
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Implant Placed in the Septum
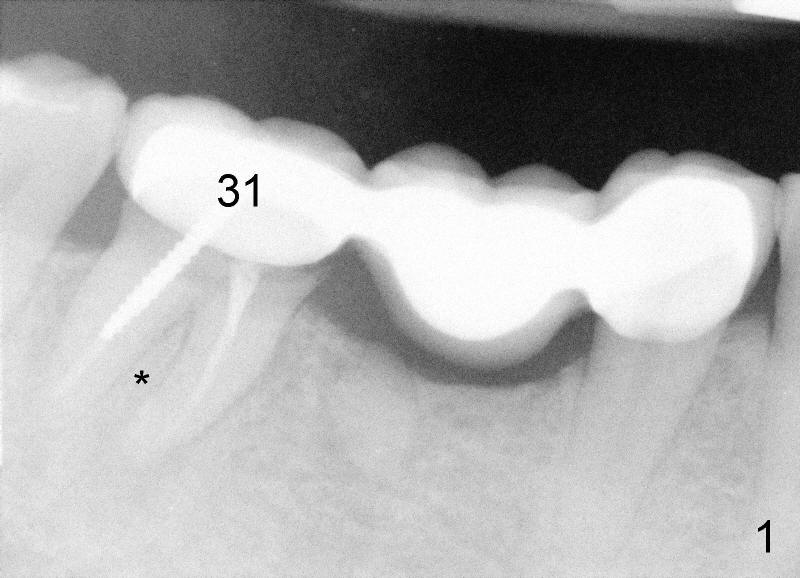
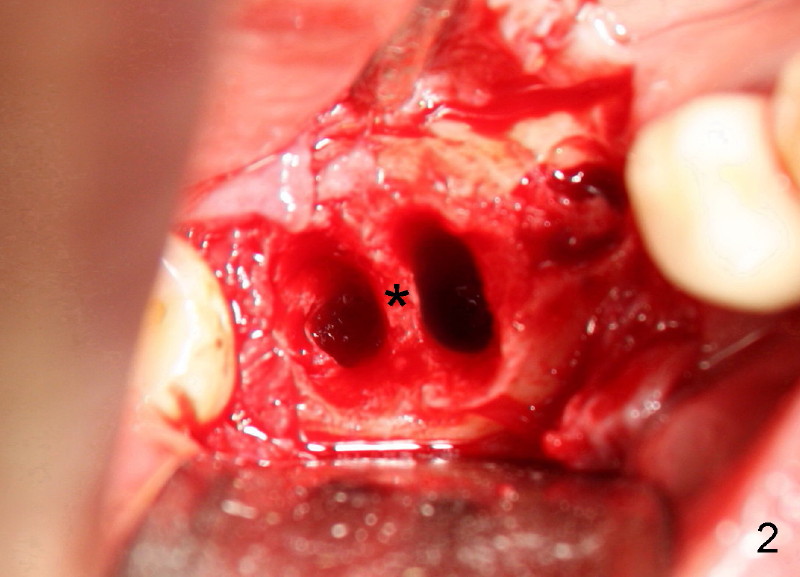
Fifty-three year old man complains that he has difficulty eating in the lower right quadrant. Exam shows that there is 2nd caries underneath #31 retainer and that there is a residual root under #30 pontic (Fig.1). * indicates the septum between the mesial and distal roots of the abutment #31. The teeth #30 and 31 are surgically extracted (Fig.2; *: the septum of #31). A month later, the wound heals (Fig.3).
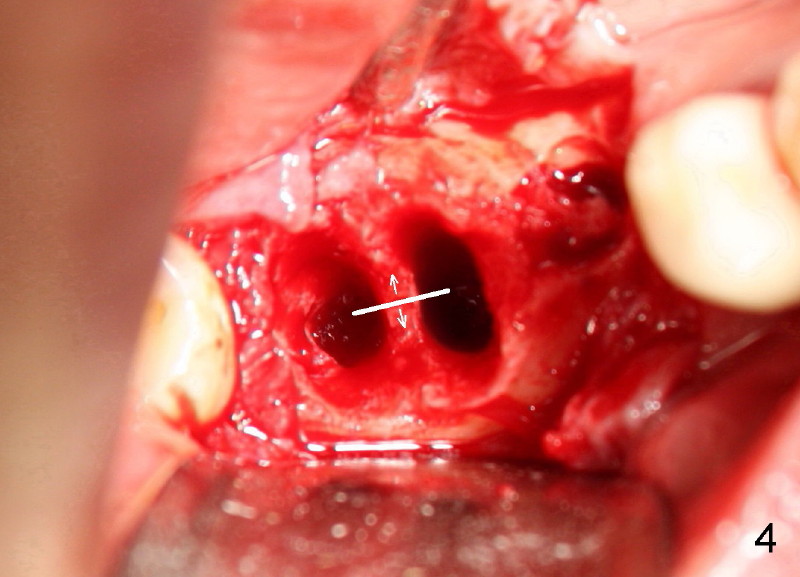
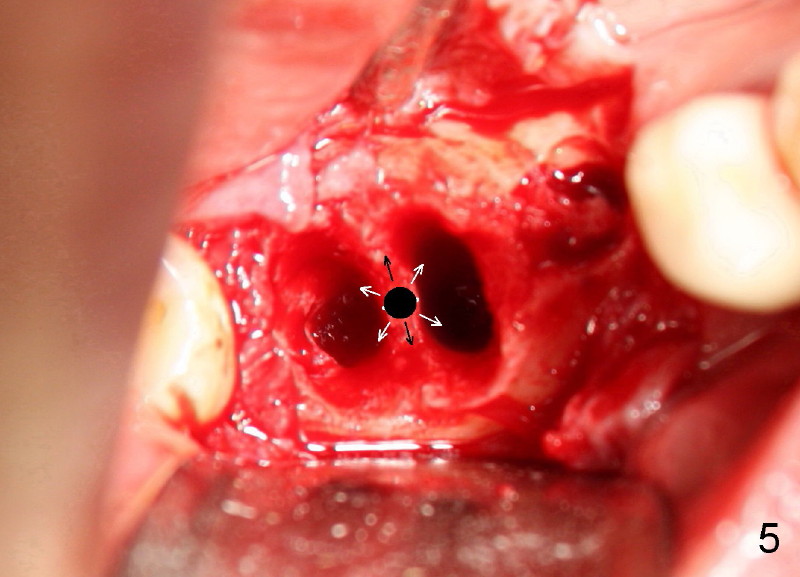
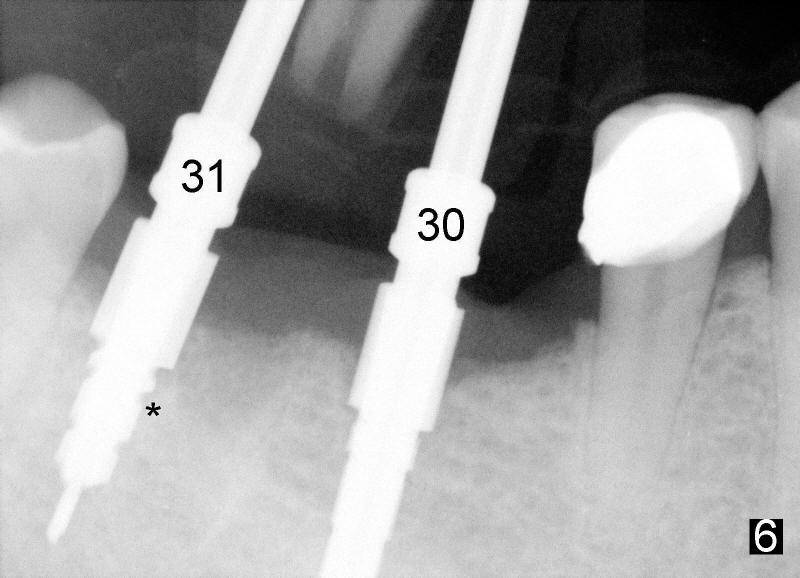
Six weeks post-extraction, a straight incision is made along the crest of #30/31. Without raising flap, #15 surgical blade, bone scalpels (4,5,6 mm wide) and bone blades (4,5.5,7.5 mm wide) ) (Fig.4 white line (illustration); Tatum Surgical) are used to expand the septum buccolingually (arrows). Then round tapered osteotomes (Fig.5 black circle (illustration)) are used to expand the septum circumferentially (arrows). Bone expansion with osteotomes alternates with sequential drills using irrigation. Fig.6 shows 4x17 and 4x14 mm drills placed in sockets #30 and 31, respectively. It appears that osteotomies are placed somewhat distally. The drill #31 is distal to the septum (*).
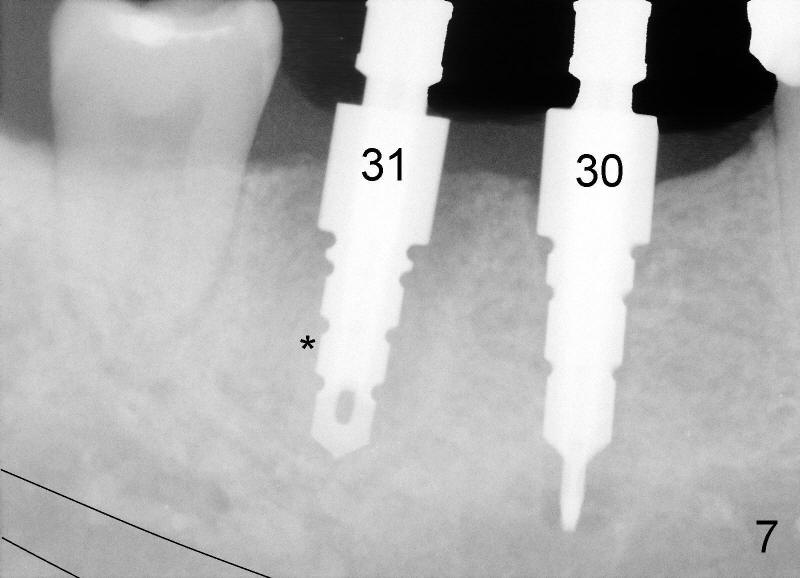
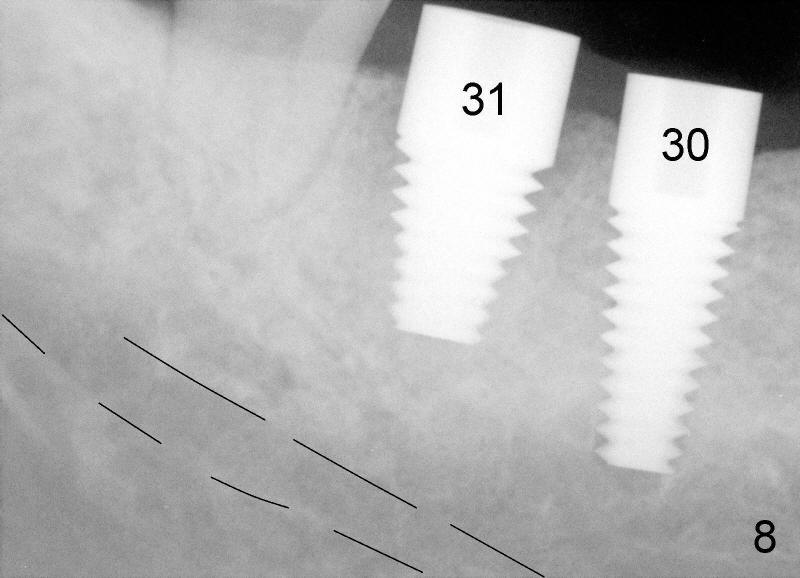
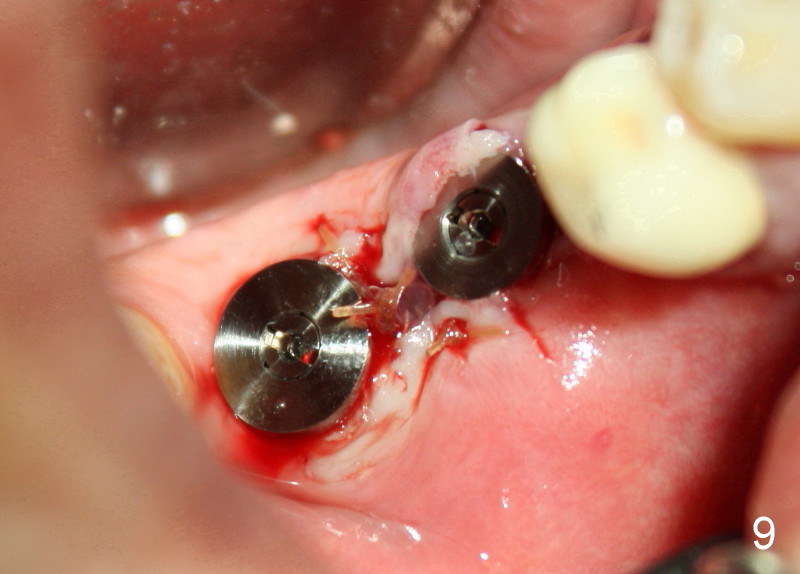
After adjustment, next drills (5x17, and 5x14 mm for #30 and 31) are located more appropriately relative to neighboring teeth (Fig.7) and also in some distance from the inferior alveolar canal (black lines). The septum of #31 is now distal to the drill for #31. Finally 6x17 and 7x14 mm Tatum tapered implants are placed with certain degree of initial stability (Fig.8). Black dashed lines represent the inferior alveolar canal. Fig.9 is taken immediately post-implant placement.
Xin Wei, DDS, PhD, MS 1st edition 11/15/2011, last revision 11/15/2011