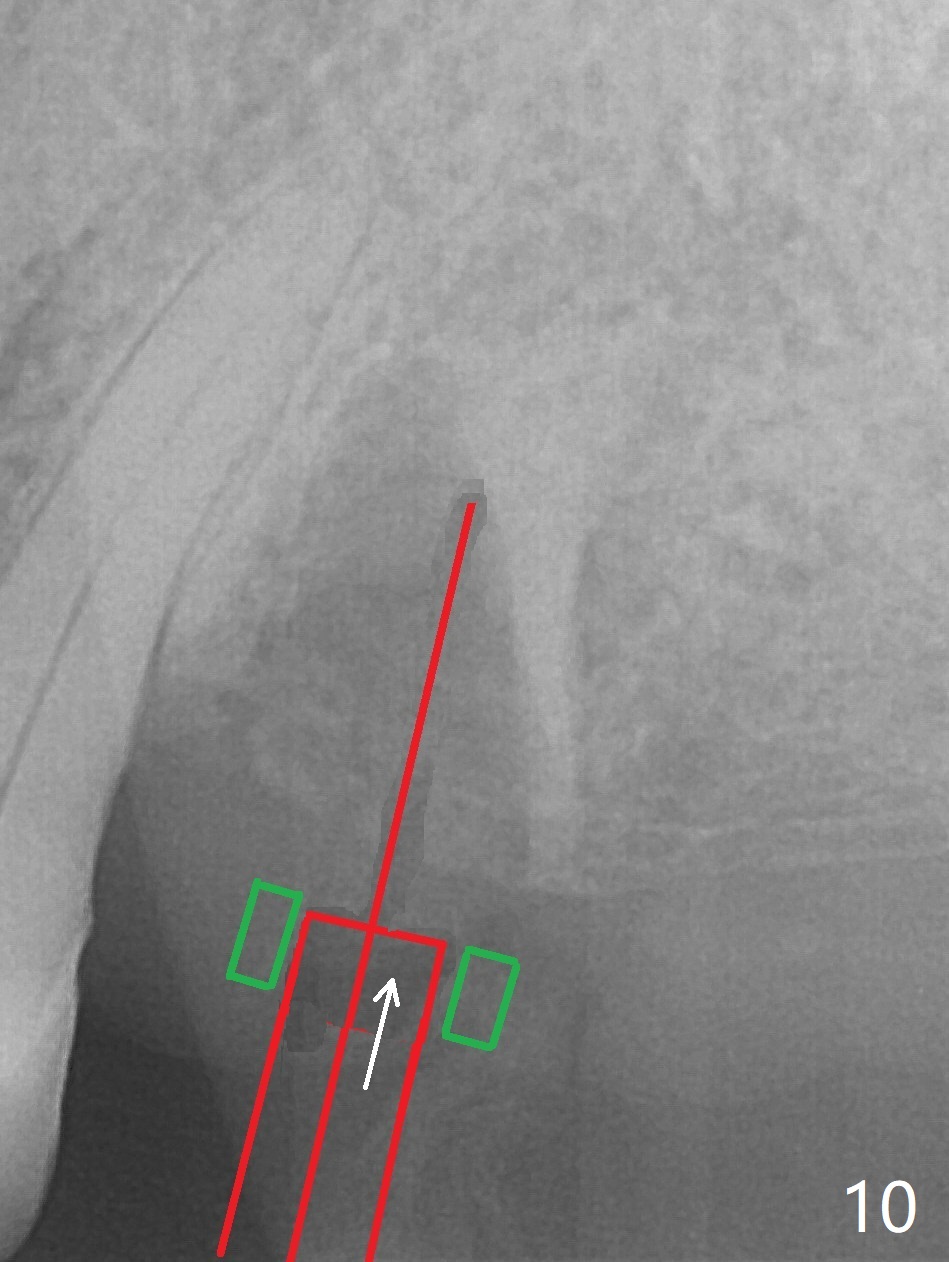
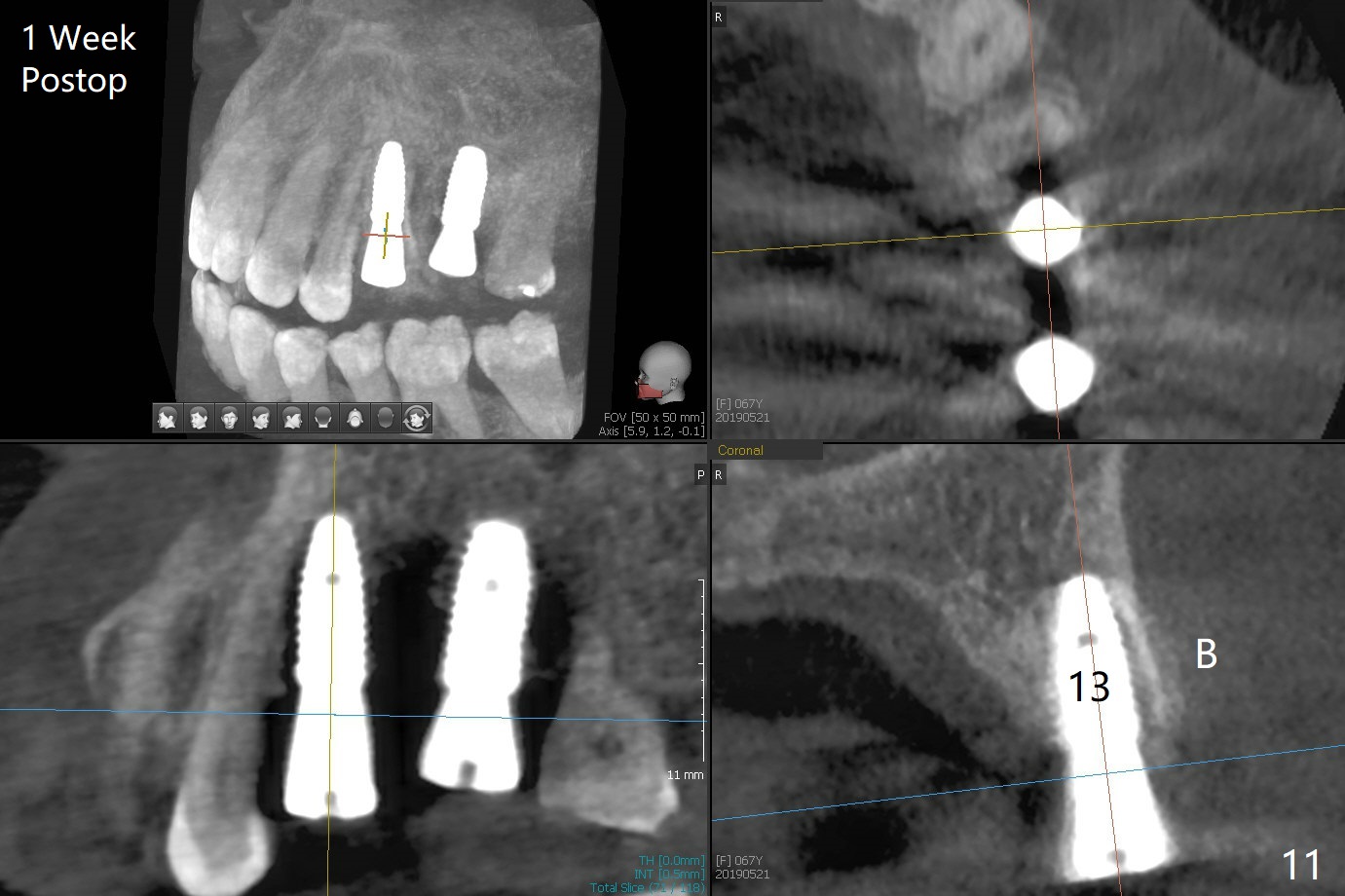
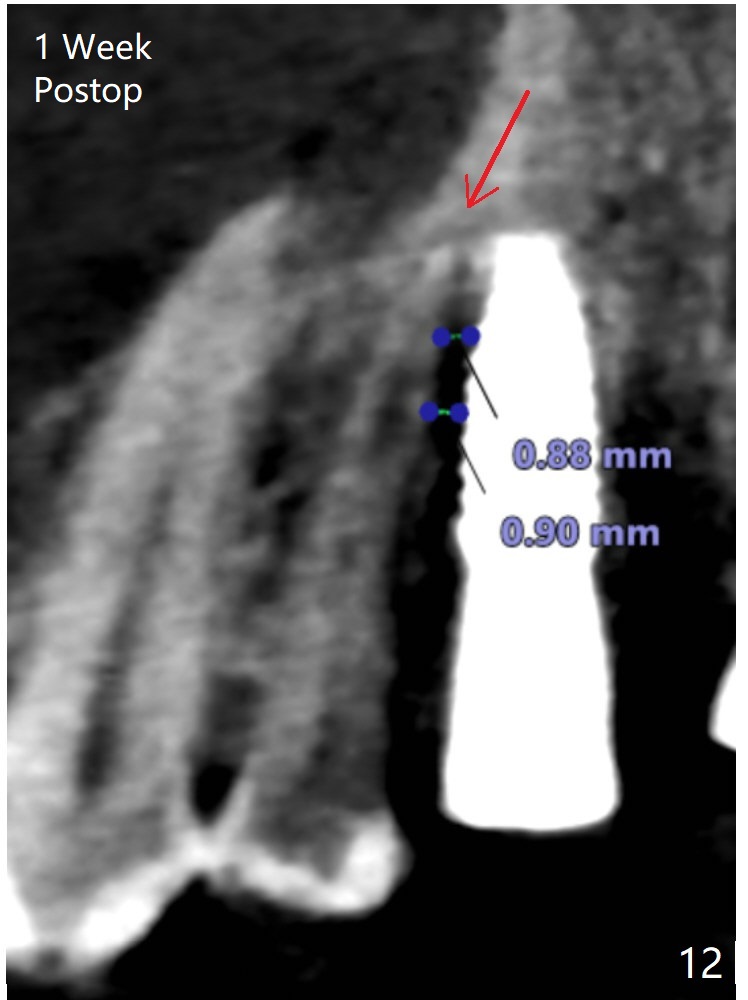
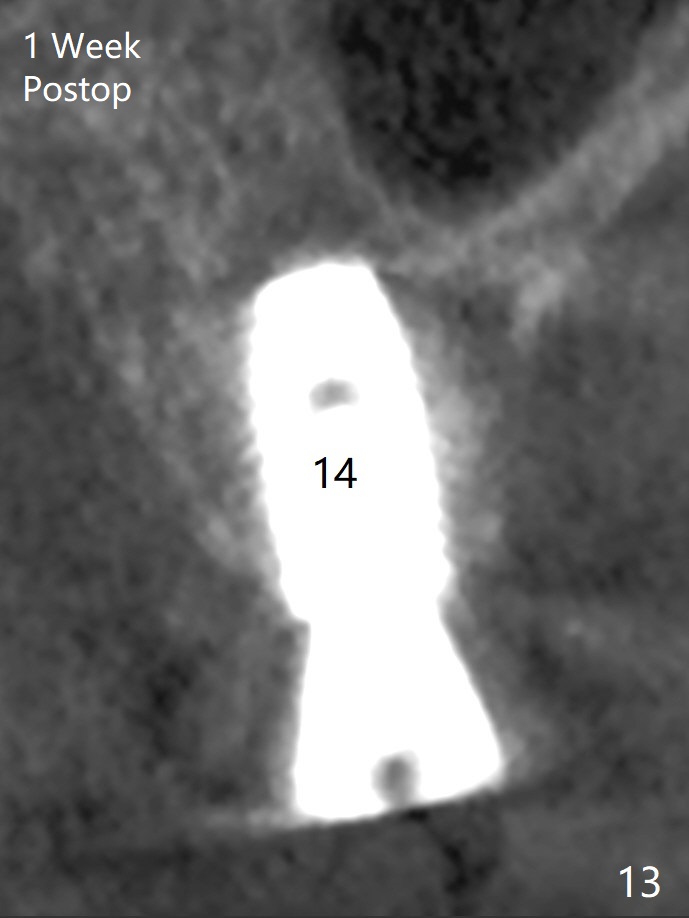
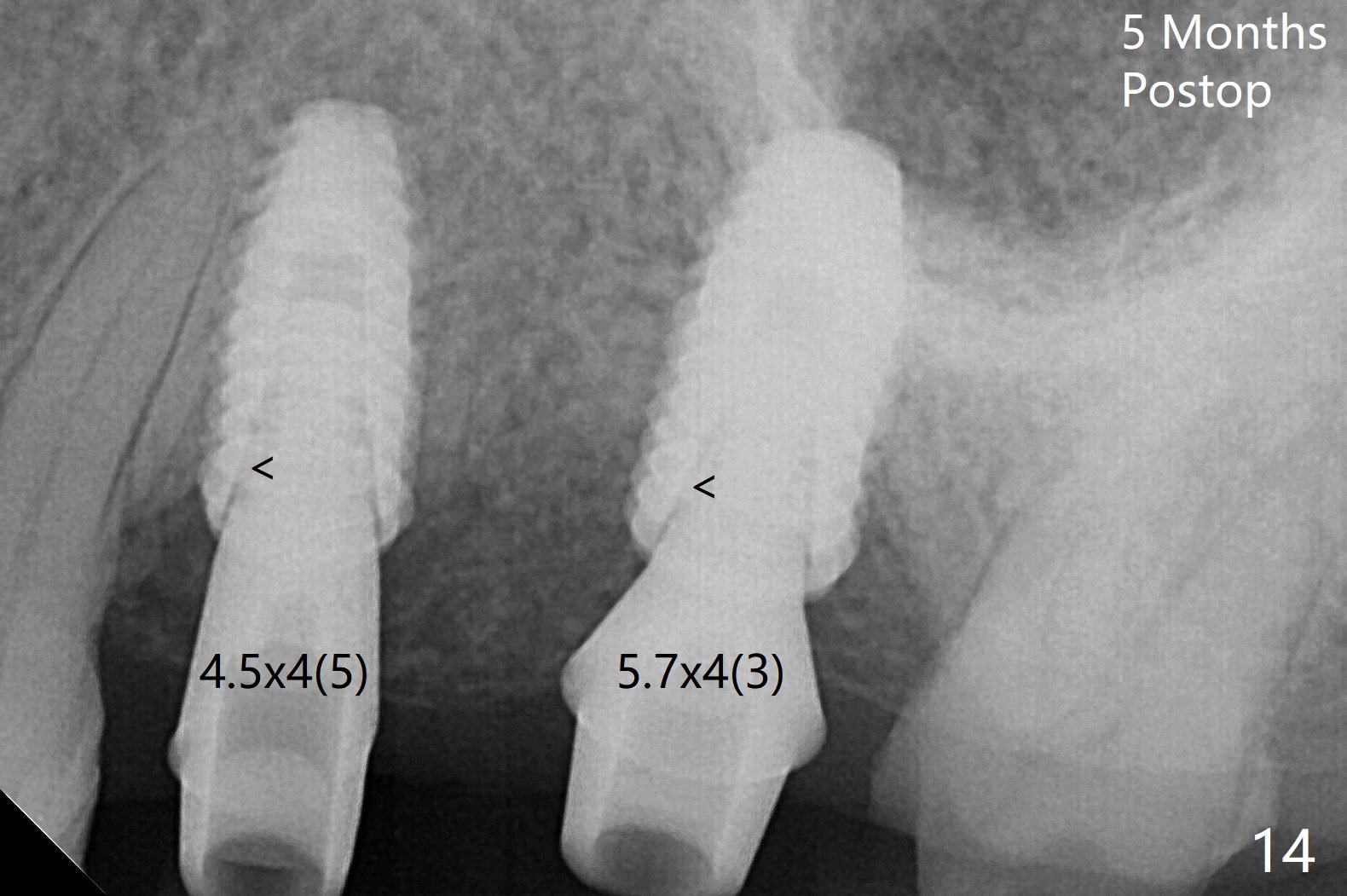
After extraction of the tooth #13 residual root, the bone in the distal wall of the socket looks white. Intraop PA rules out root structure (Fig.1 *). Osteotomy is conducted according to drill sequence. Bitewings are taken to check implant placement level (Fig.2,3). Following implant level adjustment and healing abutment installment (Fig.4,5 (*: bone graft)), the implant at #13 is found to be close the root of #12 (Fig.6 *), i.e., not parallel to the implant at #14. Introspectively, 2.2x10 mm drill seems to be long. When it touches the bone, the cylinder portion of the drill (Fig.7 red) does not engage into the sleeve (green). When it goes into the bone, it may have been deflected mesial due to the slope of the distal wall of the socket (hard bone, Fig.8 open arrow)). If a shorter drill (such as 2.2x7.3 or 8.5 mm) were used (Fig.9), the deflection would be minimal if drilling is slow (Fig.10). CT taken 1 week postop shows that the implant at #13 is approximately 1 mm near the root of the tooth #12, but the neurovascular bundle to the latter seems not to have been interrupted (Fig.11,12). The buccopalatal trajectory at #14 is within normal limit (Fig.11,13 (B: buccal)). There is no periapical radiolucency at #12 five months postop (Fig.14). However the cemented abutments are incompletely seated (<). The patient is reluctant to return for impression 17 months postop (due to coronavirus); with attention, the same abutment at #13 is reseated completely; an abutment with longer cuff and narrower diameter is also seated completely (Fig.15).
Return to
Upper
Molar
Premolar
Immediate Implant,
Trajectory
Xin Wei, DDS, PhD, MS 1st edition
05/14/2019, last revision
11/03/2020