



%2030%20Ncm.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Repair Sinus Mem-brane with PRF I
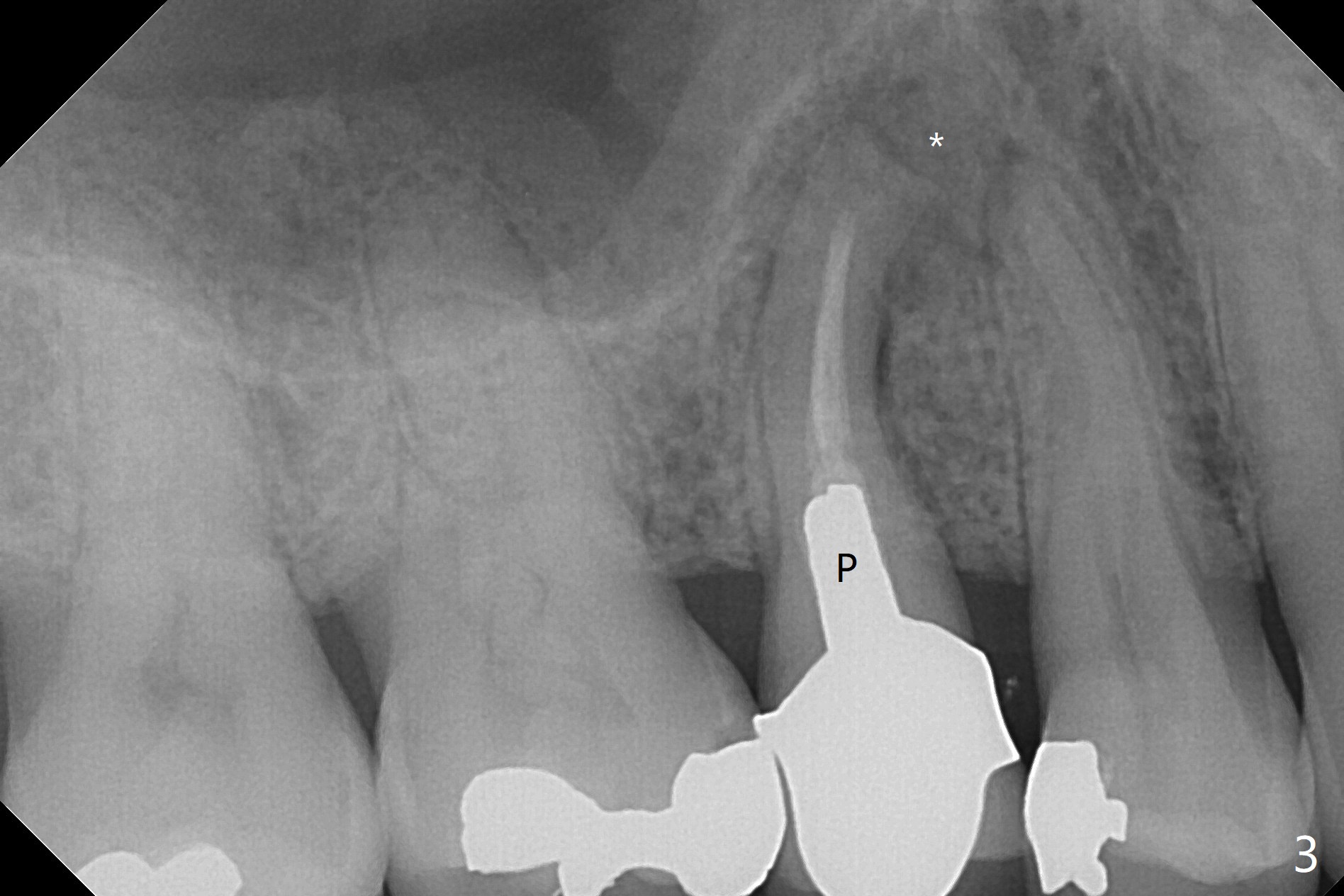
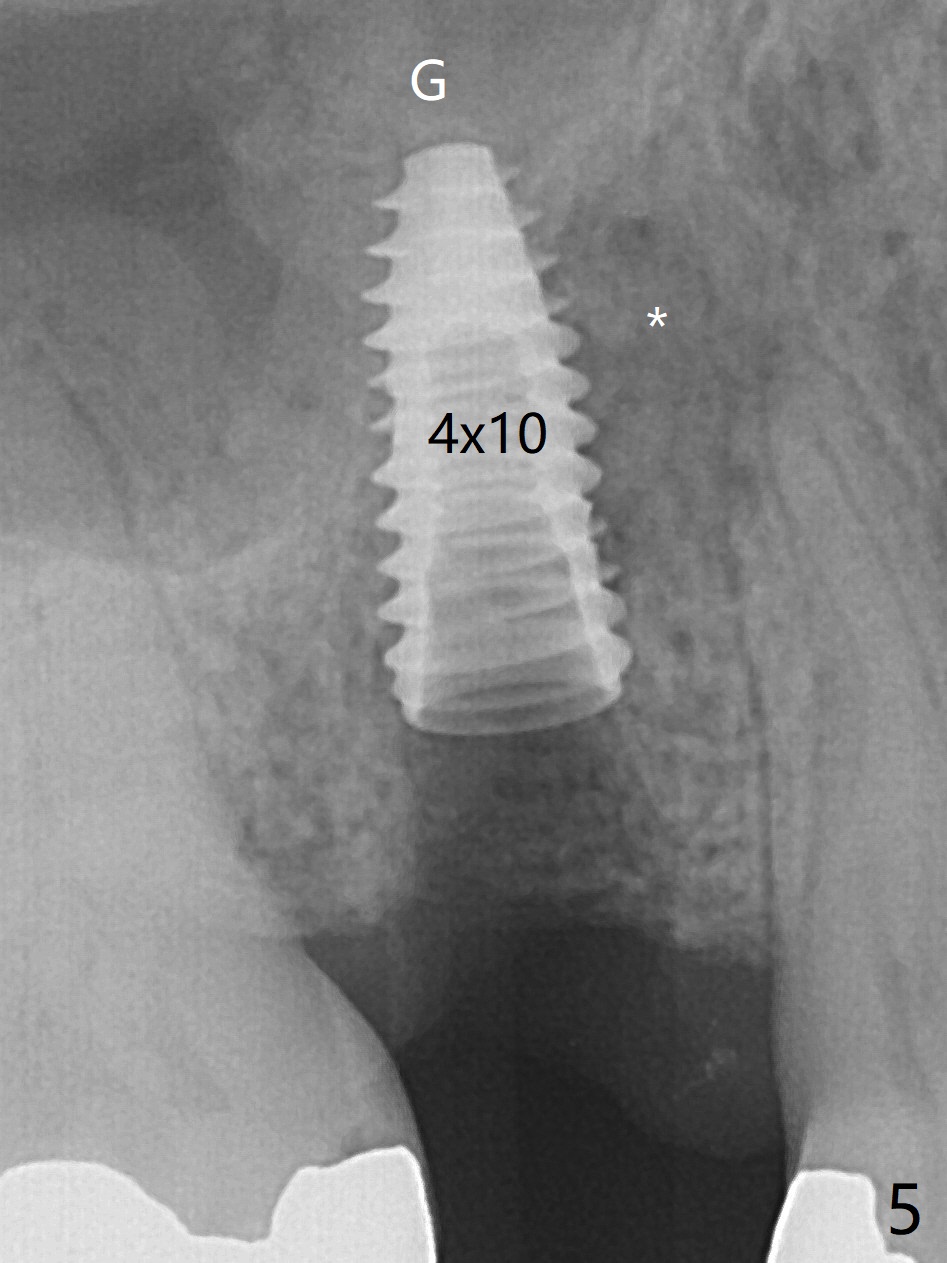
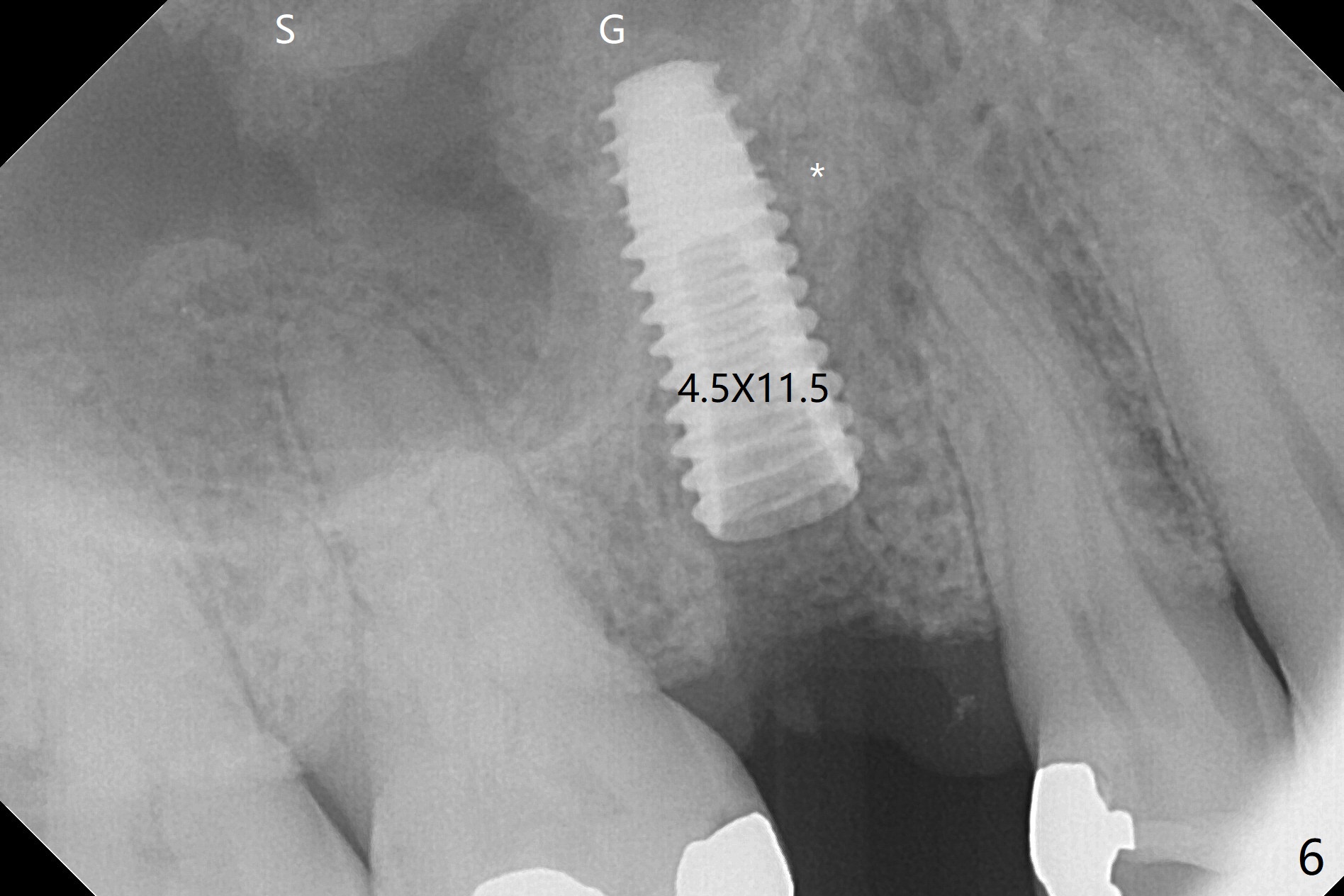
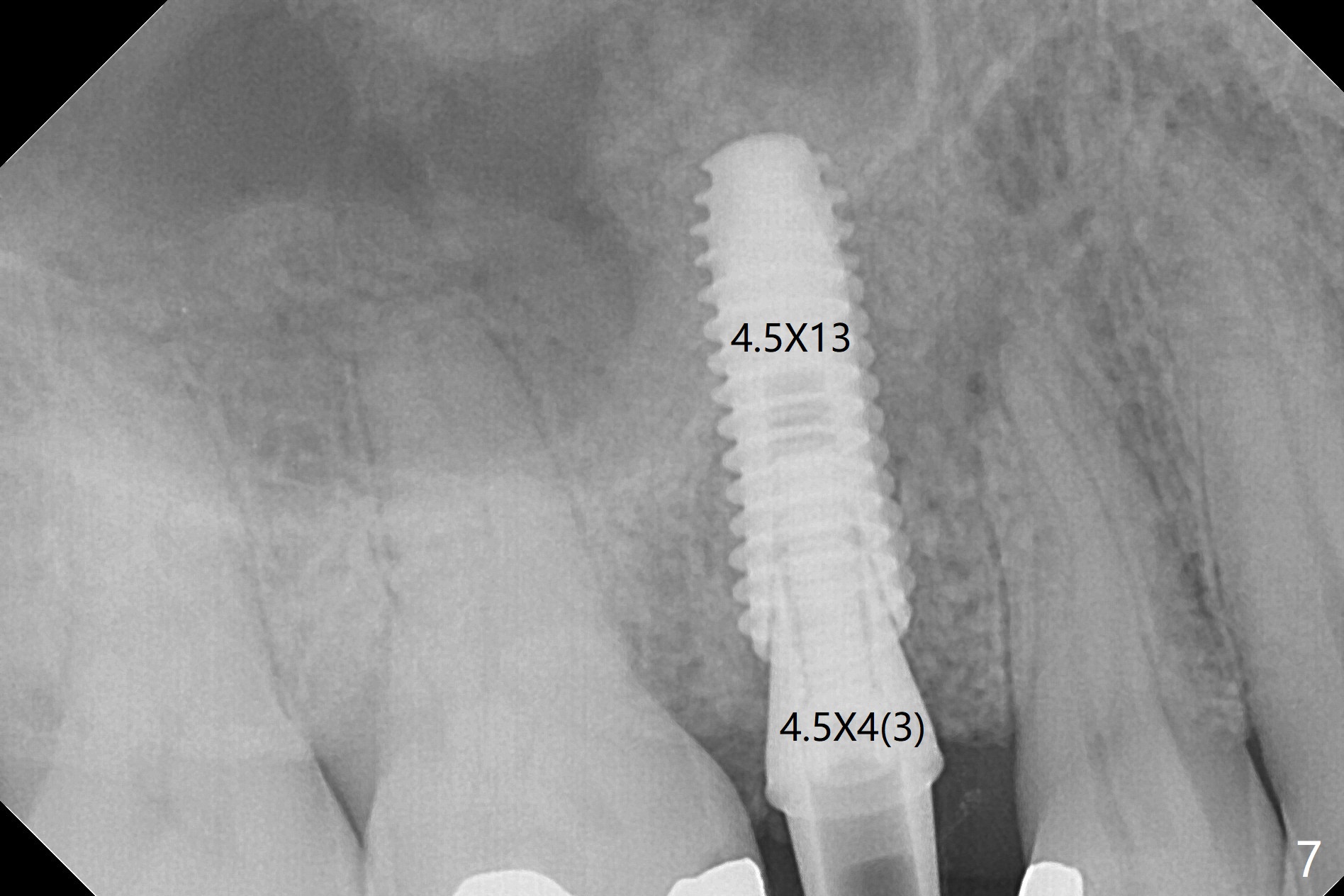
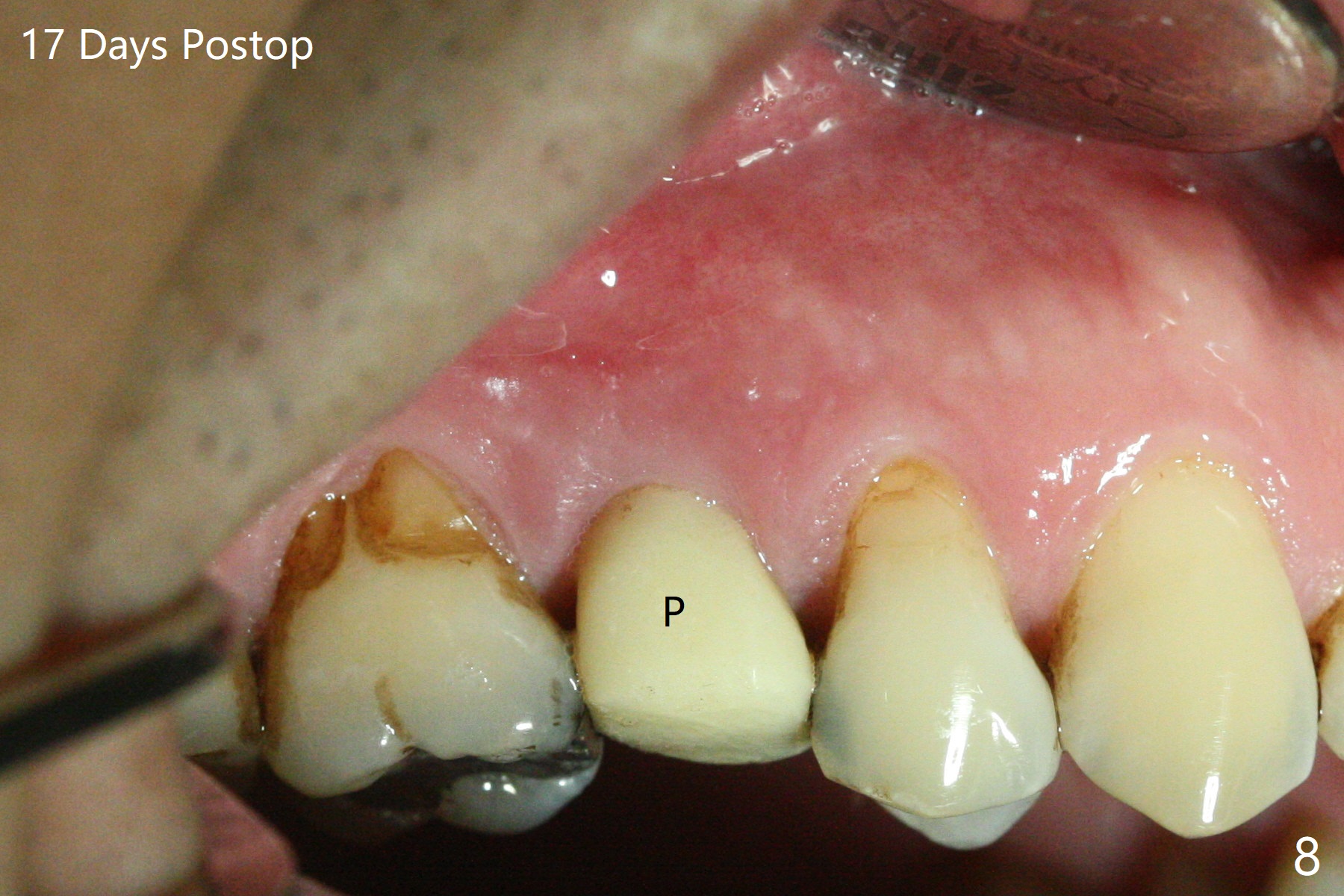
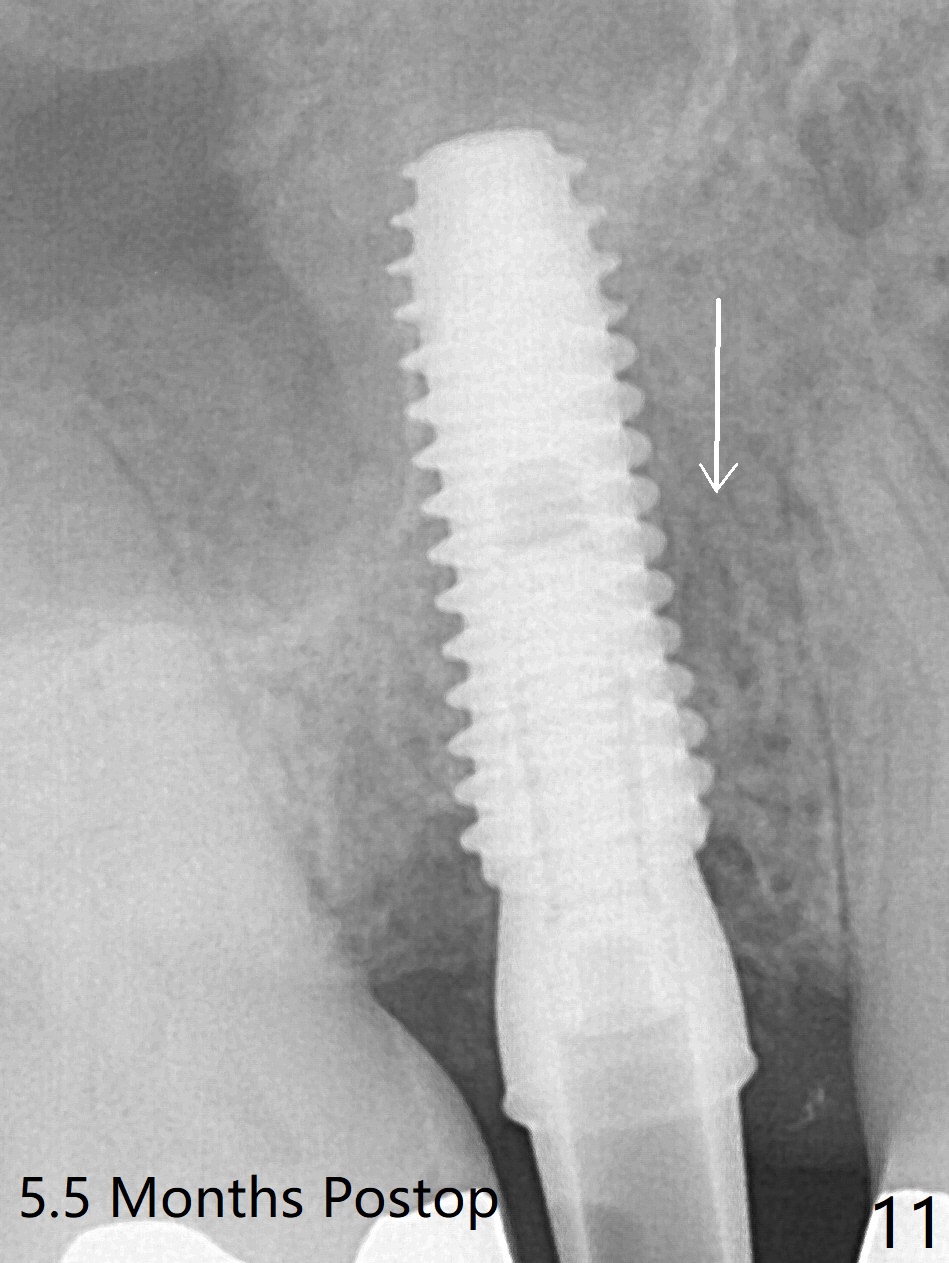
The 48-year-old man agrees to extract the tooth #4 with buccal and palatal fistulae (Fig.1,2 >) and large PARL (Fig.3 *) because of purulent discharge. The large post (Fig.3 P) is most likely associated with a longitudinal fracture. The latter is not noted until postop (Fig.4 <). Intraop finding is large amount of granulation tissue removed from the mesial apical region (Fig.3,5 *). With 10.5 mm offset, Sinus Approach Drill (19 mm) is estimated too short for sinus lift after 3x8.5 mm drill. Without careful repeated check, 2.2x10 and 2.2x11.5 mm drills are used. The sinus floor is perforated, but the membrane seems to be intact. The perforation is too small to insert PRF, but alright for allograft. Then nose blowing test shows that the sinus membrane is perforated, which seems to be repaired after placement of 2 pieces of PRF membrane, followed by another round of allograft (Fig.5 G), which is lifted by a 4x10 mm IS dummy implant. Before placement of a 4.5x11.5 mm final UF implant, allograft is placed in the 3 defective bony areas mentioned above, including the apical mesial one (Fig.6 *). But the final UF implant seems too short with non-satisfactory torque. The latter appears to be solved with the increased length of the implant (Fig.7). The gingiva around the provisional (P) is healthy without fistulae buccal (Fig.8) or palatal 17 days postop (Fig.9). A new abutment with 1 mm longer cuff is seated completely 5.5 months postop (Fig.10 < (no gap), as compared to Fig.7). The lower portion of the mesial defect seems to have been repaired (Fig.11 arrow, as compared to Fig.7).
Return to Upper Premolar Immediate Implant, Trajectory II
Xin Wei, DDS, PhD, MS 1st edition 09/27/2019, last revision 03/13/2020