
|
|
|
|
|
|
|
|
|
|
|
|
Socket Preser-vation for Intact Walls I
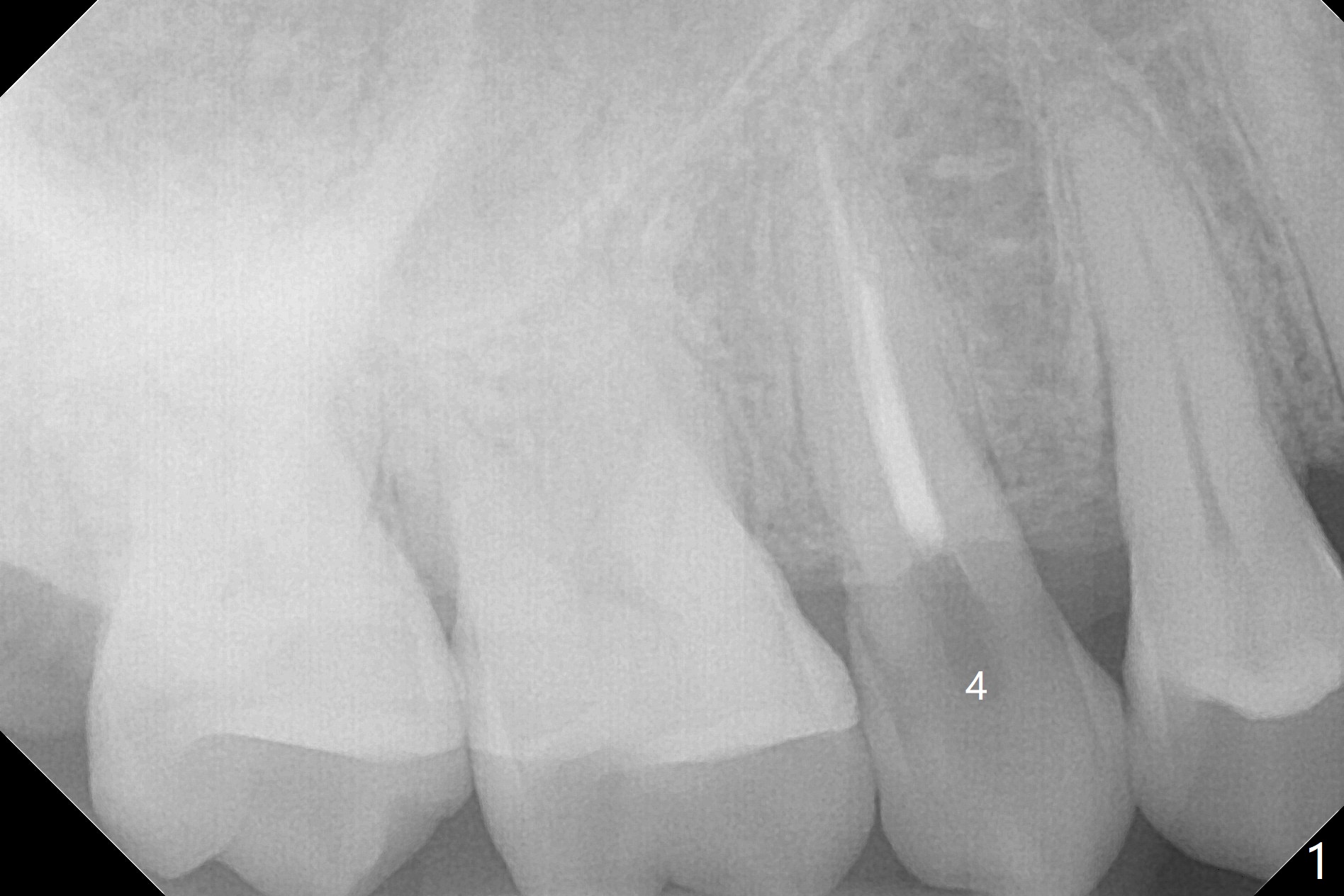
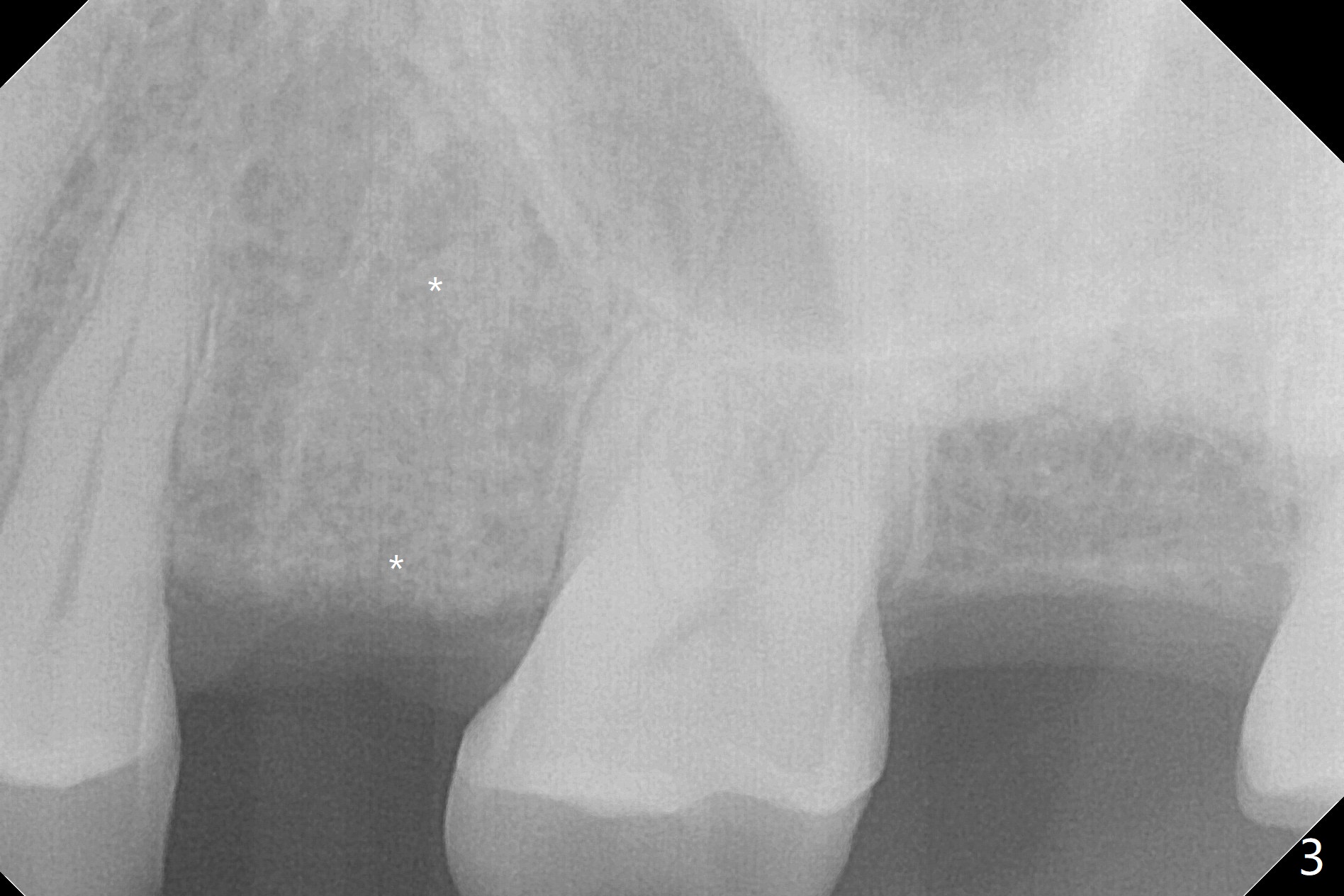
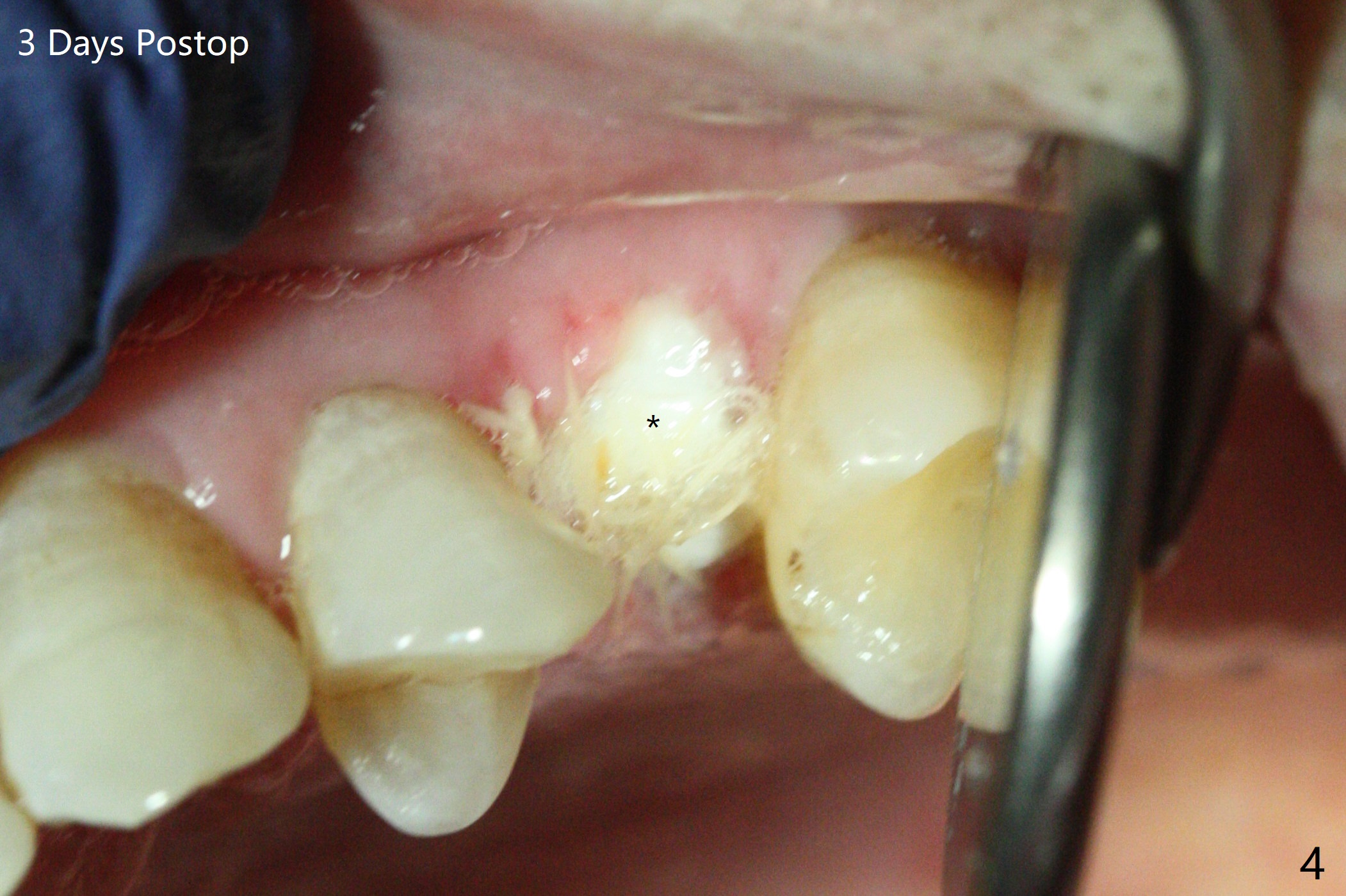
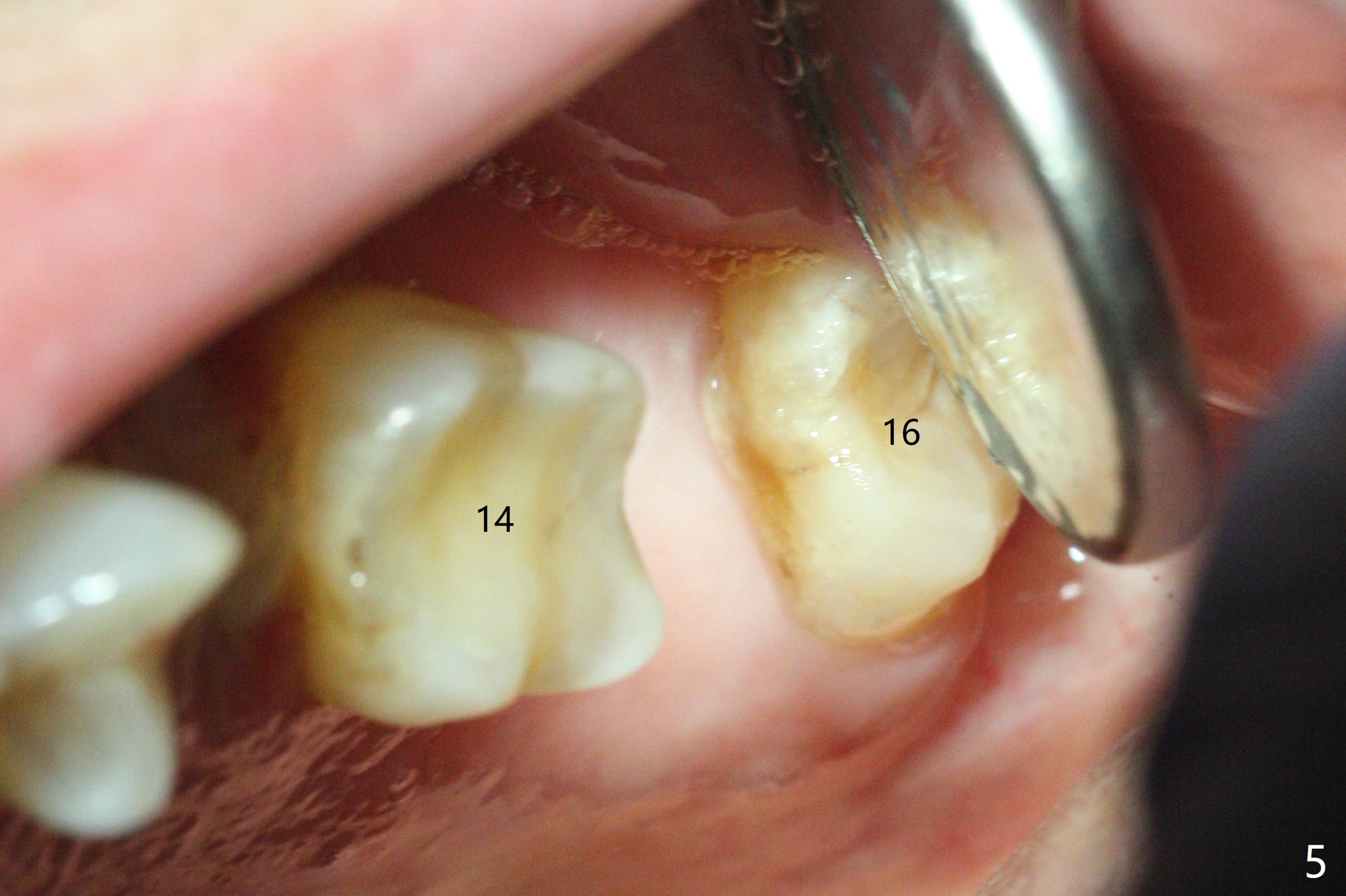
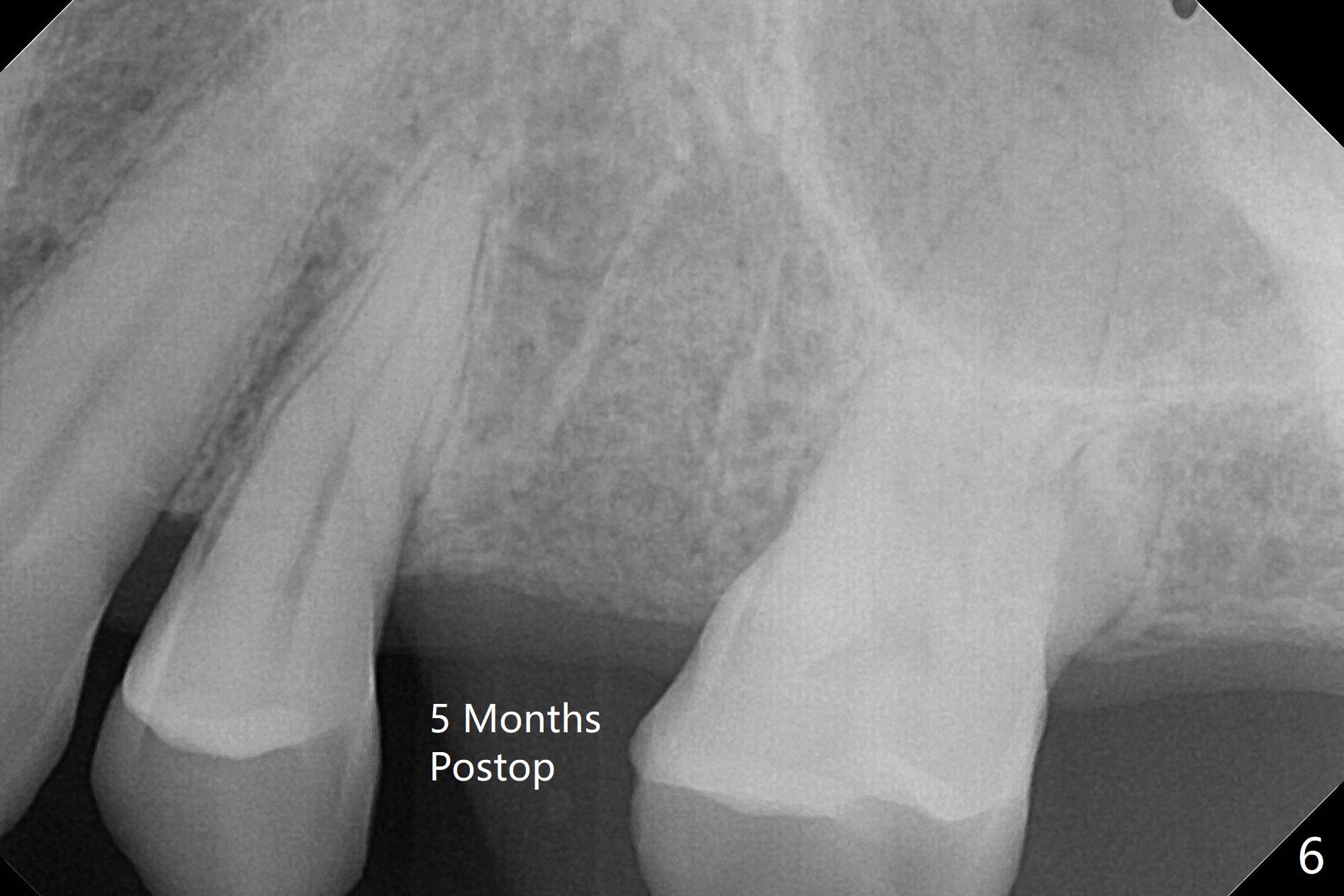
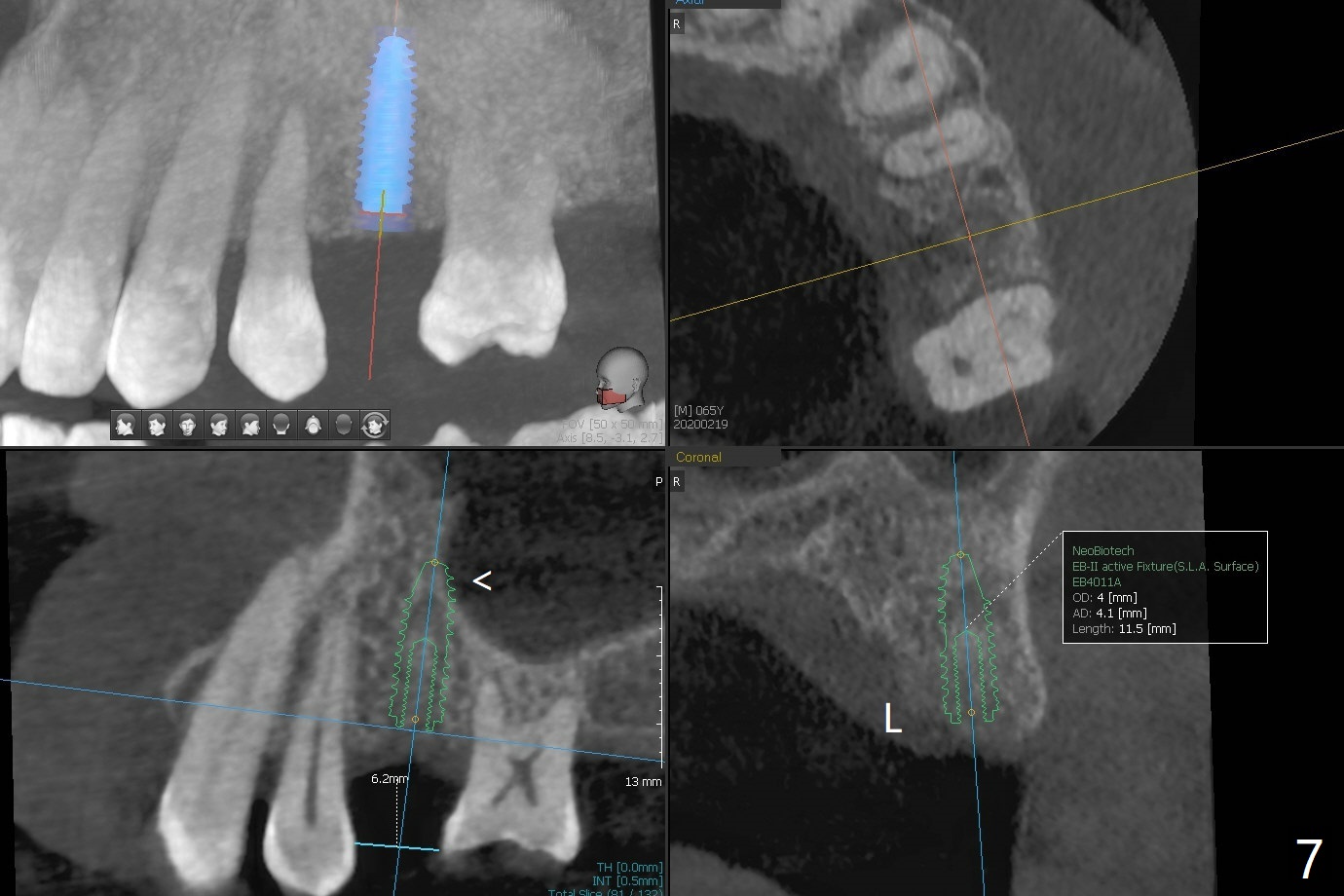
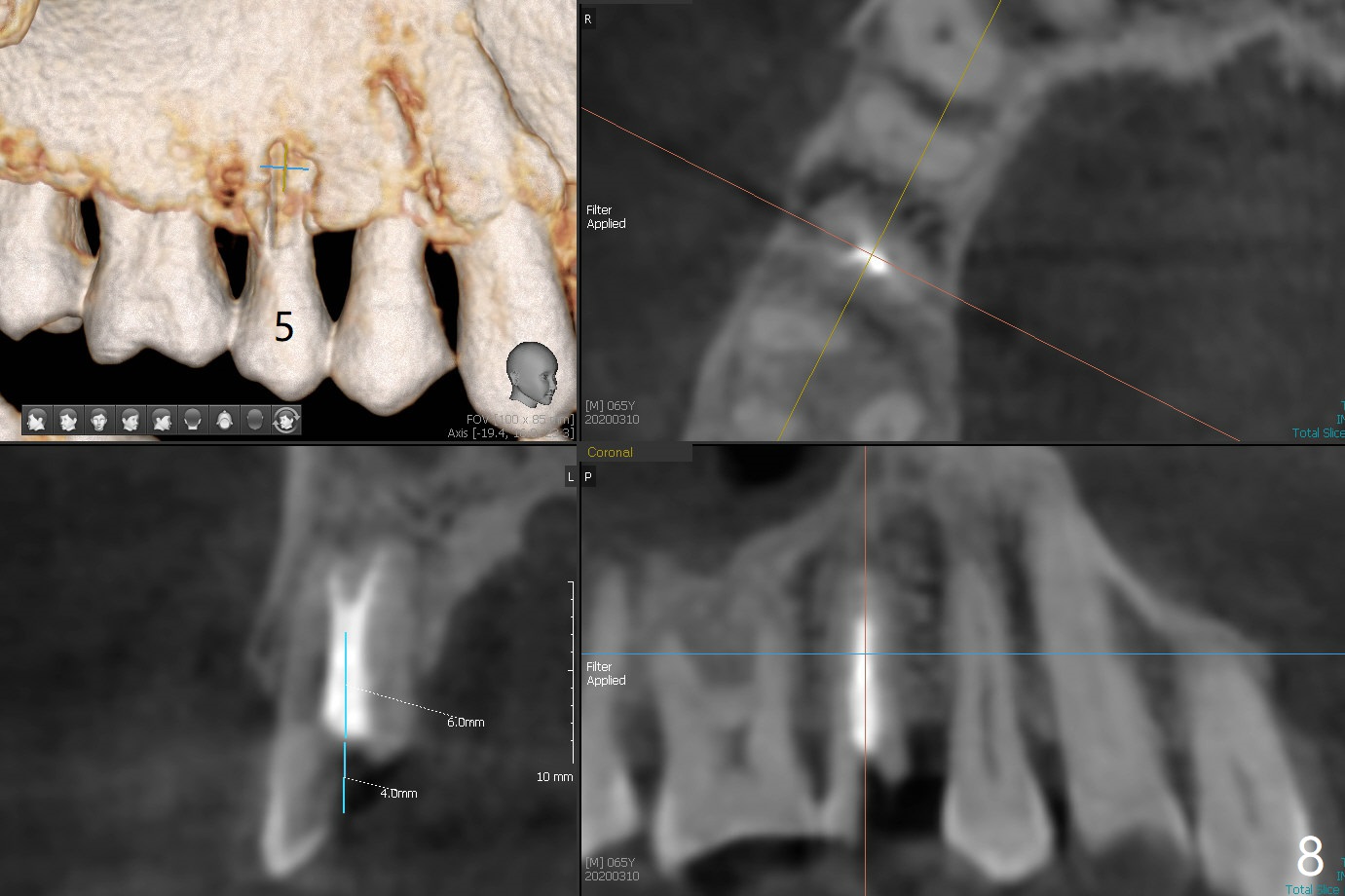
A 65-year-old man cracks 3 teeth in ~2 years (Fig.1,2 (#4, 13, 15)). The tooth #4 is sympto-matic after RCT (Fig.1); it appears that the buccal canal is incom-pletely filled (data not shown). In fact an exam 1 month later shows that the symptomatic tooth is #2 (crack), while #4 is salvageable (Fig.8). The tooth #13 has palatal sub-gingival fracture with severe pain (Fig.2 with palatal defect). In fact the title of this case is incorrect. After extrac-tion, allograft is placed (Fig.3 *) with 6-month membrane. In fact the bone graft is not packed into the apex of the socket; a condenser should have been used. The patient returns 3 days postop before leaving abroad. The 6-month membrane remains in place (Fig.4), while the ridge at #15 is minimally atrophic (Fig.5). The coronal lamina dura (mesial) becomes indistinct 5 months postop (Fig.6), suggesting the coronal socket is more active than the apical portion after extraction with bone graft. The bone graft remains in the socket. The distoapical portion of a 4x11.5 mm implant may be in the sinus (Fig.7).
Return to
Trajectory II
No Deviation
Xin Wei, DDS, PhD, MS 1st edition
09/24/2019, last revision
03/10/2020