






|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|||
|
|
|
||||
Bone Level Immediate Implant
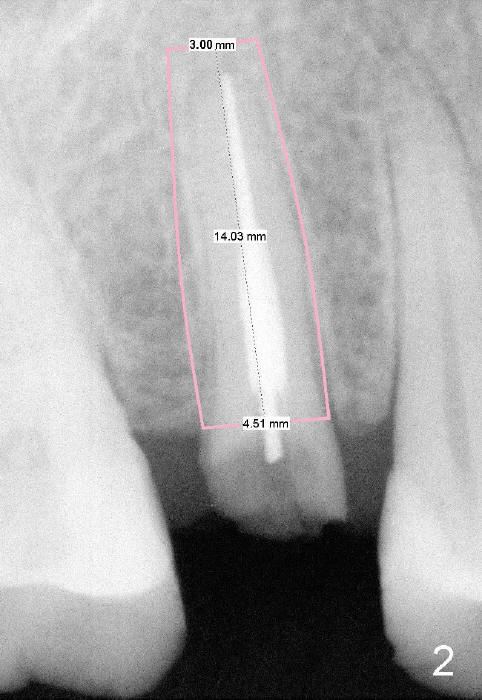
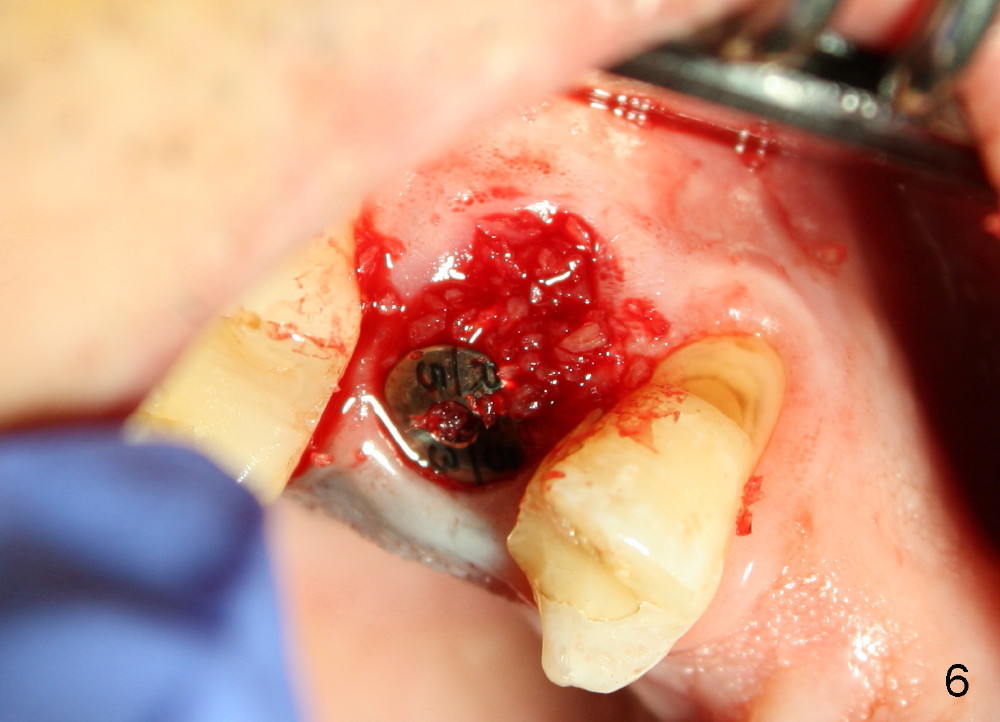
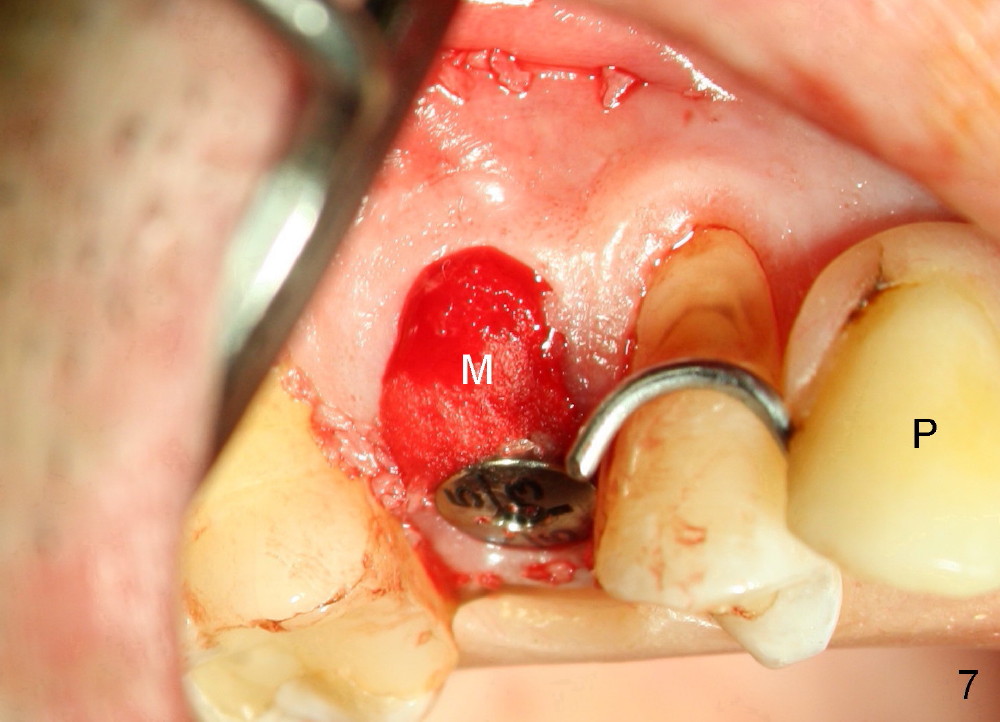
A 51-year-old man has several missing teeth in the maxilla restored by a partial denture. The tooth #4 fractures (Fig.1) and is planned to be restored by an implant (Fig.2 design: 4.5x14 mm). Immediately post extraction, osteotomy is initiated by a 2.0 mm pilot drill at the depth of 14 mm (3 mm into new bone, Fig.3). Finally a 4.5x14 mm SM (submerged) implant is placed with insertion of a 5.2x5(3) mm healing abutment (Fig.4). Mixture of autogenous bone and demineralized cortical allograft is placed in the gap between the buccal plate and the implant/abutment (Fig.6), covered by collagen membrane (Fig.7 M; P: partial denture). In fact the membrane is fixed between the implant and the healing abutment lingually. The wound is finally covered by perio dressing (Fig.5 ^). The patient returns 5 days postop. The perio dressing is removed unintentionally. It appears that the membrane has started to be resorbed (Fig.8).
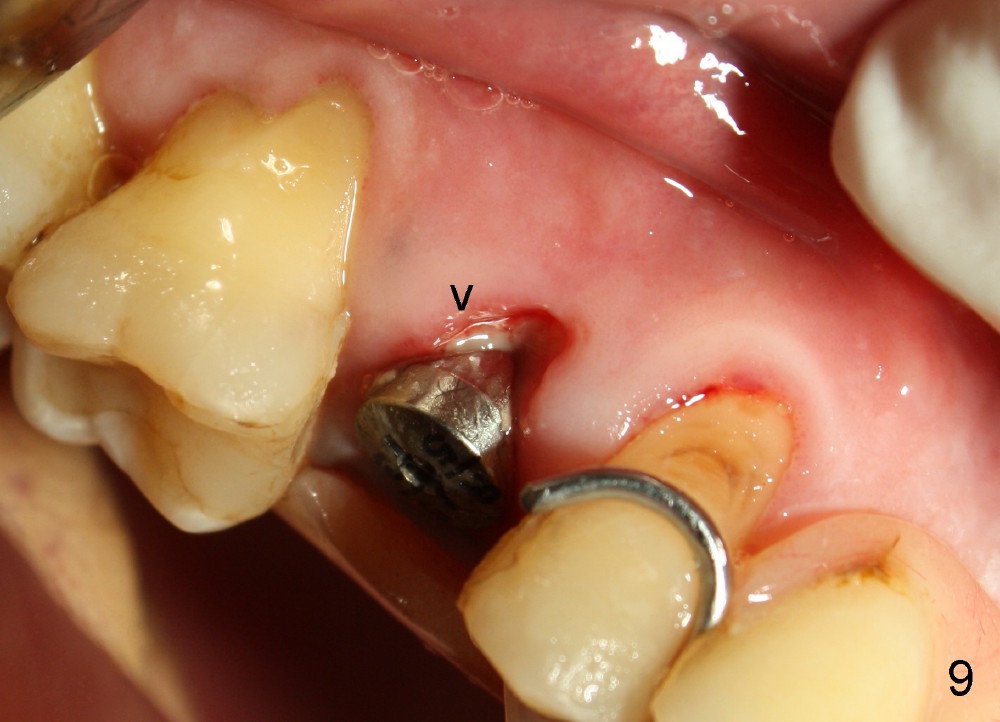
By 2 weeks postop, there is granulation tissue formation around the buccal aspect of the implant/abutment (Fig.9 arrowhead). The wound (gingival recession) appears to shrink (as compared to Fig.7,8). The patient feels great and wonders why no crown is fabricated. Once the granulation tissue is mature, a provisional crown will be made. The reason that no immediate provisional is provided in this case is that there are several missing teeth and that the implant may be overloaded. If there is no overloading issue, immediate provisional is preferred to the membrane. The provisional can provide with more secure coverage over the bone graft.
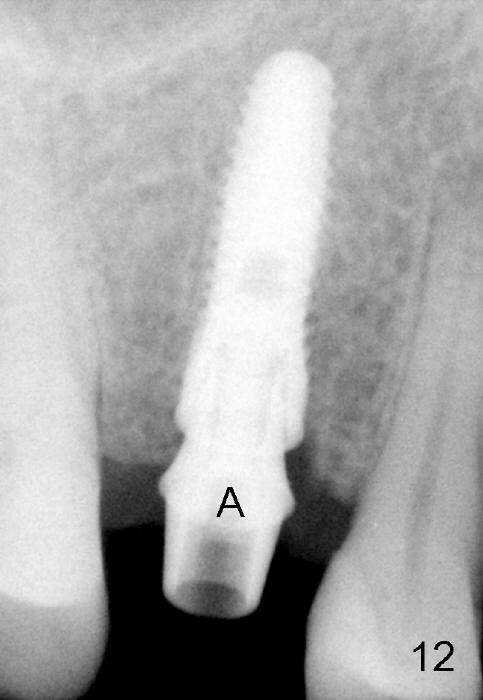
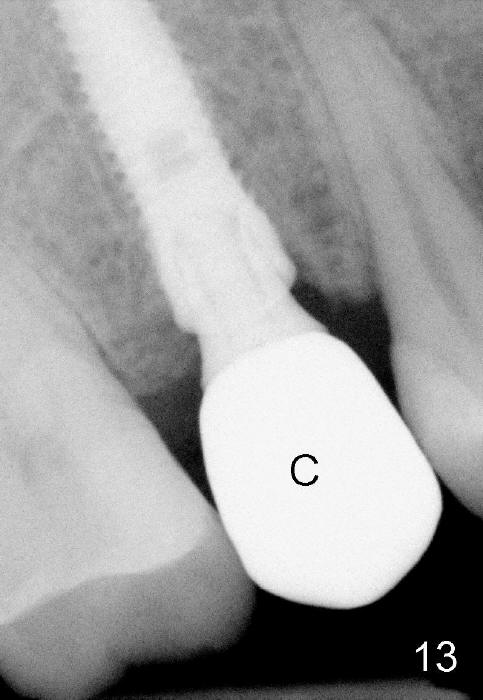
Due to insurance termination, restoration has to be done 2 months post implantation. Both the soft (Fig.10 *) and hard (Fig.11) tissues heal normally. A cemented abutment is placed (Fig.12 A). Fig.13 is taken 5 months post cementation. There is no bone resorption.
Return to Professionals,
Upper Bicuspid Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 01/20/2014, last revision 12/21/2014