

|
|
|
|
|
|
|
|
|
|
|
|
Orthodontic Treatment with Extraction of A Lower Canine
Tim: Can you explain a little bit about bite opening in context of the above (to satisfy my curiosity)?
Yes, connecting an AW to the 3s is likely to cause intrusion of 2-2 and bite opening---at least temporarily.
Hi Xin,It is a brilliant idea. Is it inherited from ortho department of UNC or you have refined and developed it? I will publish this case on my web so that I will never forget this idea.
I have published Toby's case. While I was editing, two questions popped out. First, asymmetric extraction may make it hard for you to achieve interdigitation bilaterally. Your experience indicates that this is not a problem? Second, LL3 root may elongate once the tooth is erupting fully.
Interdigitation in the posterior will be hard to achieve. Primary goal in Toby is to resolve crowding and with short roots, be realistic. A functional posterior occlusion is the goal. Something must be removed from the bottom and I am choosing to substitute the LL4 for a LL3:-) And you are right, the LL3 is a bit longer than it appears on the pan because of imaging.
Tim: thank you for all the replies and explanation. Your treatment plan will be carried out faithfully if there is no particular situation.
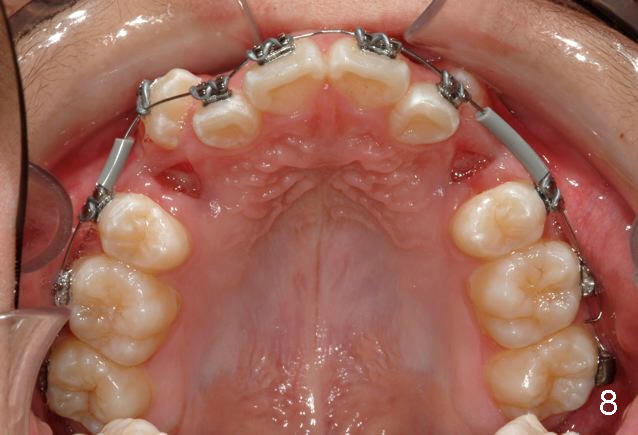
P.S. I do not take the first small gauge NiTi AW back to the 7s at appointment #1, to A) make sure of a good 7 bond (as they are most difficult to isolate), B) to prevent a wire poke if a 7 should come off, and C) minimize the chance of a very flexible AW pulling out of the 7. If the 7s are still bonded at appointment #2, I trust I have a good bond and then include the 7 with every subsequent AW change. I thought I would share that little tip with you:-)
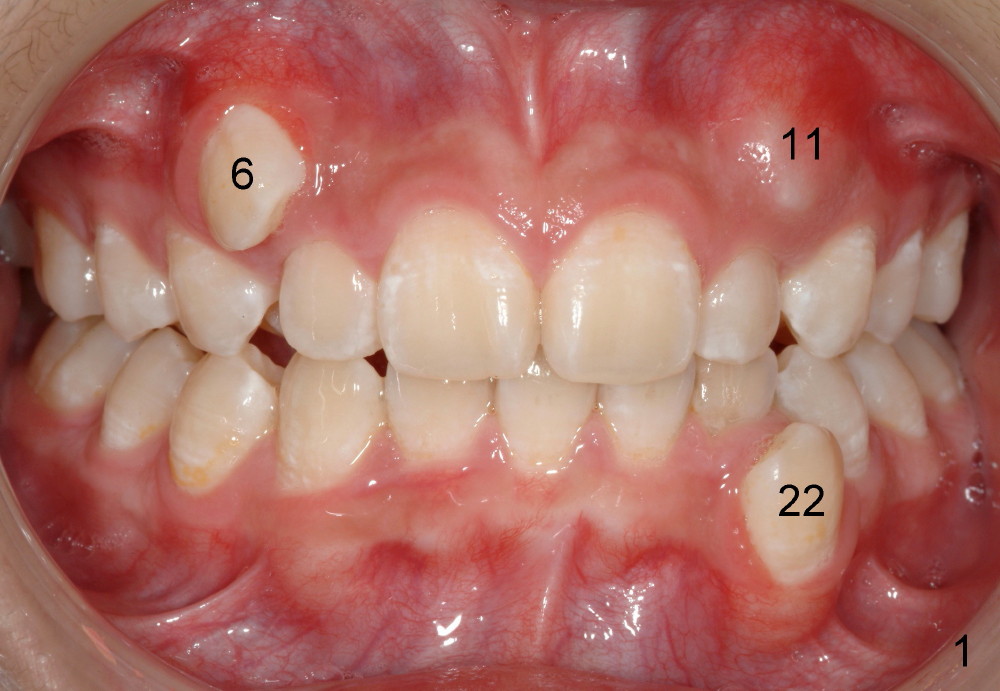
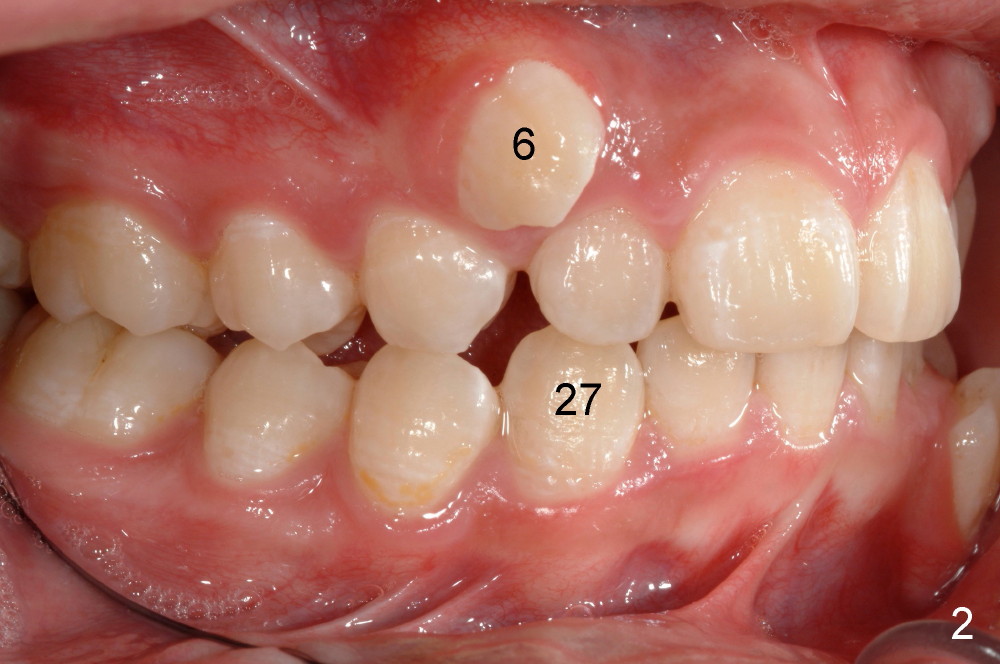
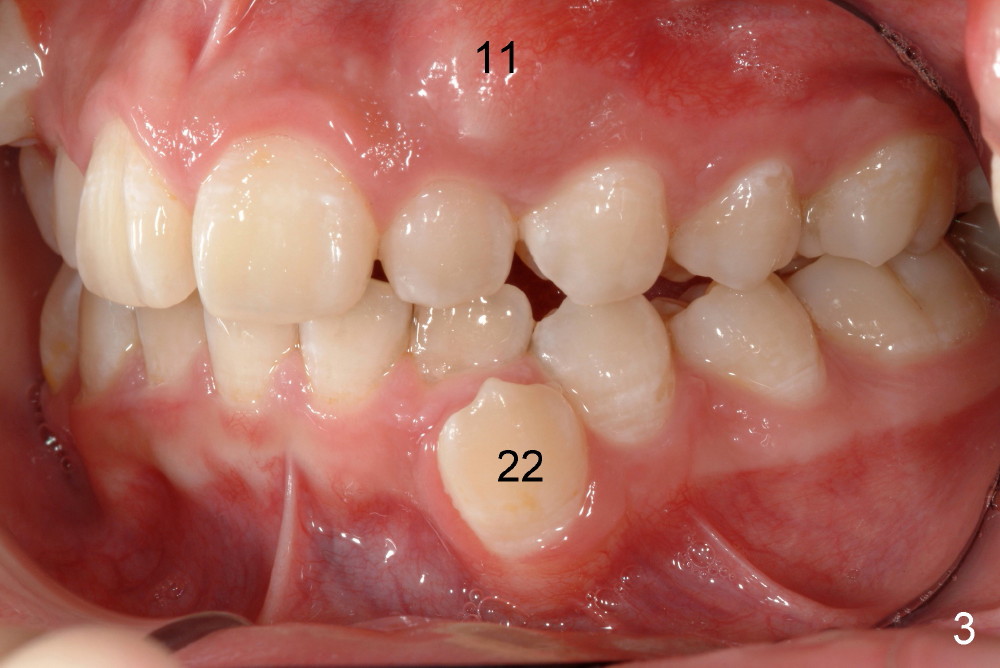
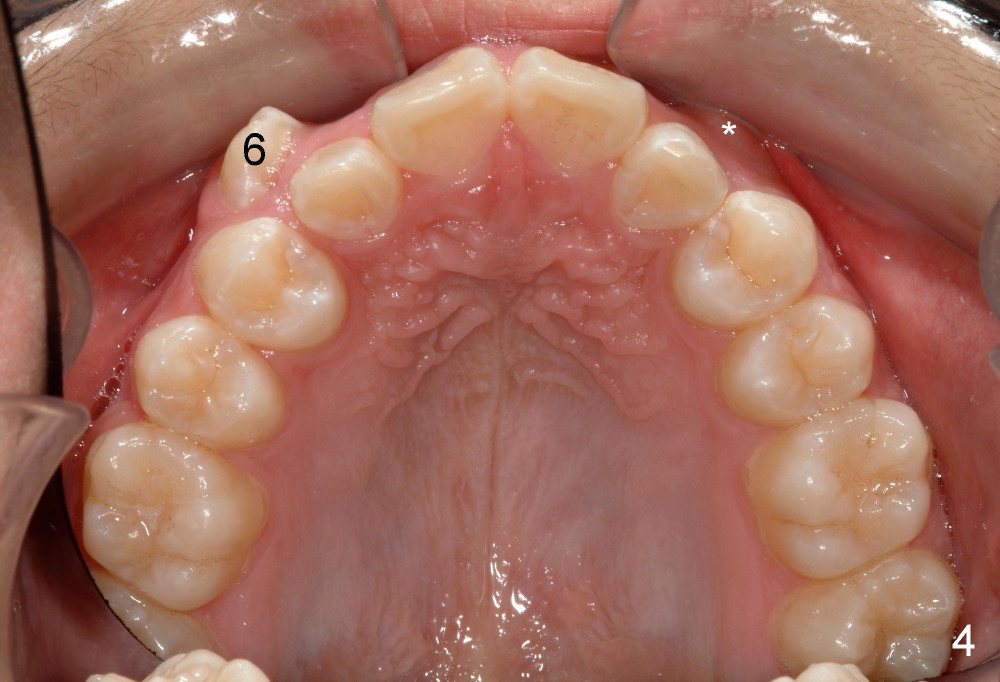
Tim: Thank you so much for the tip. It appears that an alastik is placed between #6 bracket and the upper AW. Can you recommend surgical exposure of #11?
I love the term teasing and your concept of minimizing reciprocal forces. When the opposing arch is used as anchorage, the reciprocal forces are basically totally avoided. The opposing arch has more mature periodontium/bone and several teeth as a group. In my case, surgical exposure was considered for #6, because of extraction of the retained deciduous canine. It was possible to place a lingual button for #11 for initial retraction. Later it has to be removed. A bracket is to be placed in a normal position. Treatment will be delayed. In fact, the young girl is doing great after surgery on both sides, the same way Toby does.
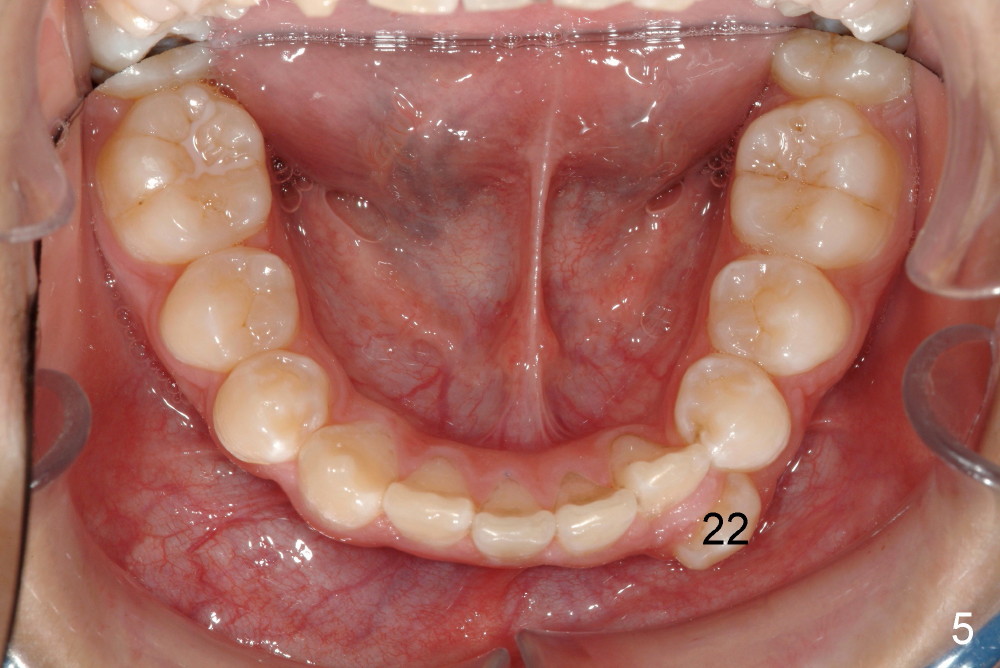
I hated to extract his lower left canine, more due to expected difficulty. Amazingly, the patient was more ready for extraction than me. He said that the tooth was not of use at all. He has been under my care periodically for a while. Her mom did not want to have treatment for his deciduous teeth. Besides, he is my daughter's classmate.
In fact, the canine was easier to be extracted than the two upper first bicuspids. It had been nonfunctional, out of occlusion. The periodontal ligament must be loose and alveolar bone is immature. The buccal bony plate is thin and low. Toby returned for cleaning 3 days post extraction. The three sockets healed so well that photos were taken. Unfortunately the latter are misplaced. Otherwise we would share them with you.
Anyway, we may need to discuss some of issues more often and in advance so that the service may be rendered in a more efficient manner. That is why I update another case for you. He is your next potential patient. Check my previous message. Thanks. Have a nice weekend, too. As a matter of fact, I am in Las Vegas for an implant training.
Xin Wei, DDS, PhD, MS 1st edition 11/05/2013, last revision 12/07/2013