Full-mouth Implants
Mr. Fan is 65 years old. He has had upper and lower
overdentures for ten years. Both of them are loose. He also complains pain
associated with upper distal abutments: #8 and 13. Exam shows generalized
advanced chronic periodontits (Fig.1, 2 (upper anterior PAs), 3 (lower anterior
PAs). All of the remaining teeth are nonsalvageable. The width of
the alveolar ridges is adequate (Fig.4 and 7). The ridge height of the
mandible is sufficient, whereas that of the maxilla is questionable (Fig.1).
The patient prefers fixed prosthetics. We plan to place as many as 24
implants in stages.
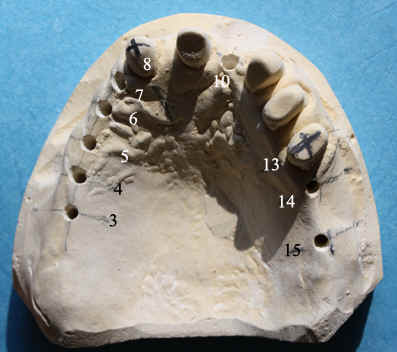
First, do model surgery, use existing information to place
implants in ideal position (Fig.5-10), and finish stents for cone beam CT (Fig. 11,
12).
Second, extract #8 and 13, do scaling & root planing, and
reline overdentures. Stress oral hygiene. Wait 2 months for wound to
heal before 1st staged implant placement.
Third, do sinus graft or lift if indicated by cone beam.
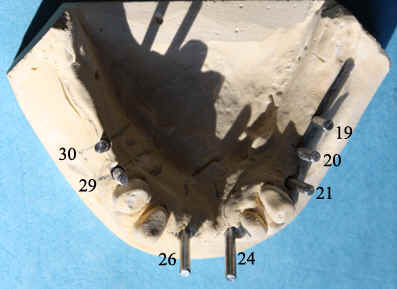
Fourth, place implants at #3-8, 11, 13, and 14 for upper (Fig.5)
and 19-21, 24, 26, 29, and 30 for lower (Fig.8). If the left sinus floor
is low at #14, we plan to place implants at #13 and 15 and make a fixed partial
denture (FPD) (Fig.5). The lower anterior implants are tilted labially due
to the presence of a ridge undercut (arrowheads in Fig.9). Fig.10 shows
the lateral view of the upper model surgery.
Fifth, uncover 3-4 months later, change tooth-supported
overdentures into implant-supported ones, possibly using o-rings, and extract
remaining teeth.
Sixth, two months later, place implants at #9, 11, 12, 22, 27
and 28.
Seventh, implant-supported crowns and FPDs.
01/11/2010