




,%2030.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sensor Holders & IAC
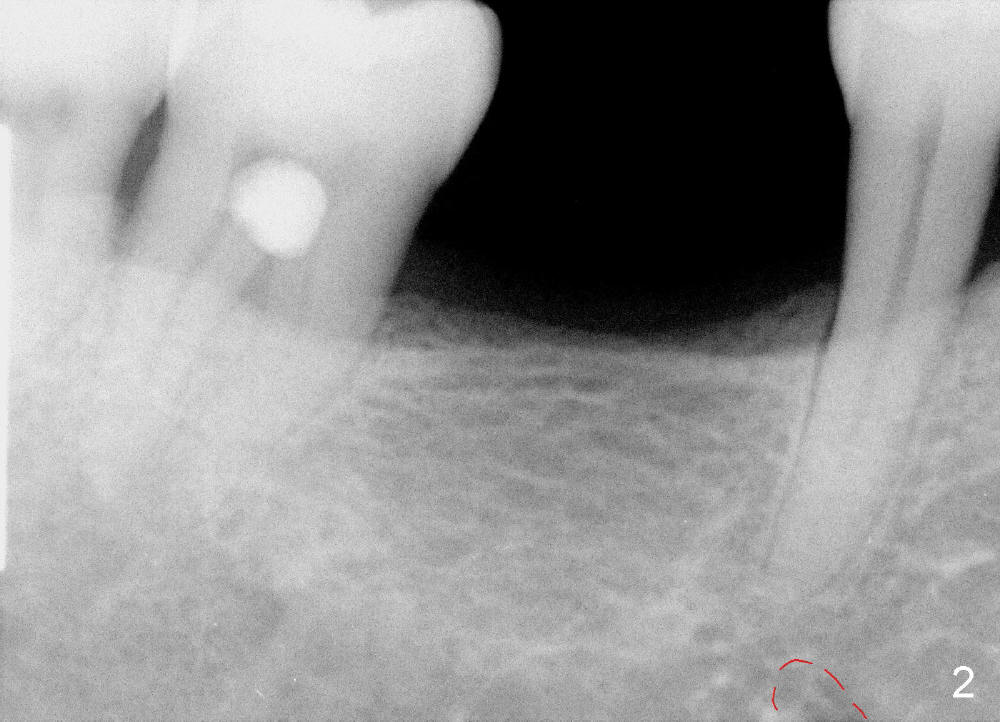
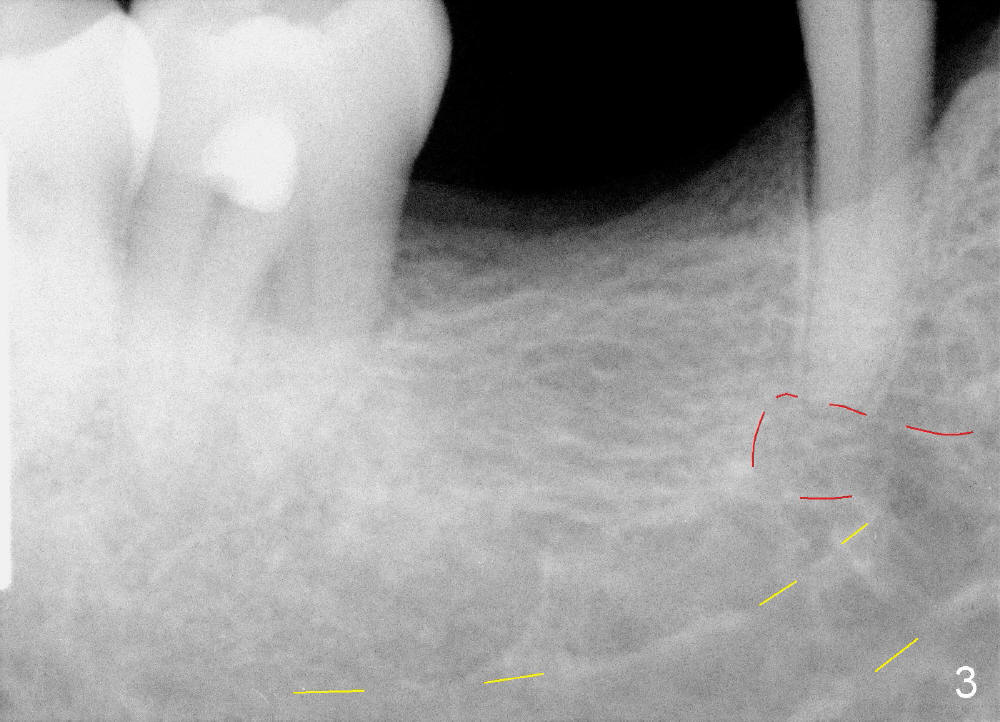
It is critical to identify the inferior alveolar canal (IAC) prior to and during implantation. A 59-year-old man requests implant for the lower right 1st molar (Fig.1). PA taken with a regular sensor holder does not show IAC except part of the mental loop (Fig.2 red dashed line), whereas the one taken with an endo sensor holder does show IAC (Fig.3 yellow dashed line).
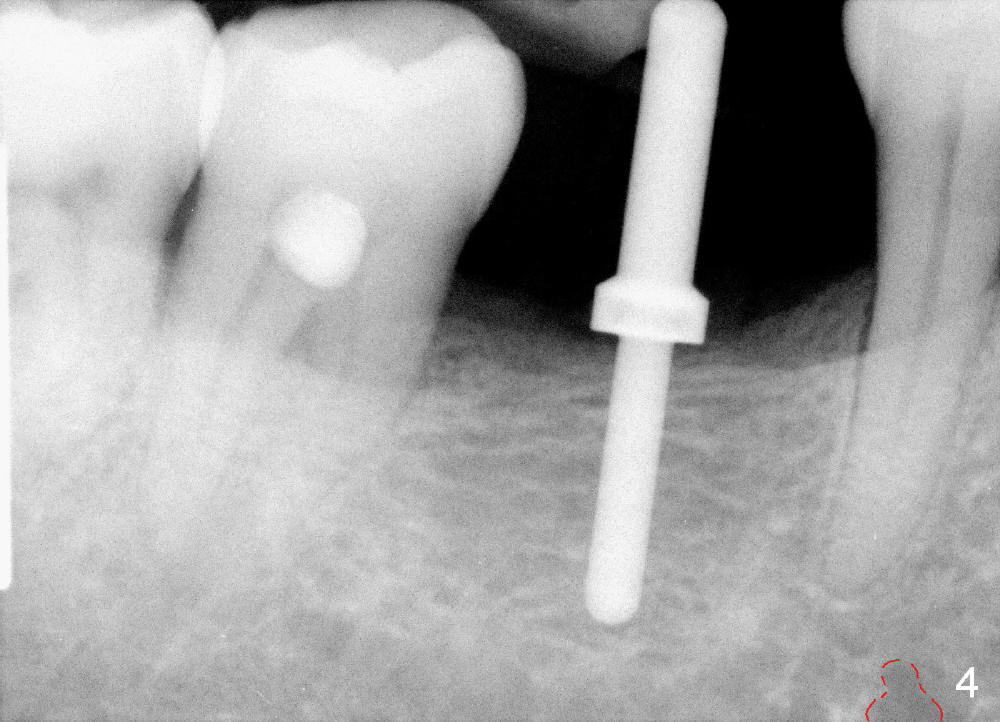
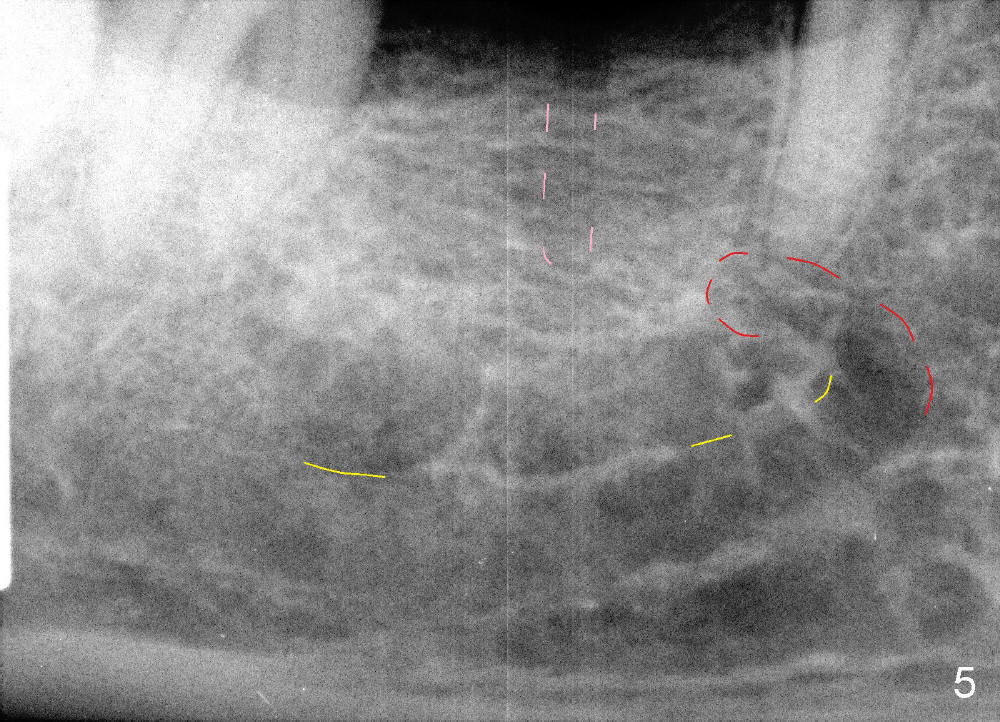
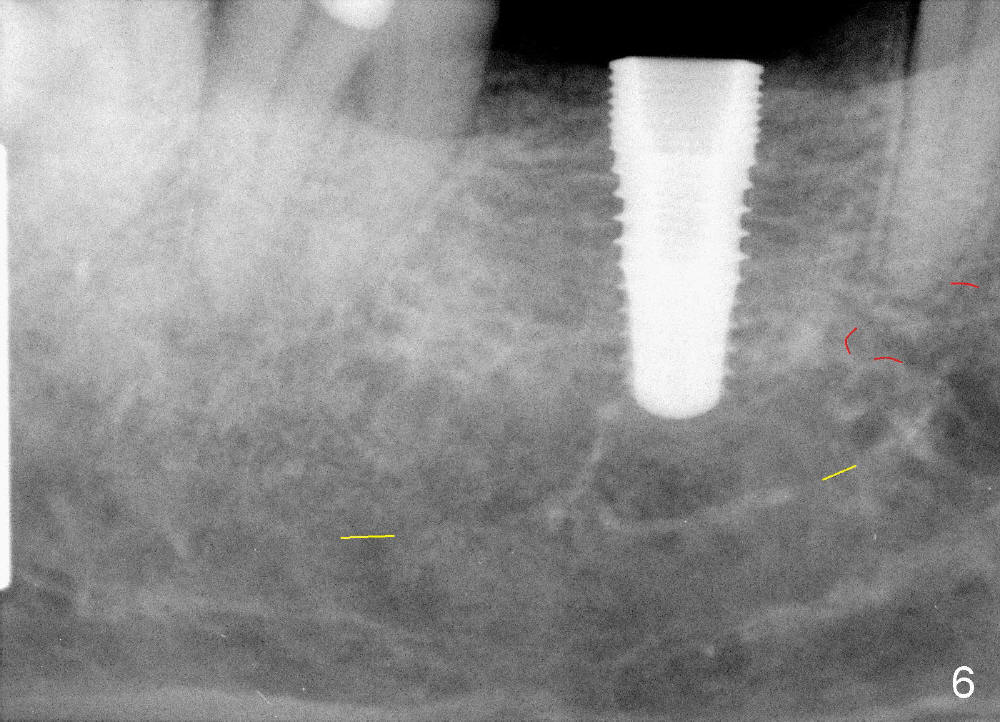
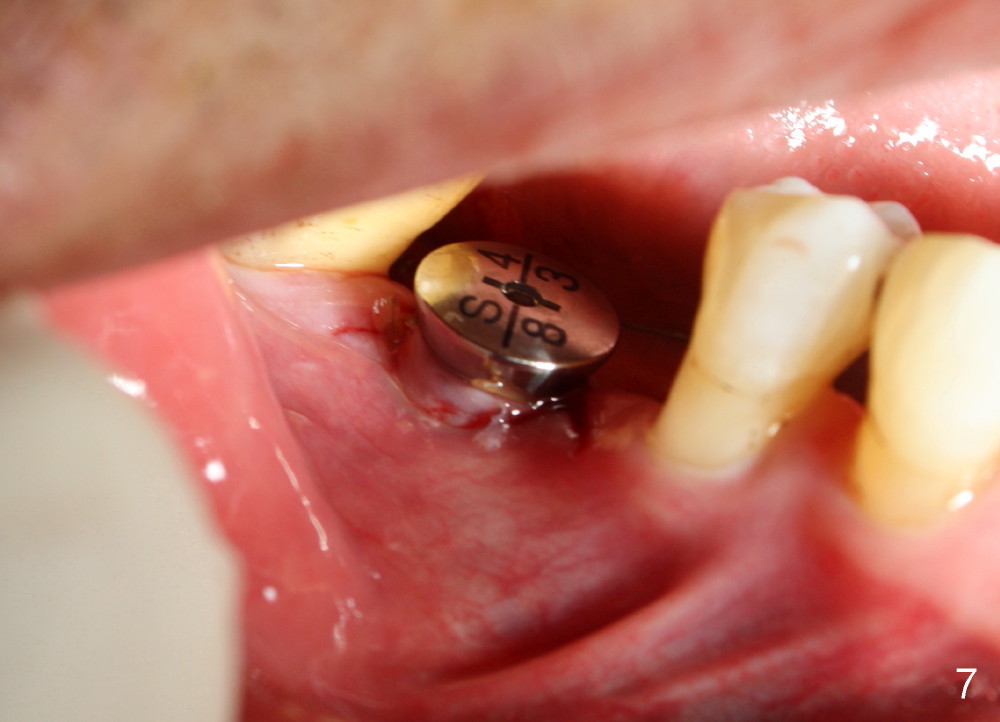
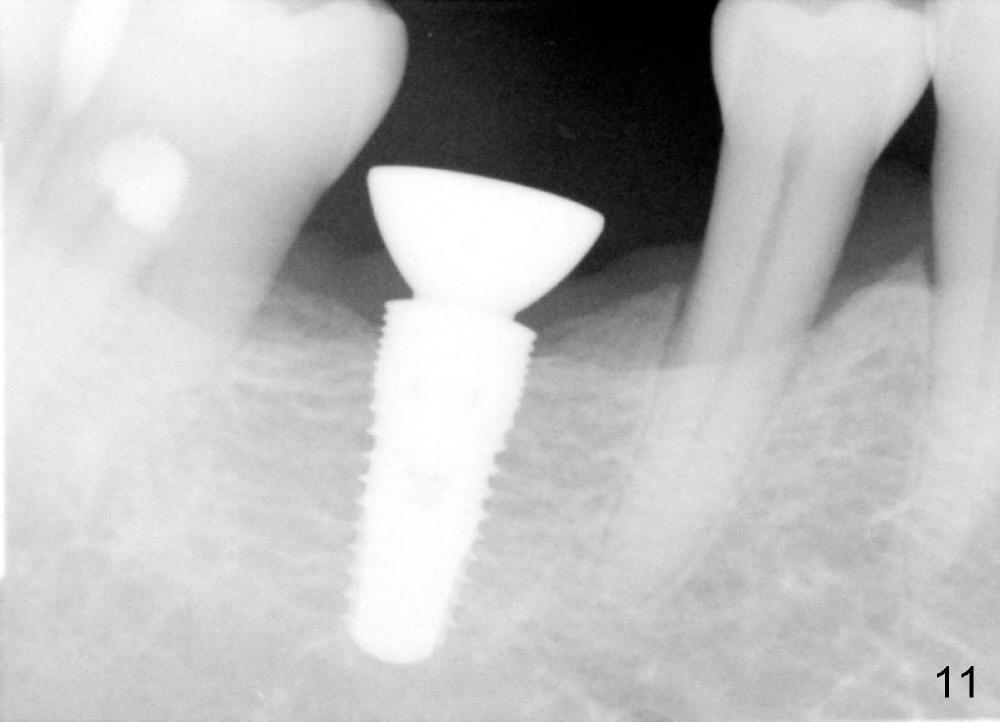
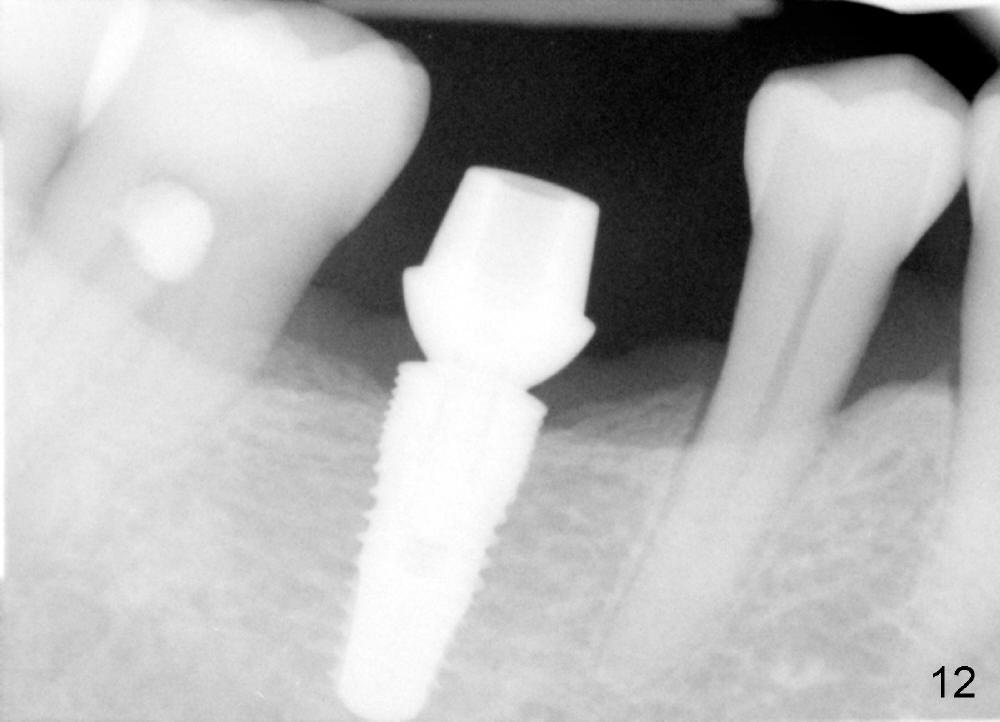
When a positioning pin is placed in the osteotomy with 10 mm deep, the sensor cannot be placed deep enough because of pin interference so no IAC is visible (Fig.4). When the pin is removed and the sensor is placed low enough, IAC is clearly shown, but the osteotomy is barely visible (Fig.5 pink dashed line). With information obtained from pre- (Fig.2,3) and intra- (Fig.4,5) op PA, twelve mm of osteotomy appears to be appropriate. A final implant (5.3x12 mm) is placed with separation from IAC (Fig.6, insertion torque 50 Ncm). A healing abutment is placed (Fig.7,8), which helps retain perio dressing (Fig.9). Two weeks later, the gingiva heals around the abutment (Fig.10). Four months postop, the implant appears to osteointegrate (Fig.11). A cemented abutment is placed (Fig.12). With supragingival margin, oral hygiene is easily maintained (Fig.13). Due to delayed placement, the gingival embrasure is extremely large (*). The issue is much less with immediate implant.
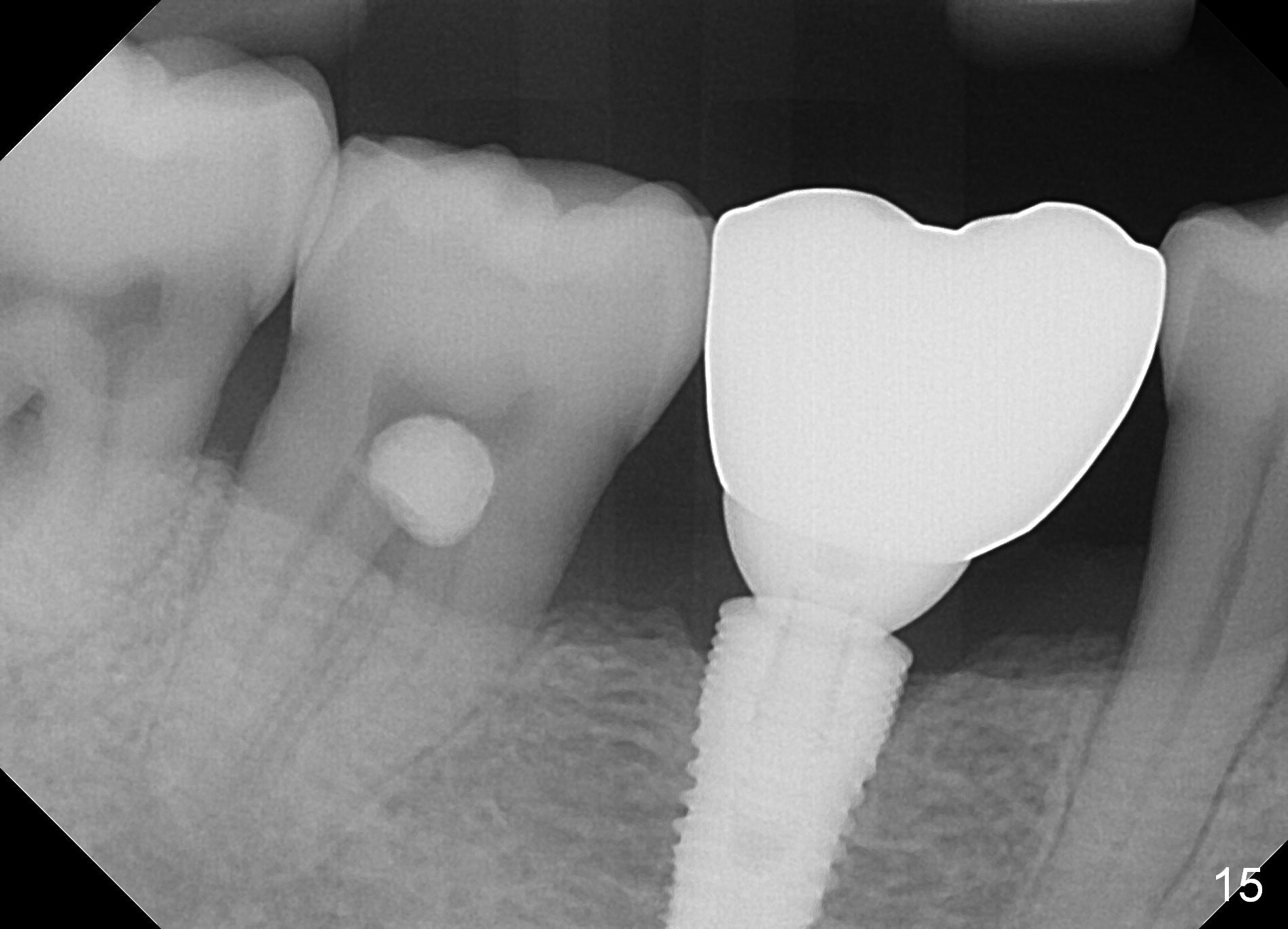
The patient returns for recall 9 months post cementation. His concern is inability to masticate hard on the right side. The tooth #29 has mobility I with bone loss (Fig.14 ^). Six months later, the symptom disappears. In fact occlusal equilibrium should be provided. There is no bone loss 2 years 2 months post cementation (Fig.15).
Return to Professionals,
Trajectory
Xin Wei, DDS, PhD, MS 1st edition 10/06/2014, last revision 04/15/2019