
|
|
|
|
|
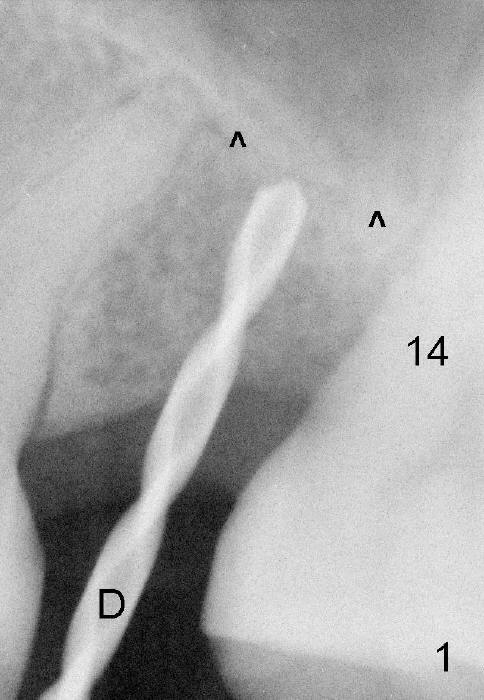
Why is Implant Deviated?
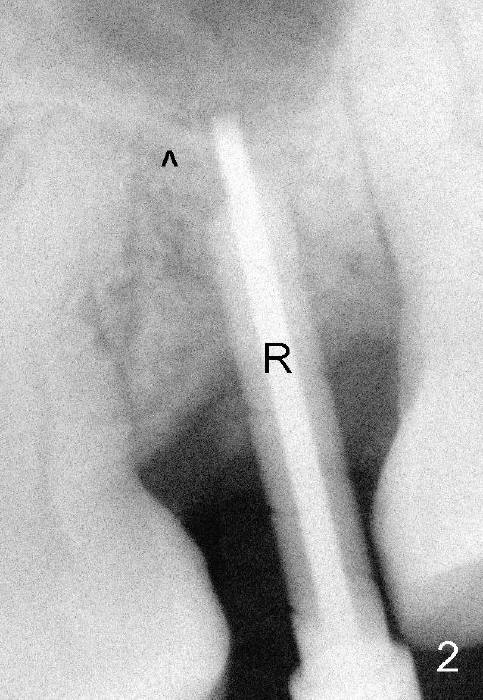
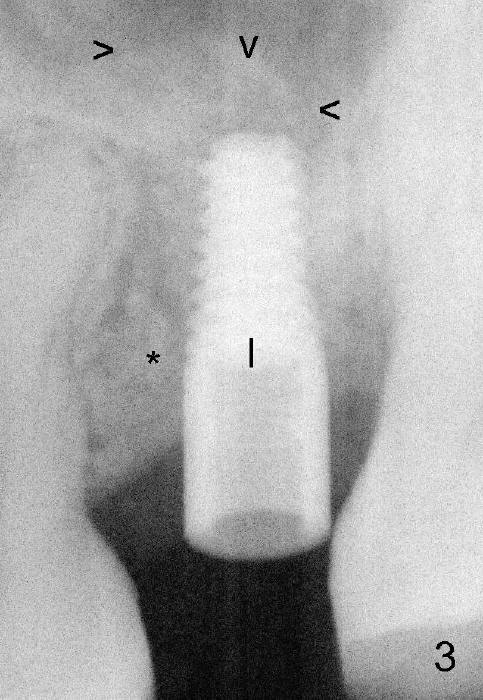
Exam immediately prior to surgery shows that the edentulous ridge is wide buccolingually. The mesiodistal space is less than 6 mm. It appears that a 4 mm implant is appropriate. Two piece implant is chosen over a one-piece one, because of large surface area of the former. After local anesthesia, a 3.5 mm tissue punch is used for access to the bone. A 1.5 mm pilot drill initiates osteotomy 8 mm in length (Fig.1 D). The drill is more or less in the middle of the edentulous space and 1 mm coronal to the sinus floor (^). Then a 2 mm pilot drill, 2.5 mm and 3 mm reamers are used to enlarge osteotomy (8 mm deep). Mixture of autogenous bone and Osteogen and 2.5 mm Bicon osteotome are used for sinus lift. The osteotome does not reach the intended depth of 10 mm. The osteotomy is extended with the 2 mm drill and 2.5 mm reamer (Fig.2 R) to barely perforate the sinus floor. When a 4x11 mm implant is being placed, it tends to deviate distally. The implant is backed up twice: initially it appears to lean mesially, but as it is seated deeper, it is deviated distally again (Fig.3). An immediate provisional has to be fabricated to prevent the space from further narrowing. A 3.5x3 mm abutment is placed. The mesial surface of the tooth #14 (Fig.4 black area) is trimmed for restoration. Why is the implant deviated? How to fix it?
Return to Professionals,
Implant Failure,
Upper Bicuspid Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 01/14/2015, last revision 01/14/2015