


|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sinus Lift Using Bone Expander Kit (ITL)
Bone expander technique is more acceptable to the patient than osteotomes. The former takes longer time to do. Both are indicated in cases of poor bone density and width.
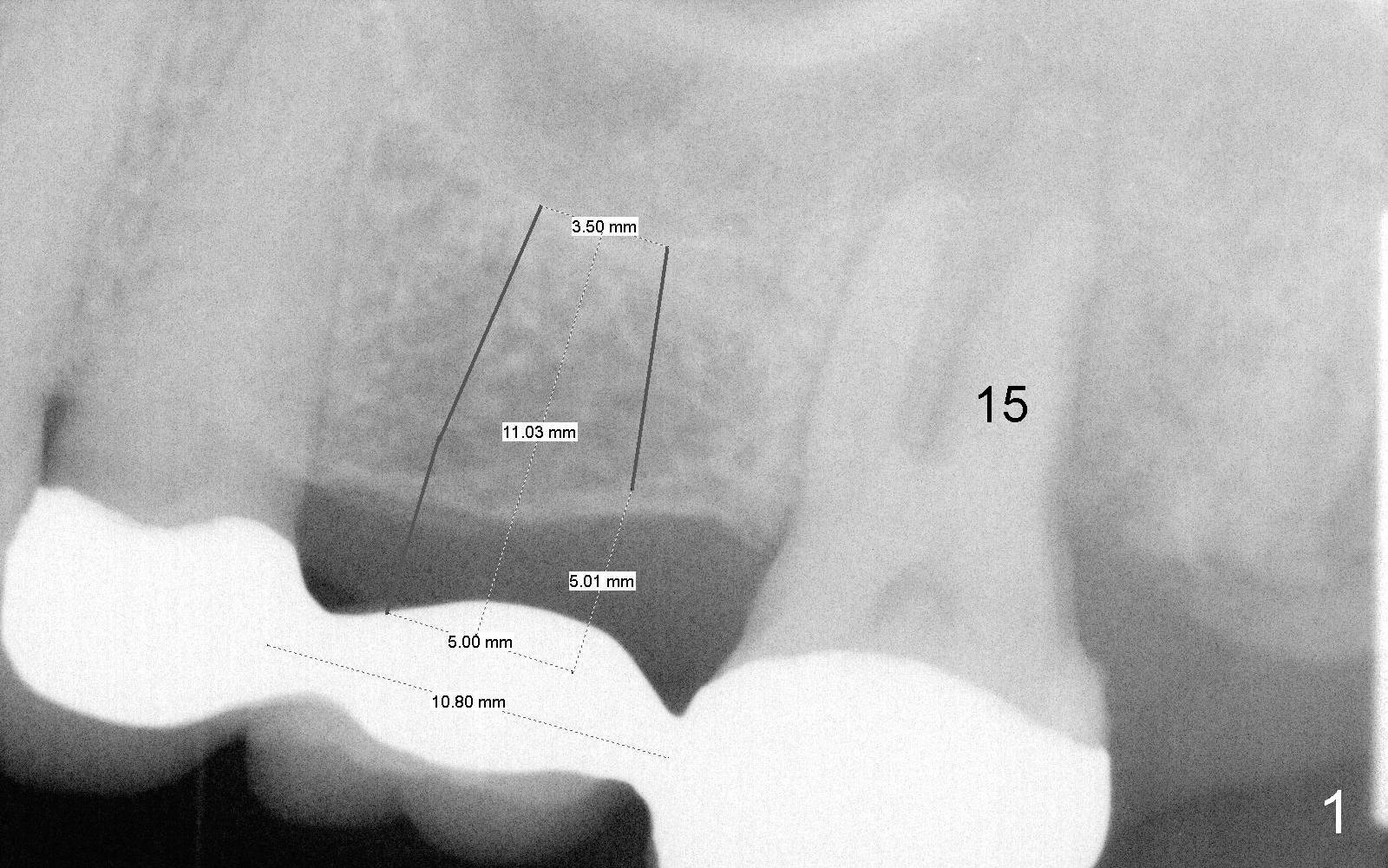
A 65-year-old lady has a failing FPD in the upper left quadrant (Fig.1). After the posterior abutment (#15) is extracted, an implant is planned at the site of #14 (5x11 mm). The bone width and density are expected to be low, considering the long term loss of the tooth.
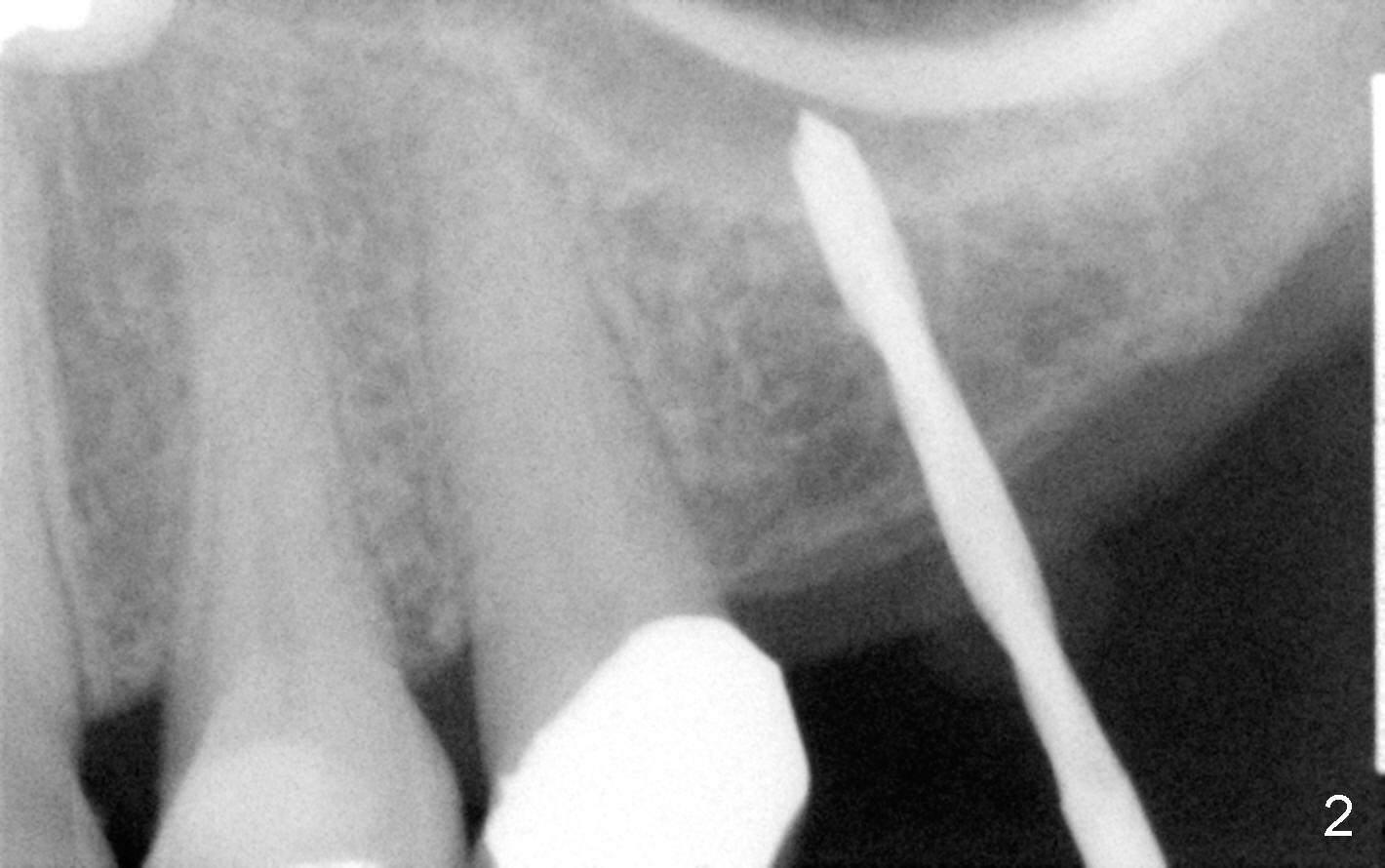
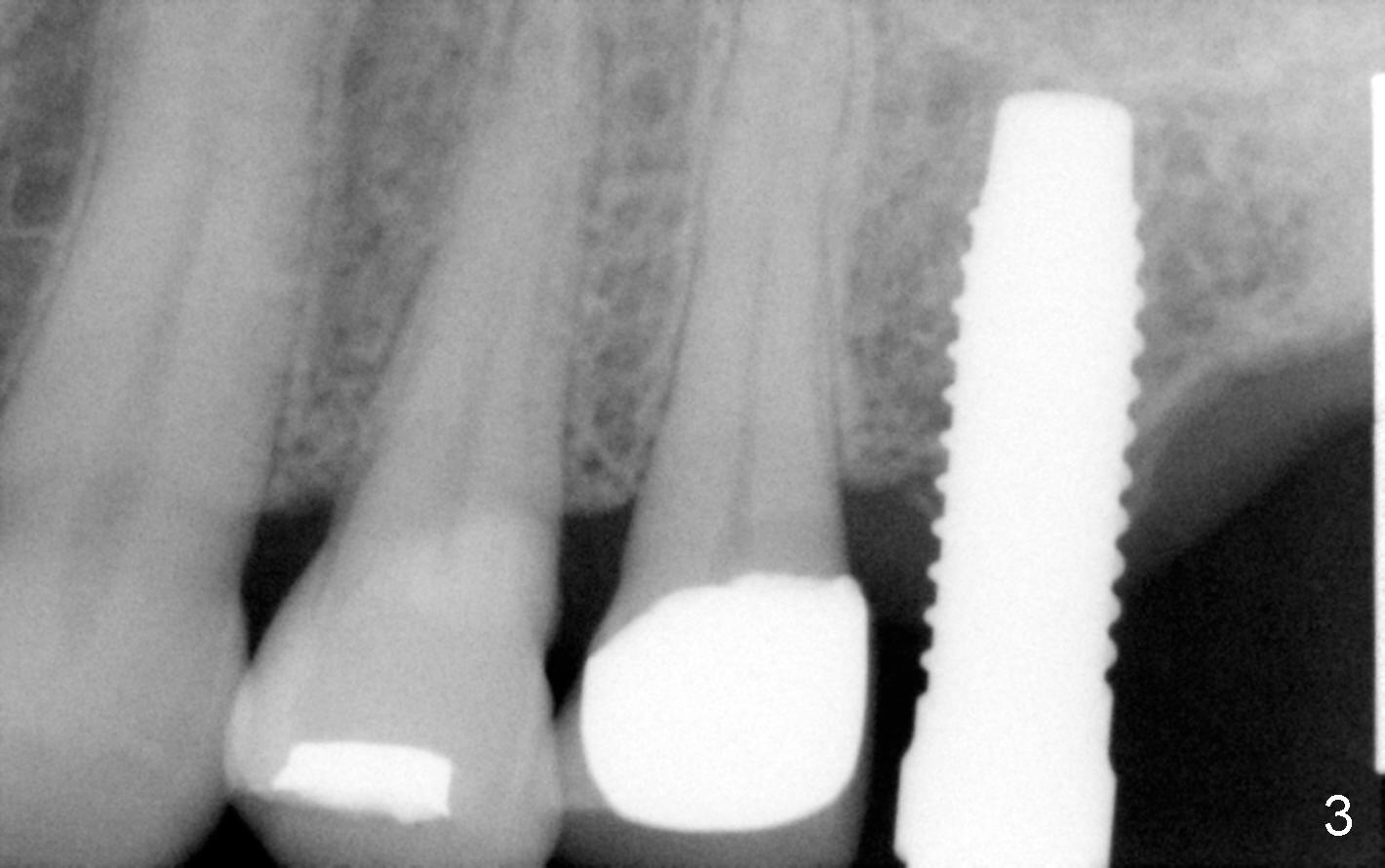
Fig.2 shows a 1.6 mm pilot drill at the depth of 11 mm; the tip of the drill penetrates the sinus floor. Bone expanders (2.6, 3.0, 3.4, 3.8 (Fig.3) and 4.3 mm) are used and alternated with tapered osteotomes (3 and 4 mm). The latter are used to break through the sinus floor. Then 4.5x14 mm and 5x14 mm taps are applied to create threads for implant. The second tap has some binding to the bone. Finally 5x14 mm tapered implant is inserted with more than 60 Ncm torque (Fig.4). Although the apical portion of implant (approximately 3 mm) pokes into the sinus, the patient does not experience nasal hemorrhage intra- or post-op.
The patient develops herpetic infection on the left corner of the mouth and in the palate corresponding to the teeth #13 and 14. The infection disappears 7 days after antiviral mouth rinse and ointment.
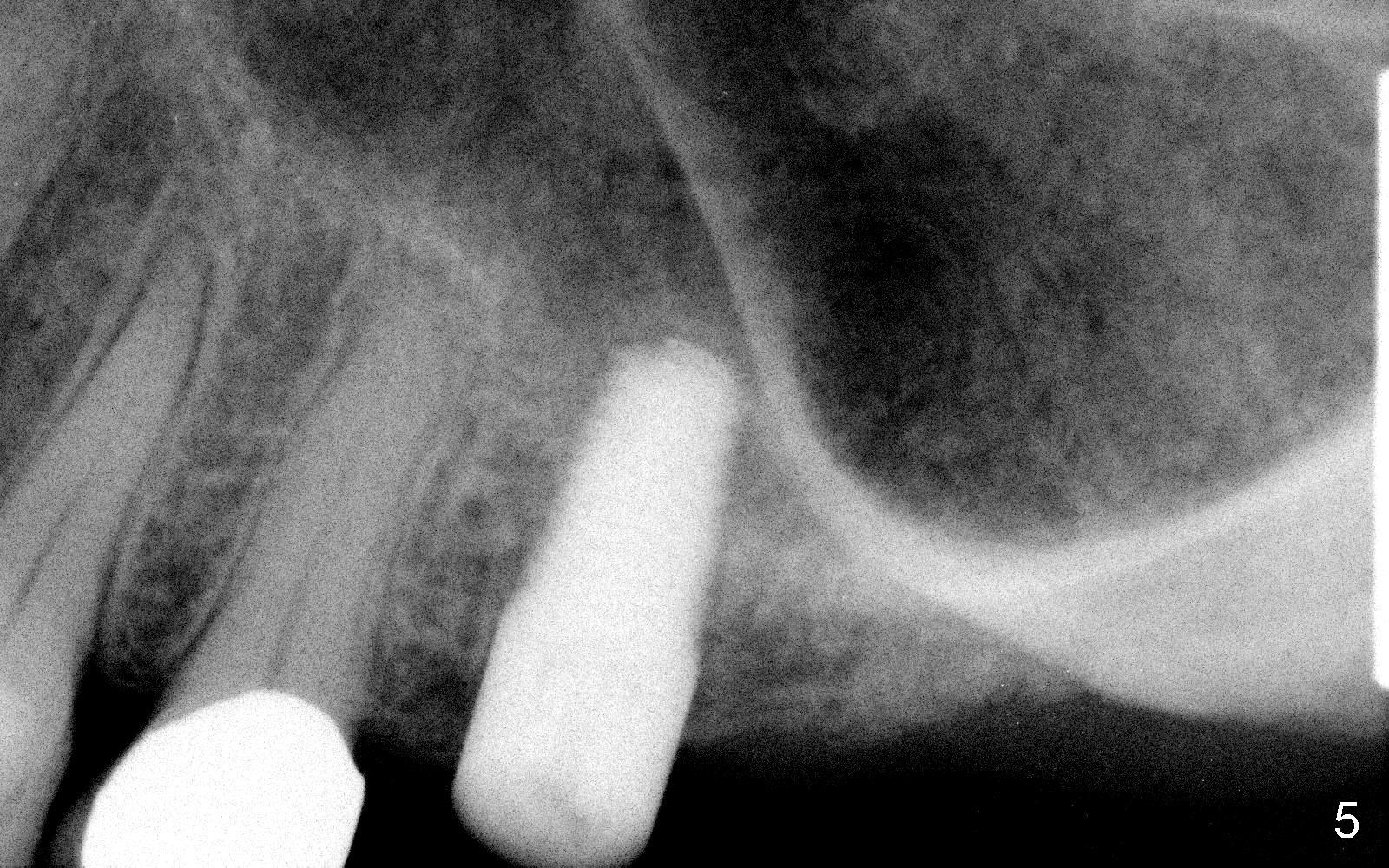
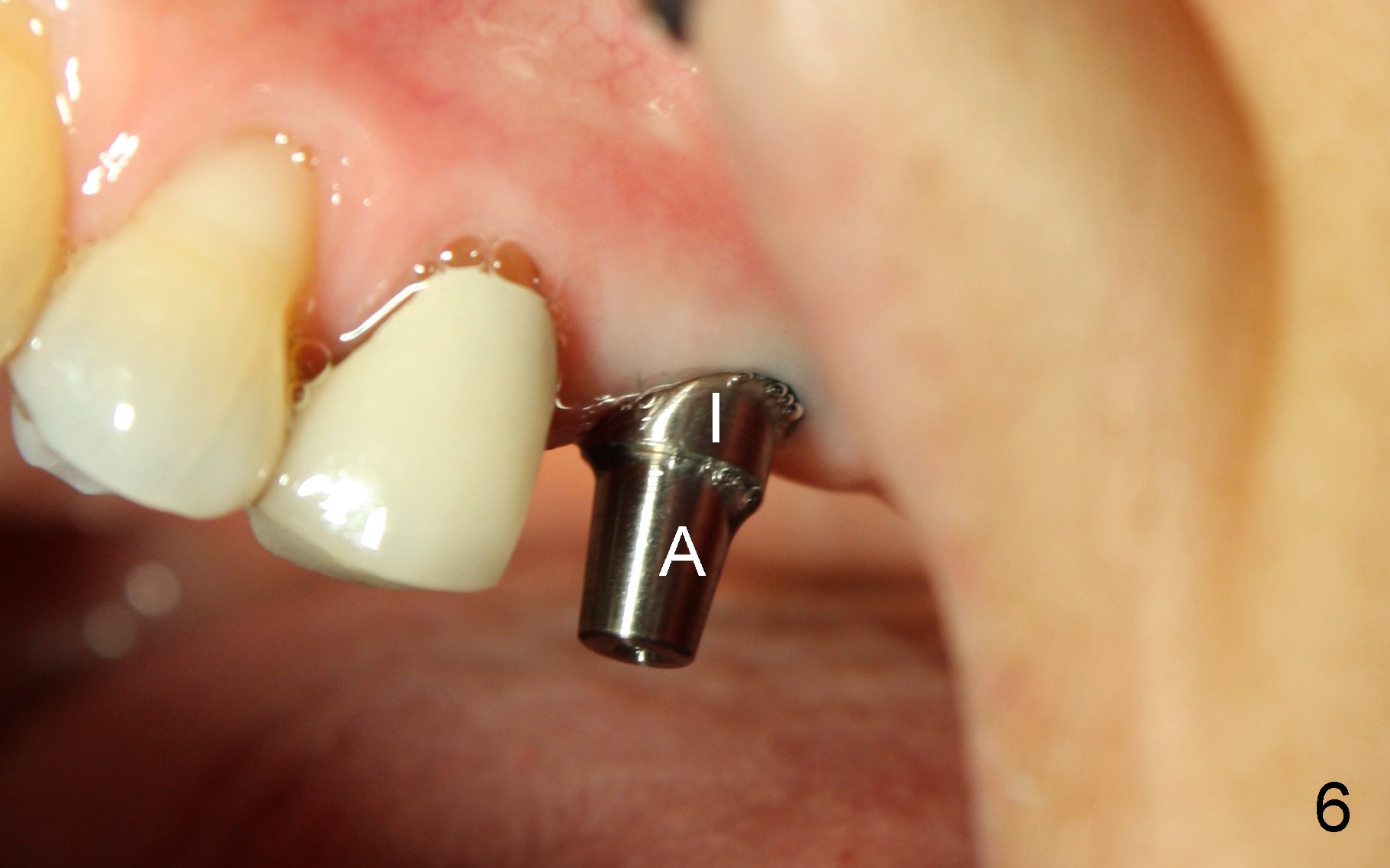
Fig.5, 6 are taken 3 and 4 months post implantation (I: implant; A: abutment).
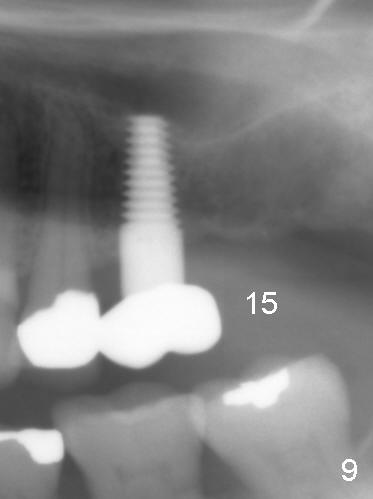
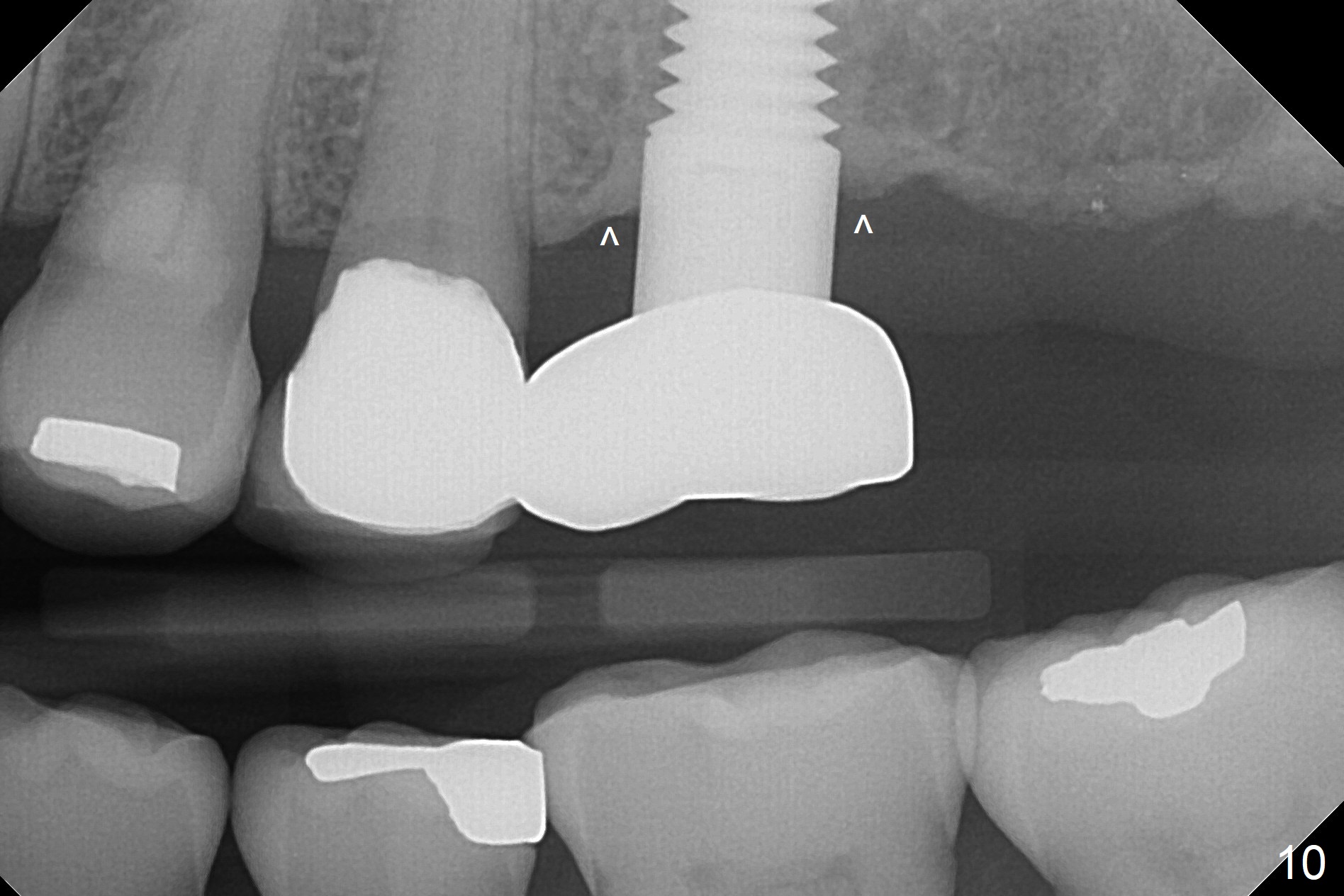
One year 2 months post cementation, the patient complains of inability to chew on the left. It appears that the crown at the site of #14 (Fig.8) is not as large as the tooth #3 (Fig.7); the occlusal contact of the crown is less than that of the tooth #3. The complaint remains the same after crown being remade. It appears that implant at #15 is needed (Fig.9: 1 year 9 months post cementation of #14 crown). The crestal cortical bone is thicker around the implant 2 years 4 months post cementation (Fig.10).
Return to Sinus Lift,
Instrument,
Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 01/09/2014, last revision 09/02/2017