

|
|
|
|
|
|
|
|
|
Sinus Lift Using Osteotomes
When the maxillary posterior bone is low in density, osteotomes can be used for osteotomy and sinus lift at the same time. The bone is to be condensed. More important is that the bone can be pushed all the way from the crest to the sinus.
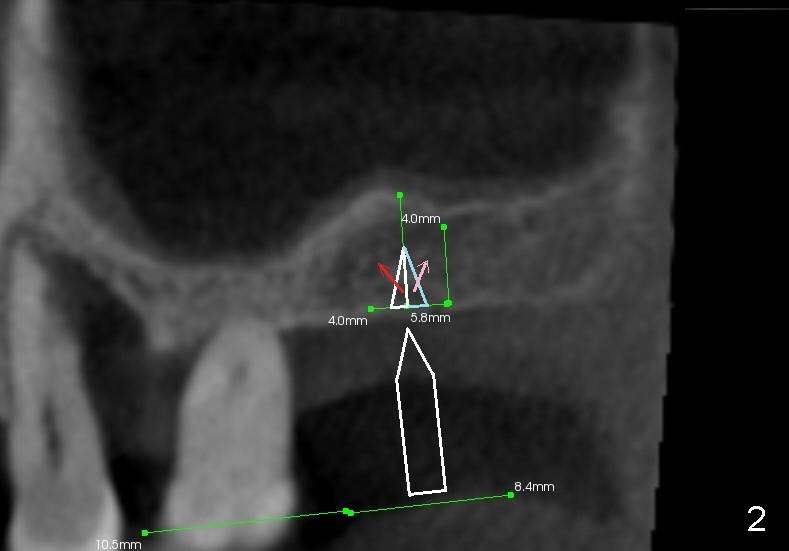
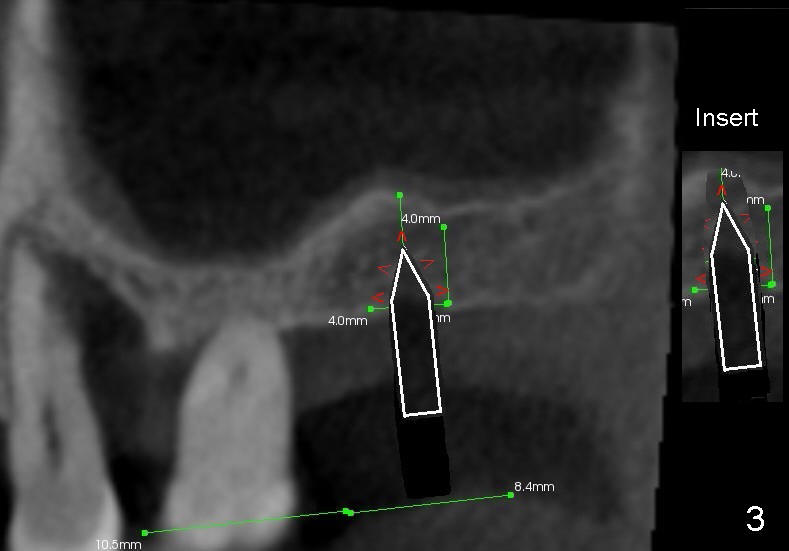
Fig.1 is a sagittal section of the posterior maxilla. A 2 mm (in diameter) round straight osteotome (white box) is going to initiate osteotomy and sinus lift. When the osteotome penetrates the bone initially, the latter is going to be condensed and pushed laterally (mesiodistally) and apically (Fig.2,3 arrows).
As the osteotome advances, some of the bone is brought apically (Fig.3 insert). The tapping with the thin osteotome should be stopped when penetration of the sinus floor is felt. The latter undergoes green stick fracture in a small area (Fig.4 arrows).
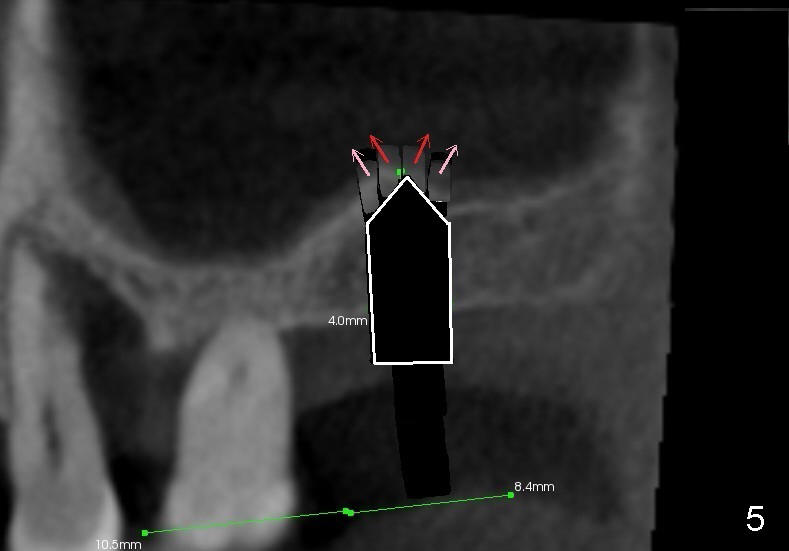
As the diameter of osteotomes increases (from 2, 3 to 4 mm), more of sinus
floor undergoes green stick fracture (Fig.5 pink arrows). At the same
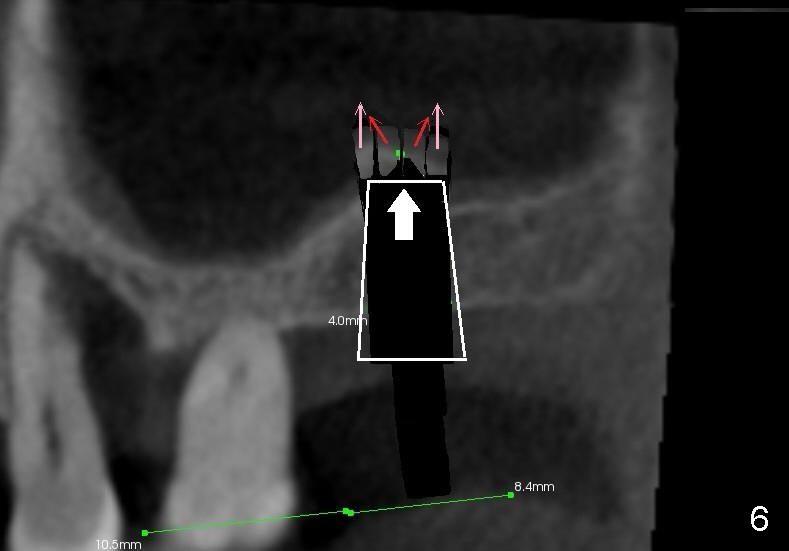
time, more bone is brought apically (not shown). Finally a tapered
osteotome with flat end or tap is used to further lift the sinus floor (Fig.6
white arrow). This time the fractured bone fragments (red and pink arrows)
are more or less at the same level.
The apical end of the ensuing implant
should be covered by vascularized (attached to the sinus membrane) bone
fragments.
Xin Wei, DDS, PhD, MS 1st edition 01/08/2014, last revision 01/08/2014