|
|
|
|
Immediate Functioning?
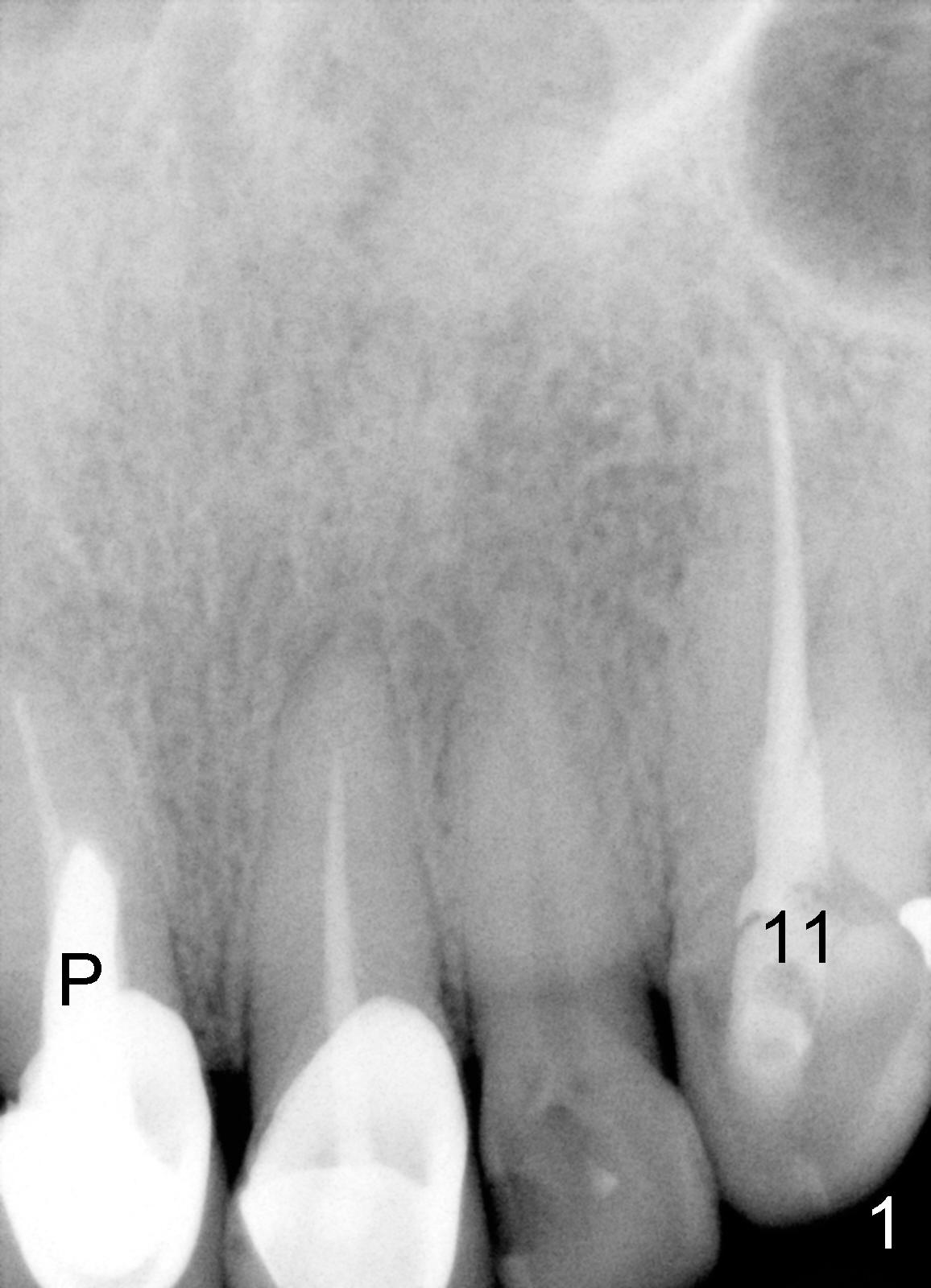
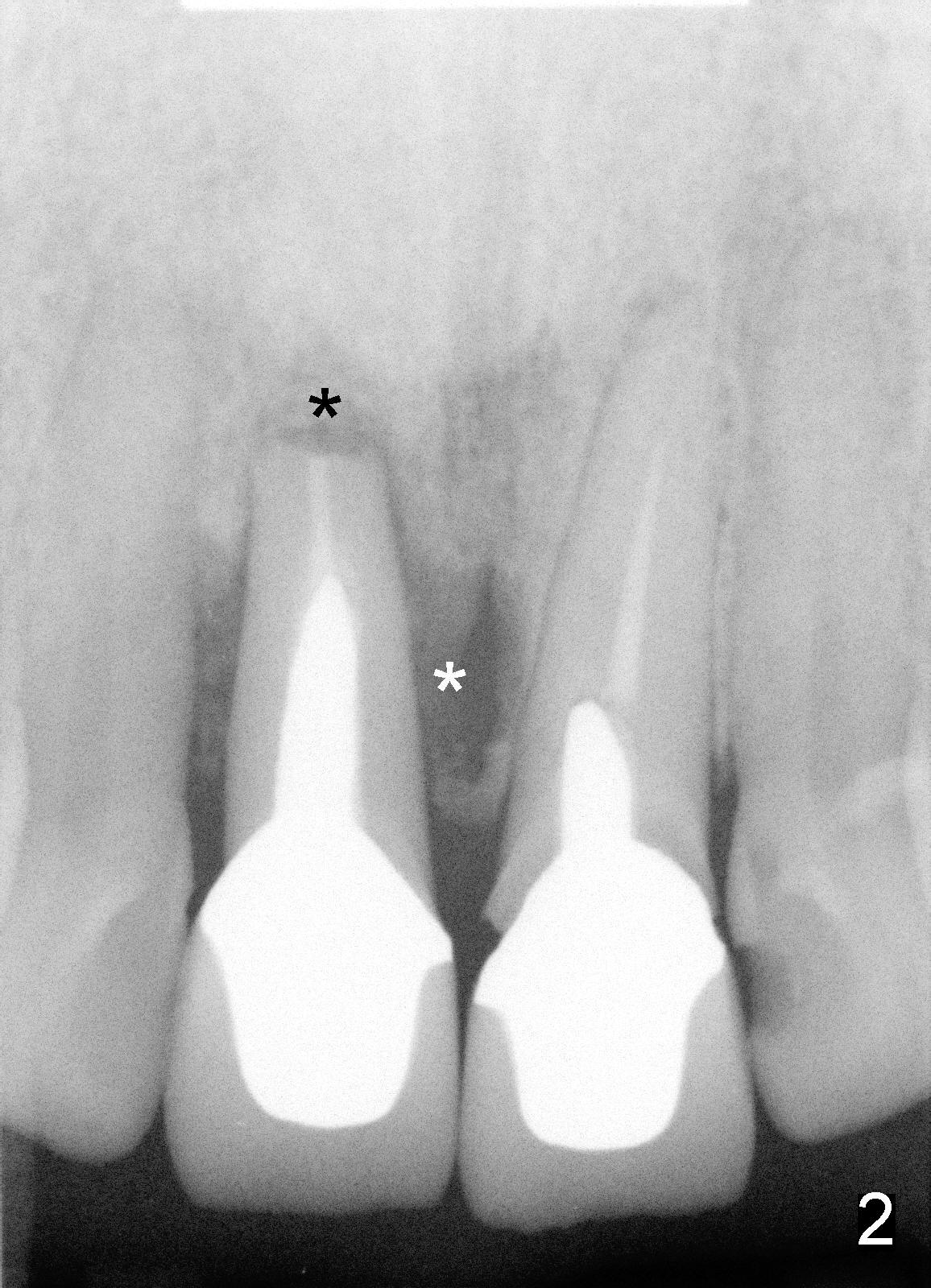
Fifty-five-year-old lady became my patient 6 years ago because of RCT for #11 (Fig.1). At that time, #8 had a large and malpositioned post (P), whereas #9 did not have a post. Since then, she has returned for recementation of crowns for several times. Recent X-ray shows that #8 has had apicoectomy (black * in Fig.2) and large radiolucency on the side of the root (white *, which was absent 6 years ago, as compared to Fig.1). The tooth #9 crown is loose with subgingival margin. It appears that both incisors are nonsalvageable.
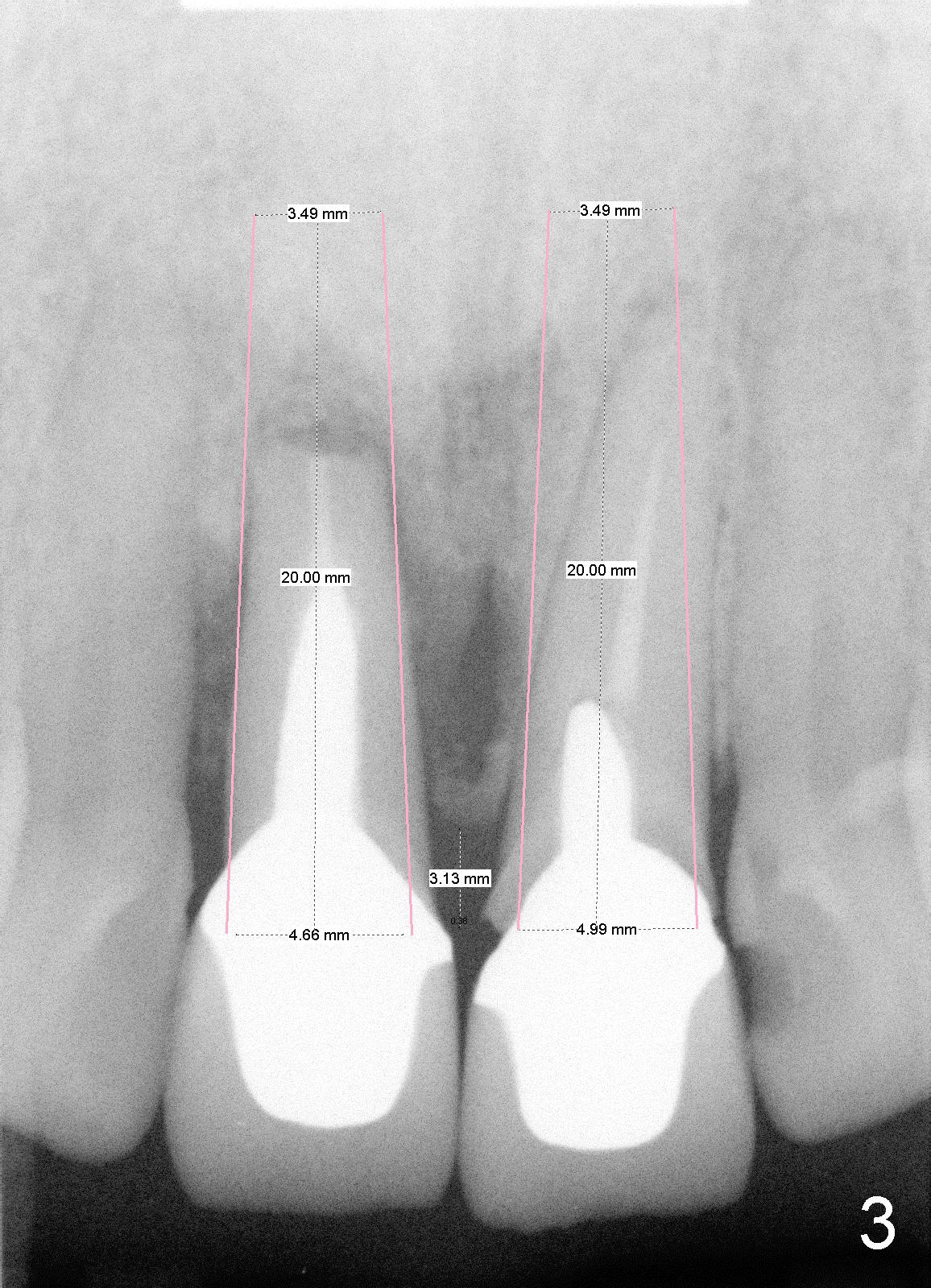
Treatment plan consists of fabrication of temporary crowns (splinting), atraumatic extraction, debridement of sockets (possible labial plate perforation at the site #8), Tetracycline suspension and Chlorhexidine irrigation, osteotomy on palatal wall with drills (Bicon reamers) from 2 mm to 3 or 3.5 mm at slow speed to collect autogenous bone, and placement of 5x20 Tatum tapered implants (Fig.3). Raise flap to expose labial plate perforation, place autogenous bone graft in the defect and around the implants and place collagen membrane for guided bone regeneration. If initial stability of implants is achieved, place 4 mm abutments immediately, reline splinted temporary crowns, and cementation.
Critical comment is welcomed.
Xin Wei, DDS, PhD, MS 1st edition 12/14/2011, last revision 12/14/2011