


|
|
|
|
|
|
Cause of Perio-Endo Disease
A 60-year-old man has a history of periodontitis with perio surgery for several decades. He develops sudden episode of apparently acute apical periodontitis of the upper 1st molar. There is deep pocket in buccal furcal area. The acute infection is controlled by incision & drainage (I & D). Buccal plate is found to have been lost during I & D. It is assumed that the apical periodontitis is due to infection from deep perio pocket.
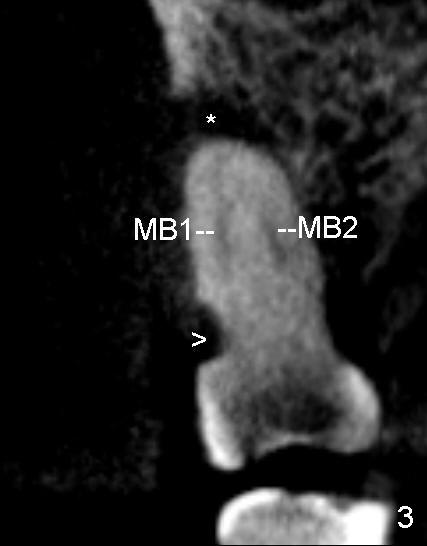
Due to complexity of the case, CBCT is done. The buccal plate is found to be lost completely over the mesiobuccal root (Fig.3), but partially over the distobuccal one (Fig.4 >). There is a deep cervical defect associated with MB root (Fig.3 >), whereas the defect is minimal over the DB root. More surprising is that periapical radiolucency is larger associated with MB1 (Fig.*) than any of the other canals (Fig.4 *) (including MB2, Fig.3). The Class V defect is close to MB1 (Fig.3). It appears that apical periodontitis is induced by Class V defect over the MB1 canal.
During root canal therapy (RCT), the pulp is found to be necrotic for MB1, DB and P canals and vital for MB2, which is obliterated in the coronal portion of the canal.
Most surprising is that the buccal aspect of the 1st molar looks normal after dissolution of apical infection (Fig.1). The cervical defect is revealed after insertion of gingival retraction cord (Fig.2 >). Composite restoration for the cervical defect is done prior to RCT.
This case demonstrates cervical defect to be the hidden cause of perio-endo disease.
Xin Wei, DDS, PhD, MS 1st edition 07/06/2012, last revision 07/06/2012