











|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
Retreat or Surgery?
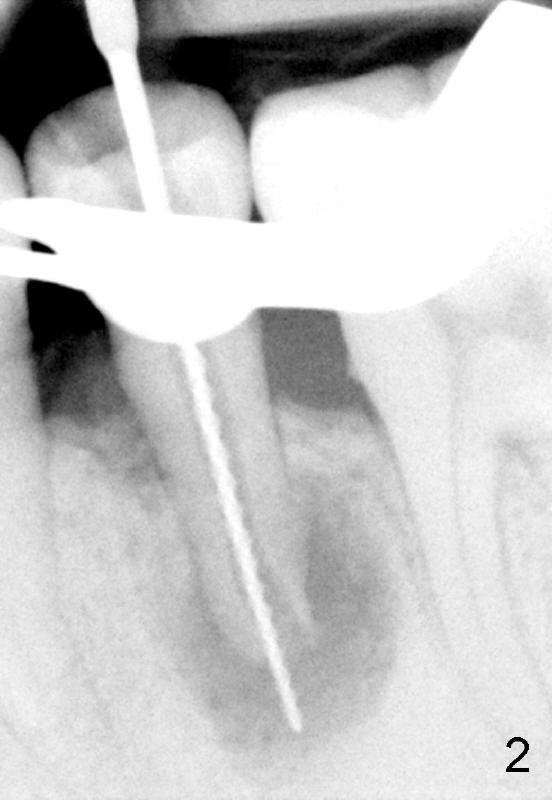
A 40-year-old Chinese man has periodic (once a month) mild pain and swelling in the lower left quadrant. Clinical exam reveals dens evaginatus (Fgi.1': <) in #20. Upon pressure from mouth mirror handle, there is limited amount of purulent discharge from the fistula (Fig.1": <). Preop PA shows a large canal with large periapical radiolucency (Fig.1). RCT started on Aug 6, 2010 with #70 file at 20 mm (Fig.2), #120 file at 16 mm (Fig.3) and CaOH paste in the canal (Fig.4). The dressing changed on Oct 8, 2010 (Fig.5). RCT finished on Jan 25, 2011 with master cone (rolled with several gutta perchae) (Fig.6), lateral condensation (Fig.7) and after vertical condensation and build-up (Fig.8). The canal was wet in the last two appointments with no sign of apexification. Follow up is done in 7 months (Fig.9), 11 months (Fig.10) and 18 months. Although the patient reports no pain after the treatment, the fistula remains with purulent discharge. The patient does not accept apical surgery. What should we do? Retreat with MTA (1,2,3)?
魏心:
1. 首先证实无折裂发生。
2.以Ca(OH)2 dressing
数天至数周直到干燥环境已确立,因为有炎症渗出或有症状。然后再放MTA Plug,以获取良好的封闭。
3.MTA Plug 后一天,完成obturation和修复。
我认为单纯以Ca(OH)2等待apical barrier 是不可靠的,对于这一病例。
方炳忠
Xin Wei, DDS, PhD, MS 1st edition 08/07/2012, last revision
08/13/2012