
|
|
|
|
|
|
|
|
Why does this Premolar Become Reinfected after RCT (Main Text)?
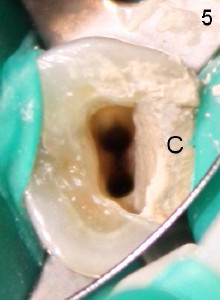
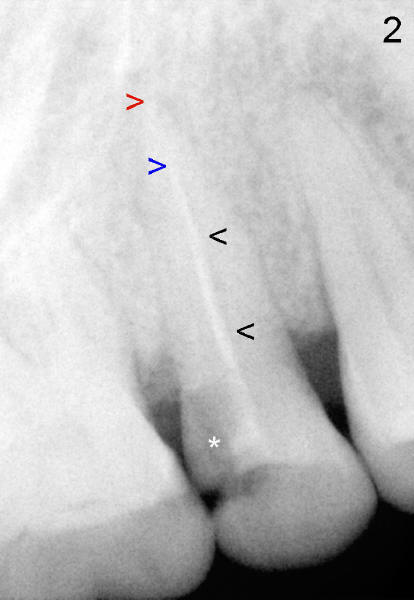
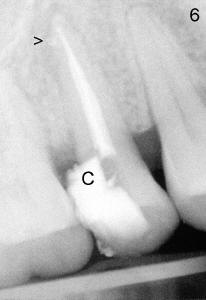
After removing DO caries and enlarging the access, it becomes obvious that there is a missing buccal canal (Fig.3 B). There is purulent discharge from the buccal canal in the beginning of the debridement. Fig.3 photo is taken after the buccal canal is fully shaped with rotary files (final file: 30/.06). Arrowhead points to the original lingual orifice with gutta percha. The RCT retreat is initiated on emergency basis. There is not enough time to remove the lingual gutta percha. More importantly, there is leakage of sodium hypochorite during irrigation due to large DO defect. After drying the buccal canal, the access is sealed with cotton pellet and Cavit. In fact the symptom and signs of reinfection disappear after initiation of RCT retreat. In the 2nd appointment, the occlusal portion of the Cavit is removed for accessing, leaving distal portion in place. The lingual gutta percha is removed and the lingual canal is re-shaped. Fig. 4 shows two master cones (30/.06). The buccal and lingual canals fuse at the apex. Fig.5 photo is taken after the two canals are dried. C stands for the remaining distal portion of the Cavit. There is no leakage during NaHOCl irrigation. Fig.6 shows the final obturation with with possible lateral canal filling (arrowhead). The access is again re-sealed with Cavit (C). Nine days later, the patient returns for prefabricated post and PFM preparation. Finally PFM is cemented. The patient remains asymptomatic.
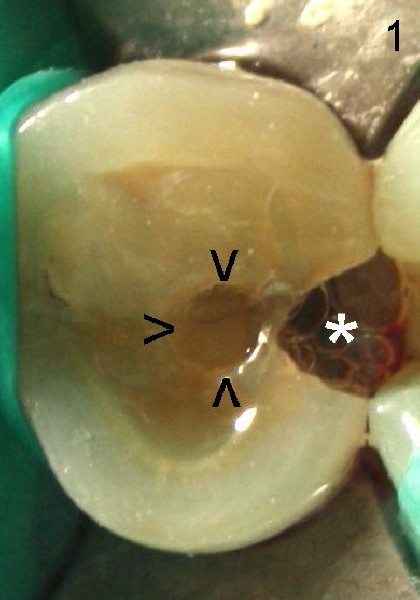
It is apparent that a missing canal is the main reason for the reinfection. The originally limited access (Fig.1 arrowheads) is the reason for the failure to find the missing canal.
Xin Wei, DDS, PhD, MS 1st edition 07/15/2011, last revision 07/16/2011