






|
|
|
|
|
|
|
|
|
|
|
|
|
|
Necessity for Shorter Abutment for Young Patients
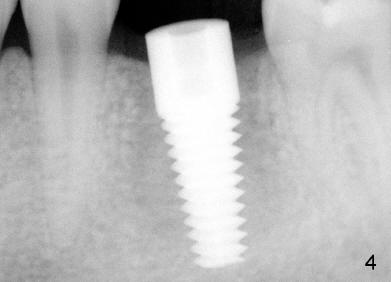
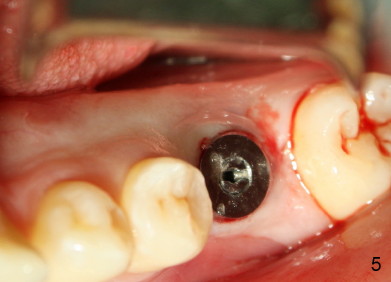
A 22-year-old man requested extraction of the tooth #19 (Fig.1). X-ray was taken 3 and 8 months post extraction, respectively (Fig.2,3). A 6x17 mm Tatum tapered implant was placed (Fig.4,5). A 5 mm (in diameter) 0 degree unipost (5 mm in height) was prepared 7 months after implant placement. Due to limited space, time was spent for extraoral and intraoral reduction of the abutment.
Fig.6 shows Emax crown with limited space for porcelain before cementation. In fact, the crown was fractured during cementation at the area indicated by arrowhead in Fig.6. A new crown was fabricated with core material used in the occlusal portion without porcelain overlay. The new crown was then cemented without complication.
Similar problems are more obvious when two or more restorations are done with limited space using 5 mm uniposts in one appointment. One of the crowns usually needs to be remade later on.
Sometimes large implants are used (7 or 8 mm in diameter). The corresponding large abutments take longer time to trim.
It appears that there is no bone resorption in height for patients at young age. For their implant restoration, a shorter abutment (3 mm long, for example) should be fabricated to save precious clinical time.
I have also shared the images with Dr. Tatum and discussed your concerns. He assured me that while he has used the (9mm) tall abutments for over 40 years, the shorter (5mm) has made the job easier for most clinicians. We did a study amongst our top users and found 85% of them cut the long abutments down to a height between 4.5-5mm. That being said, manufacturing 3mm abutments would just not make sense at this time. Tony
Dear Tony:
Thank you very much for writing the detailed explanation. Fig. 7 shows the die of this case. The margin of the implant (arrowheads) is probably subgingival, as compared to the gingival margin of the neighboring teeth.
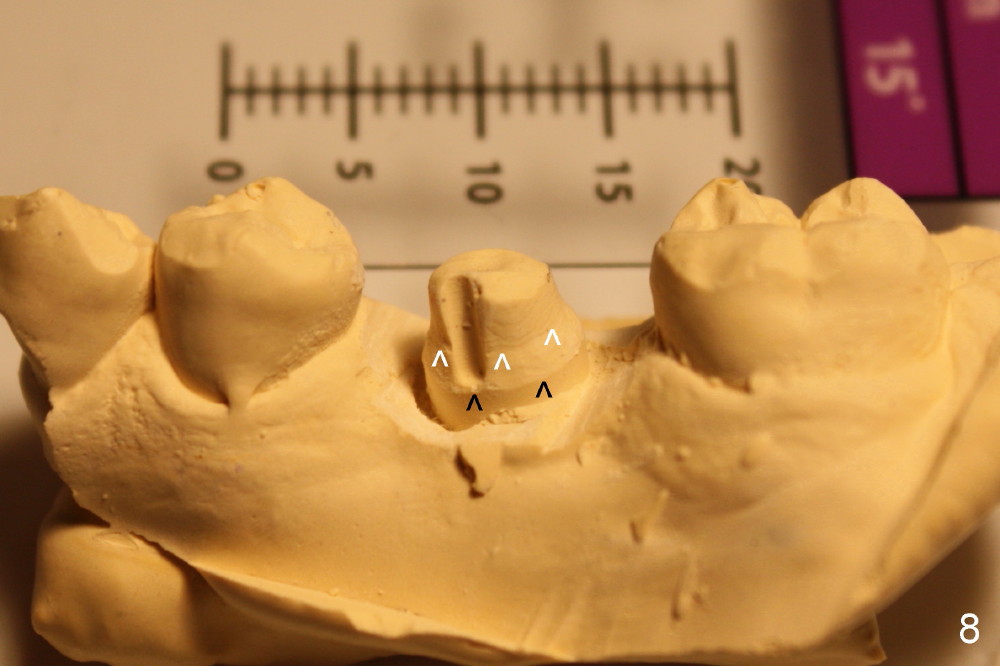
Black arrowheads in Fig.8 (solid cast) point to the implant margin, whereas white ones the junction of the abutment and the implant. The ruler in the background indicates that the height of the abutment is no more than 3 mm.
The buccal plate remains atrophic 7.5 months post cementation (Fig.9, as compared to Fig.5), while there is bone deposit next to the most coronal threads (Fig.10).
The crown was dislodged once and recemented with resin bonding. If it recurs, check whether the abutment is loose and re-prepare the margin and deepen the retentive groove.
Return to Professionals, Thread Patterns
Xin Wei, DDS, PhD, MS 1st edition 05/05/2013, last revision 08/12/2017