



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
How to Handle Missing Canal?
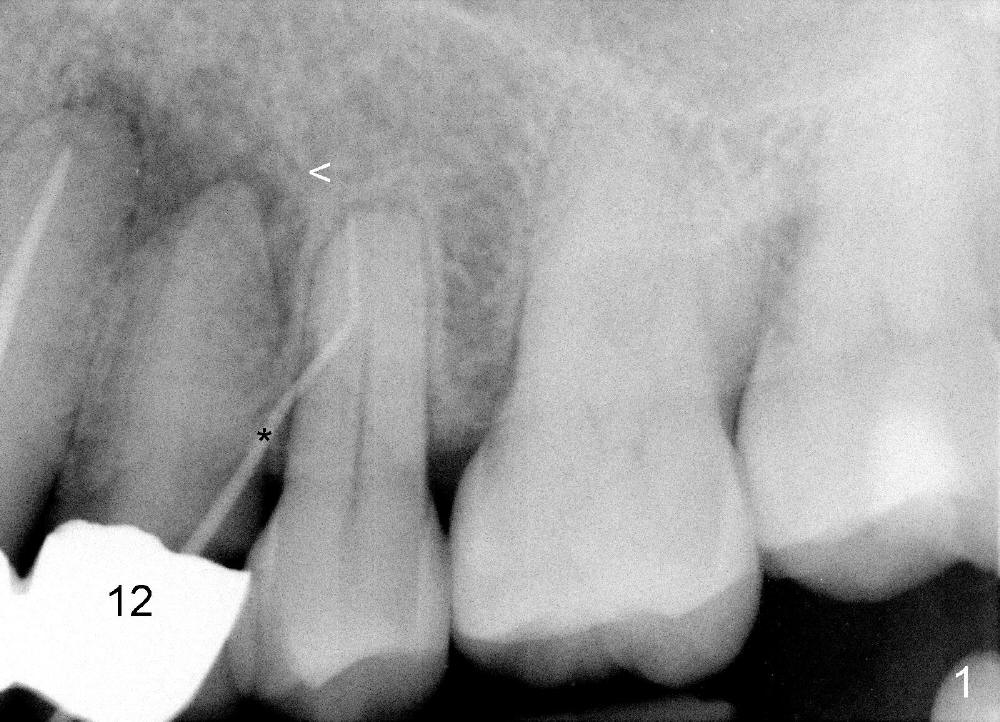
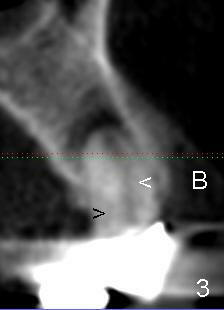
A 74-year-old man has an apical fistula (*: Gutta Percha inserted into the fistula) associated with periapical radiolucency of the tooth #12 (Fig.1 <). The first appointment fails to find the lingual canal, in spite of the fact that there are apparent two canals shown by a preop PA (Fig.2 <). Calcium Hydroxide paste is placed in the debrided buccal canal. Review of previous CT image shows the patent buccal canal (Fig.3 white <) and the apparently obliterated lingual canal (black >).
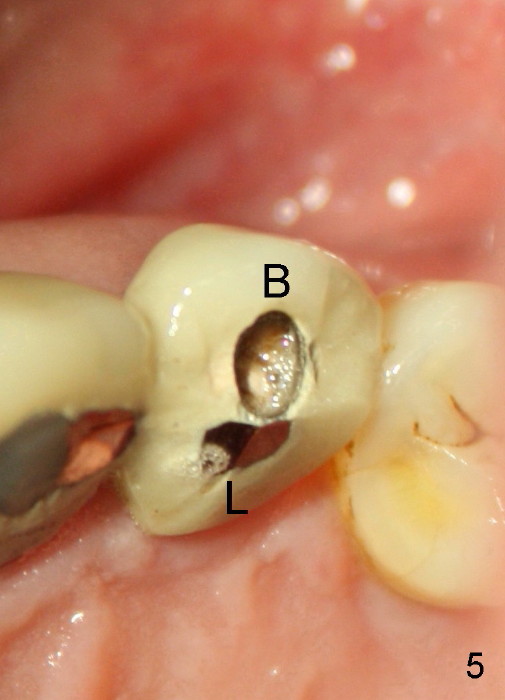
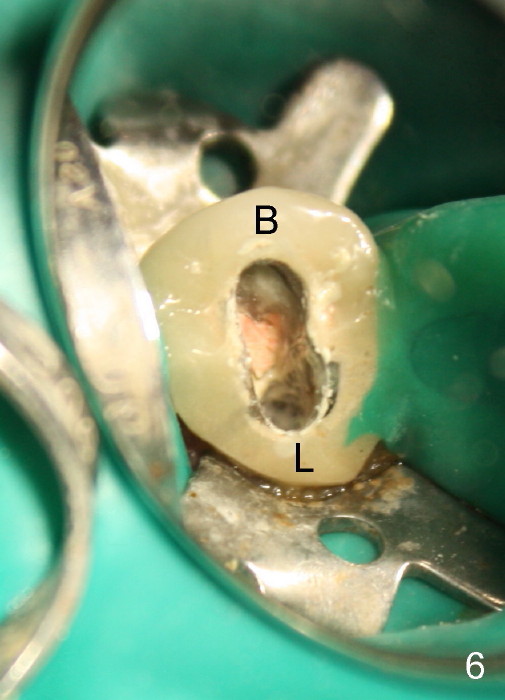
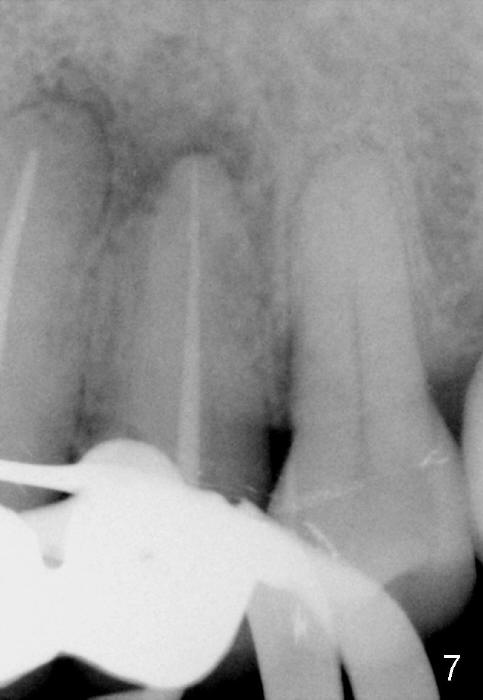
One month later, the fistula is regressing, while the pain reduces (Fig.4). It appears that the initial access is not extended lingually enough (Fig.5). The lingual canal is still non-negotiable when the access is enlarged (Fig.6). Working length of the buccal canal is confirmed with 30/.06 Gutta Percha in place (Fig.7). After explanation and consent, RCT is finished routinely. Two months postop, the buccal apical fistula resolves with no symptom (Fig.8). The retainer at the site of #12 is not removed to increase chance of finding the missing canal. It is part of a long bridge.
Seven months post RCT, the patient remains asymptomatic without relapse of the fistula; the periapical radiolucency apparently decreases (Fig.9). The long bridge dislodges 4 years later. The tooth #12 is extracted.
Return to
Professionals
Xin Wei, DDS, PhD, MS 1st edition 11/23/2014, last revision 09/15/2019