




|
|
|
|
|
|
|
|
|
|
|
|
|
||
Root Fracture Prior to RCT?
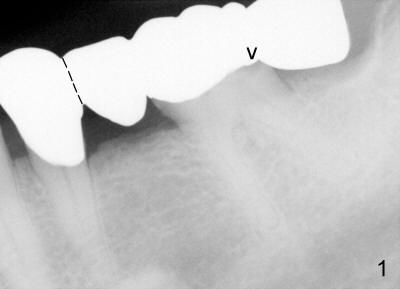
A 60-year-old man presented to clinic 2 years ago with chief complaint "bottom left bridge is loose". Dental history revealed that some of his missing teeth is due to RCT failure. Exam showed that #30 and 31 were missing. There is a 4-unit cantilever fixed partial denture (FPD) involving #18 to 21 (Fig.1); the distal margin of #19 was open (arrowhead) . Clinically, the gingiva between #18 and 19 was erythematous and edematous. The tooth #19 had mild percussion. Higher magnification of #19 showed increased periodontal ligament in the mesial and distal apices (red arrowheads in Fig.2). After sectioning between #20 and 21 pontic/retainer, as shown by dashed line in Fig.1, the distal portion of FPD came off by itself. The DOL caries under #19 retainer was confirmed. The pulp was not exposed after carious removal. Pulpal test appears to show that the tooth was vital. Temporary restoration was placed. The patient returned to clinic for #19 RCT due to tooth sensitivity 4 months later.
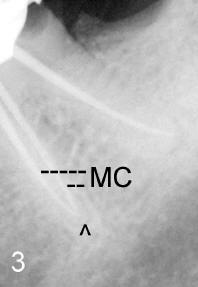
In fact, the tooth was necrotic and canals were sclerotic. Apex locator was used for working length. PA in Fig.3 was taken after placement of tapered master cones. The tips of master cones in the mesial root (MC) were ~.5 mm from apex (arrowhead). Cold lateral condensation was done for the distal canal (with one medium accessory gutta percha), but not for the mesial canals. Overfilled paste associated with the mesial canal (Fig.4 arrowhead) is not only larger than that in the distal canal, but also is apparently not continuous with the mesial apex.
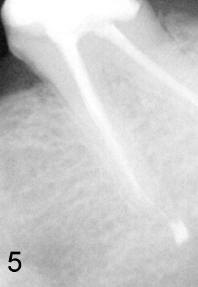
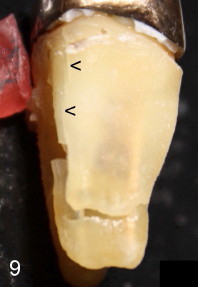
Fifteen months since RCT, the symptom (mild tenderness to mastication) has not improved. Routine X-ray does not show any deterioration (Fig.5). A single-unit crown was placed for #19. Since multiple implants were planned, CBCT was taken. The latter shows bone loss involves the mesial root (Fig.6,8): mesially (arrowhead), lingually (L) and apically (*, A). Fig.8 is a section view through the mesial canals. At an appointment of implant placement for #30, infection of #19 was found. The tooth was extracted. Fracture of the mesial root was confirmed (Fig.7,9). Arrowheads in Fig.9 point to a crack line.
It appears that the patient is a bruxer. Multiple missing teeth makes the tooth #19 sustain heavy mastication. It increases the chance of root fracture. It is felt that the fracture may happen prior to RCT. It seems that working length was well controlled Fig.3,6,8), but the overfilled paste from the mesial canal was out of control (Fig.4). Prior root fracture makes the latter possible.
Root fracture is difficult to diagnose, particularly for a bruxer. The bone density proves to be high when osteotomy was made for #30 implant placement, type I. The high density of bone makes it difficult to detect periradicular lesion around crack/fracture lines with traditional X-ray.
Xin Wei, DDS, PhD, MS 1st edition 08/14/2011, last revision 08/14/2011