




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Immediate One Piece Implant Bridge
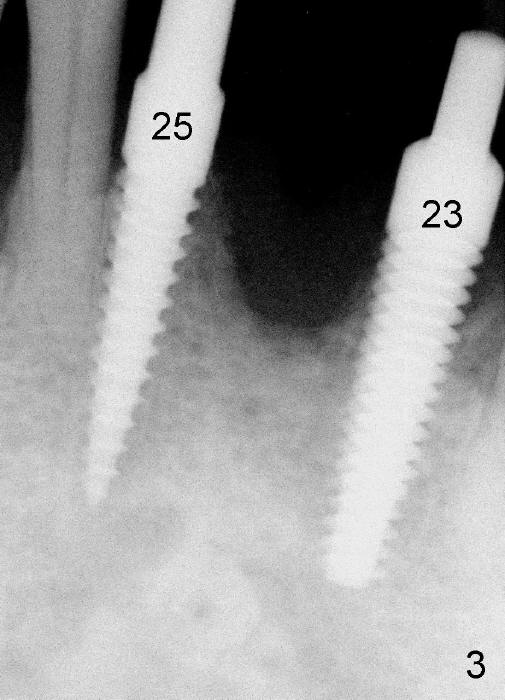
A 51-year-old man is an ex-smoker and has a history of severe periodontal disease (Fig.1). In spite of improvement in oral hygiene, the tooth # 24 falls out spontaneously and is detached from a splinting (Fig.2 ^). It appears that the affected socket is a poor recipient for an implant (*). The neighboring teeth #23,25 have guarded to poor prognosis (Fig.1,2). These two teeth are extracted and replaced by one piece implants immediately (4x17 and 3.5x17 mm, respectively, Fig.3). An immediate provisional fixed partial denture (FPD) is fabricated (Fig.4). The FPD is bonded to the neighboring teeth for additional stability. The arrowhead in Fig.4 indicates a part of a fresh extraction socket; *: upper flipper.
To make a quick and sturdy transitional anterior FPD, a suck-down stent should be used.
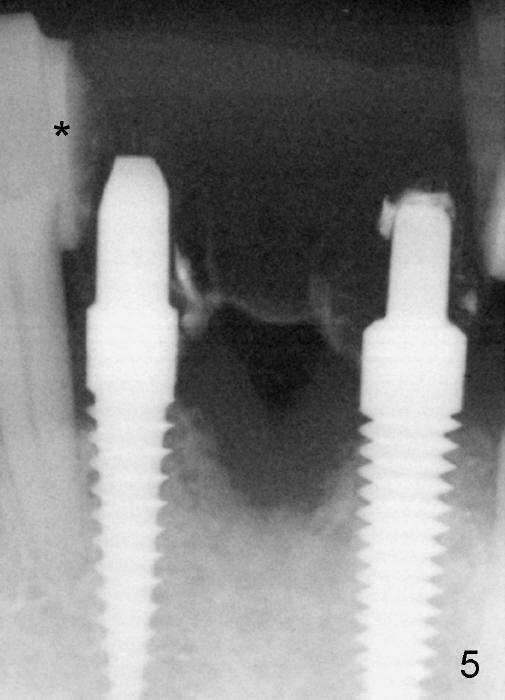
The patient returns for definitive restoration 1 year postop. The provisional FPD is still attached (Fig.5 *) to the neighboring teeth. In fact, the FPD moves together with the neighboring supporting teeth. There is apparently no bone resorption around the implants clinically (Fig.6 between arrowheads).
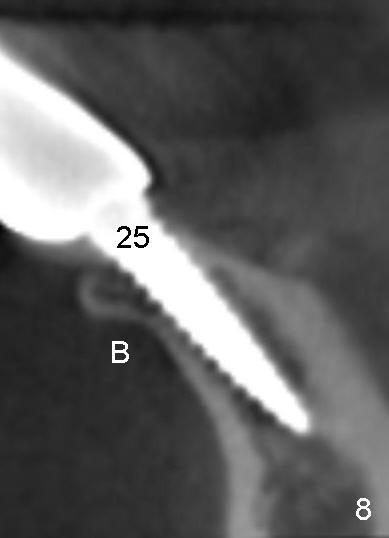
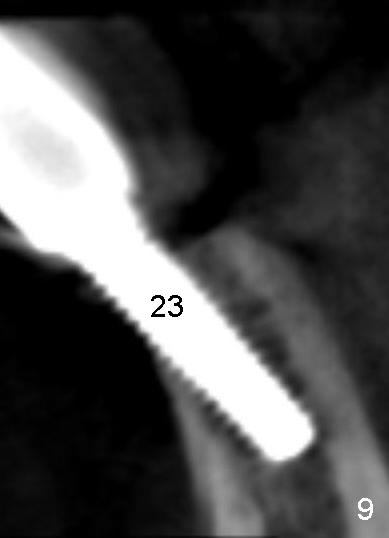
Fig.7 shows definitive bridge just cemented. There is metal exposure associated with the implant at the site of #23 (<), which is consistent with that in Fig.4. The reason for it is revealed by CBCT. The implant is placed buccally (Fig.9, as compared to Fig.8,6). It appears that the smaller one piece implant should be used and placed as lingual as possible.
Our next case features loss of the lower incisors in a small statured lady over 20 years. It shows how difficult to place the smallest one piece implants in an atrophic alveolus.
Return to Lower Incisor Immediate Implant, Systemic Diseases
Xin Wei, DDS, PhD, MS 1st edition 01/11/2013, last revision 04/18/2020