
|
|
|
|
|
|
Post-implant Infection
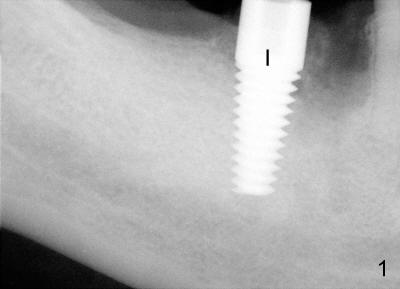
Fourteen days after placement of Tatum tapered implant (6x17 mm) in #30 edentulous area (Fig.1: I), an acute infection develops buccal to supragingivally placed implant (Fig.2: *). Why?
Surgical field was kept as sterile as possible: rinsing with Chlorhexidine, scrubbing oral cavity and perioral skin with Iodine and Ethanol and covering trays and patient's head and chest with sterile towels.
In fact, the inferior alveolar nerve (IAN) was injured during osteotomy. Although the implant was placed without impingement upon the nerve, it was placed supragingivally (Fig.2: I). Medrol dose pack was prescribed. The patient was reluctant to take pain reliever or antibiotic. Mouth rinse was not suggested.
Postop, the patient developed both hyperthesia (pain) and paresthesia for about a week. Oral hygiene was almost abandoned due to pain. When he returned for postop infection treatment, scaling was done with irrigation of hydrogen peroxide between the implant and swollen gingiva before photography (Fig.2). In brief, when IAN injury is suspected intraop, the implant should be placed not only short of injured IAN, but also submerged to reduce contamination. The second point develops after surgery is finished. Postop, pain control and oral hygiene should be maintained.
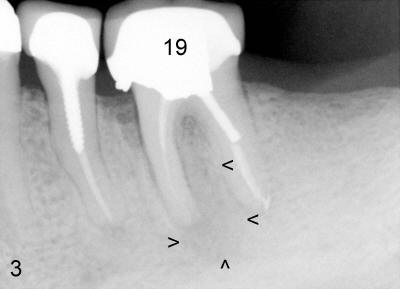
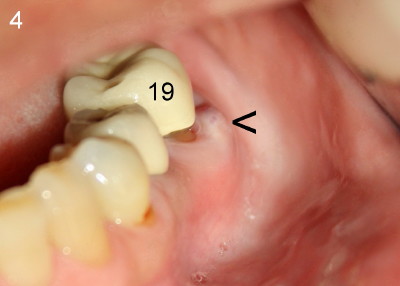
When attention was turned to the left side of this patient, chronic infection was noticed near the buccal furca of the tooth #19 (Fig.4: arrowhead). As a matter of fact, this type of infection has persisted for five years (Fig.3: arrowheads). Extraction of the tooth #19 has not been done because of mild and periodic discomfort. In contrast, signs and symptoms associated with the tooth #30 were more severe and acute, leading to extraction. Ideally, #19 should be extracted prior to or during #30 implant placement to prevent post-implant infection.
Xin Wei, DDS, PhD, MS 1st edition 08/13/2011, last revision 08/21/2011