


|
|
||
|
|
|
|
|
|
||
|
|
||
Move Lower Molars Mesially
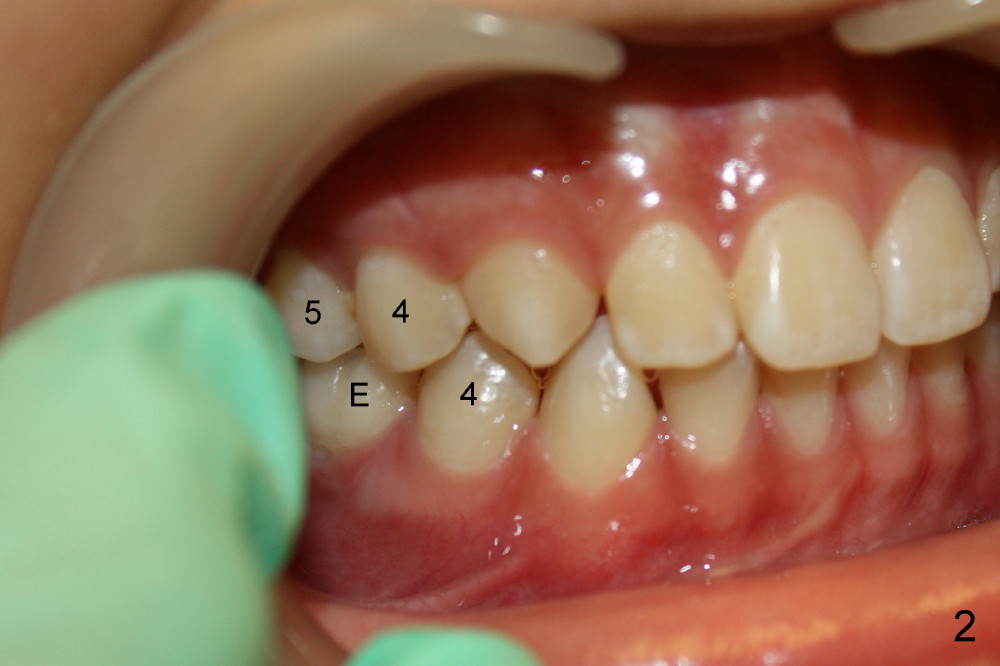
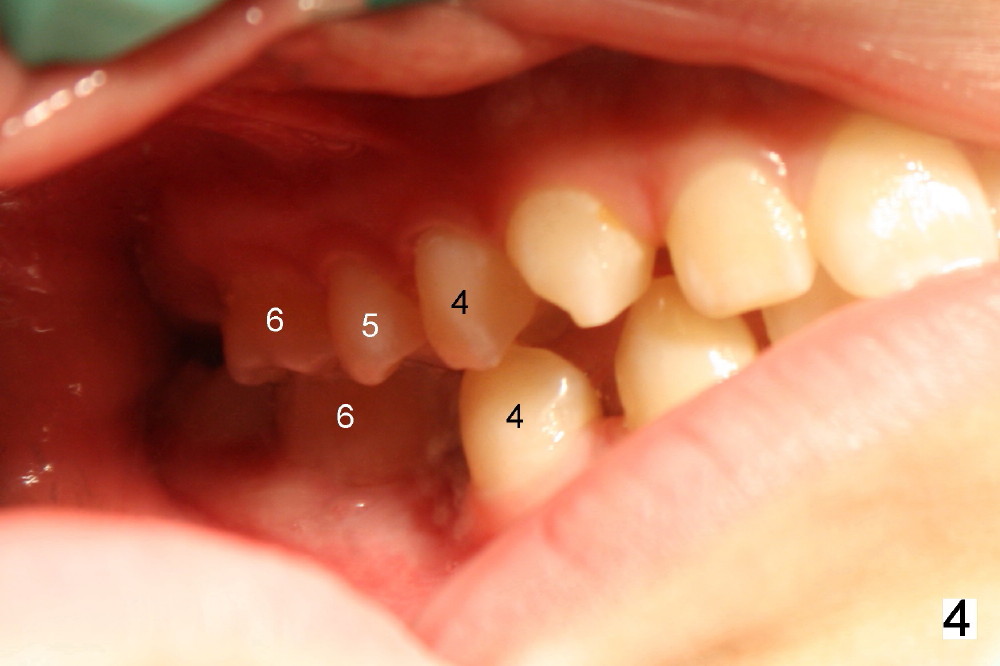
Two lower 2nd bicuspids are congenitally missing in a 11-year-old boy (Fig.1). The lower left (LL) E has been extracted due to caries. There is severe periapical radiolucency associated with the LL6. Root canal therapy (RCT) is being carried out for this molar with difficulty. In addition, the boy is a dental phobic, refusing to have the lower right E extracted in spite of DO caries and pain. In order to reduce the chance of future surgery, including extraction, there are two orthodontic plans to move the lower molars mesially. Fig.2-4 show that the anterior occlusion and right posterior interdigitation is nearly within normal limit, whereas the left is not.
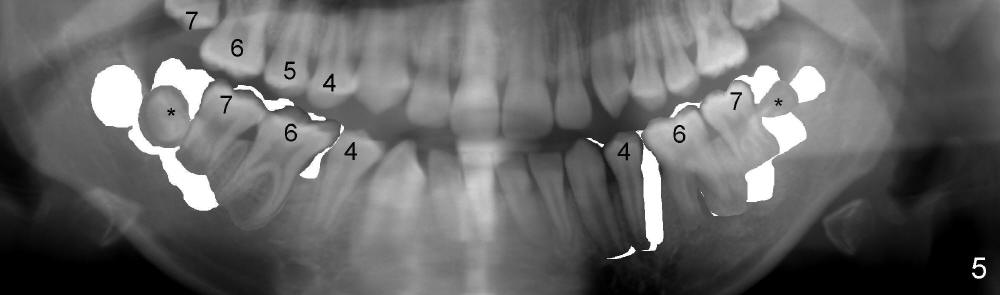
If RCT is successful for the lower left 1st molar, the lower right E is to be extracted. All of the lower molars (including the third molars (Fig.5 *) will be moved mesially so that the final molar occlusion is Class III bilaterally. This is Plan A.
Plan B is shown in Fig.6 when the LL 6 has to be removed due to RCT failure. The orthodontic movement remains the same except LL6. The edentulous space will be kept until the patient turns 18 years old. An implant is placed (black box) and a crown is installed (red outline).
Or is there any better way to fix the problem?
My vote is for implant replacement in the lower. It would be difficult to close space completely in the lower via mesial movement of molars 100%. Of course TADs could be helpful---but a dental phobic??? And if you do not move 100% mesially, you increase OJ and struggle with Class I canine occlusion. If you are successful in moving molars 100%, then your upper second molars become non-functional teeth.Thanks. Pan at the age of 11 shows no U8s, +L8s. My dream is that L8s will occlude U7s. Xin
My dream too! That would be nice---but a long time from now. My other worry is the large radiolucency, moving teeth through this area and hoping like crazy no ramifications.It is also long time to maintain the space. What would you do to prevent U5s from supraeruption into lower E spaces when ortho is done? Xin
That is why I like to close spaces like this in the lower in combination with extraction in the U---if of course it is necessary/defendable. This case does not look like such a case. Patient would need to have significant protrusion in the U. TimExcellent point Xin! Perhaps if U get beyond ext and root canal, with resolution, you could close the spaces---and prevent longer term issue with supra eruption of U second premolars.
Xin Wei, DDS, PhD, MS 1st edition 08/11/2013, last revision 09/10/2013