
|
|
|
|
|
|
|
|
||
|
|
|
||
Primary Stability
With one case of immediate implants under the belt, CT is immediately felt to be not so necessary for most of immediate implant cases, especially in the lower anterior area. In fact, immediate implant can reduce the chance to take CBCT.
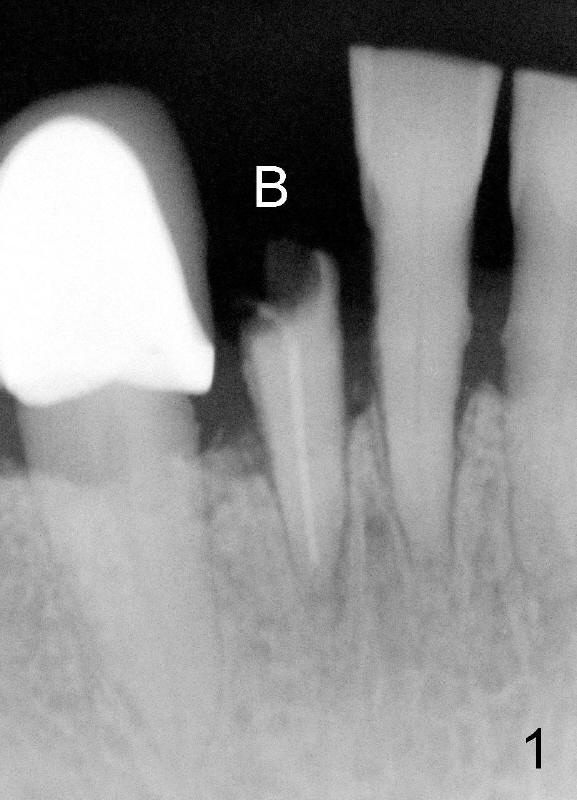
A 63-year-old lady breaks a lower incisor (Fig.1 B). The tooth with the disadvantageous crown-to-root ratio can still break. It suggests that an implant 3 to 4 mm longer than the root should be functional. There is no important structure apically. Therefore, no CT is needed for this case.
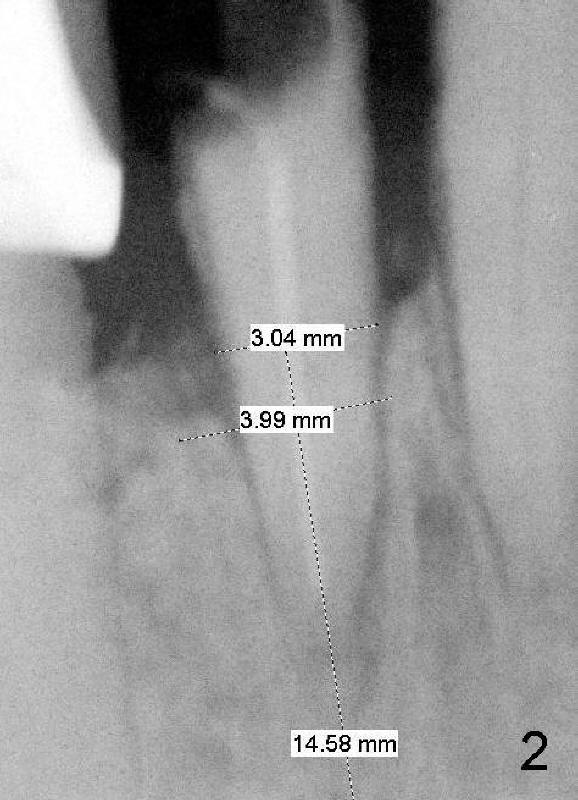
The mesiodistal width of this incisor is 3 mm (Fig.2). There is plenty of space regarding the neighboring teeth. It appears that an implant with 4 mm in diameter should not invade the roots of the neighboring teeth. The benefit using the relatively large diameter implant is to close the buccolingual socket, which is usually larger than mesiodistal.
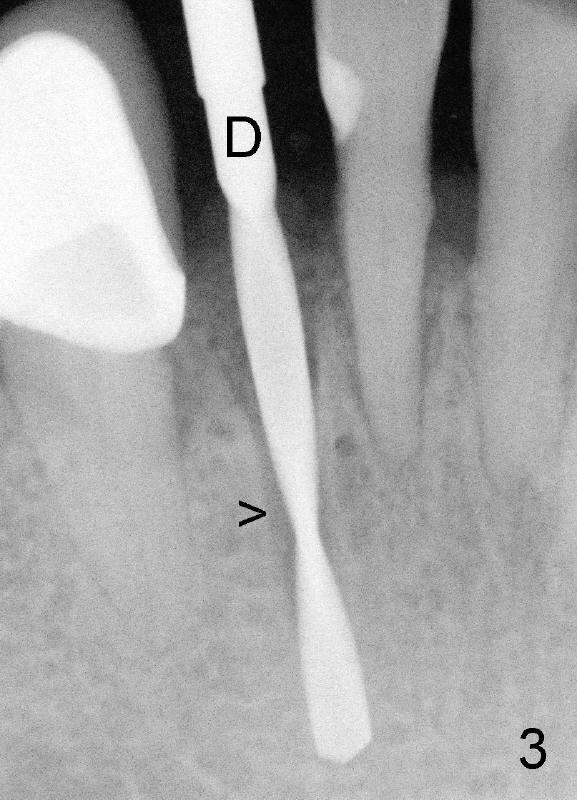
A 2 mm pilot drill (Fig.3 D) is used to extend the socket. The arrowhead (>) indicates the original root tip. With the guidance of the socket, direction of drilling is much easier. This is one of advantages of immediate implant. There is something reliable to follow.
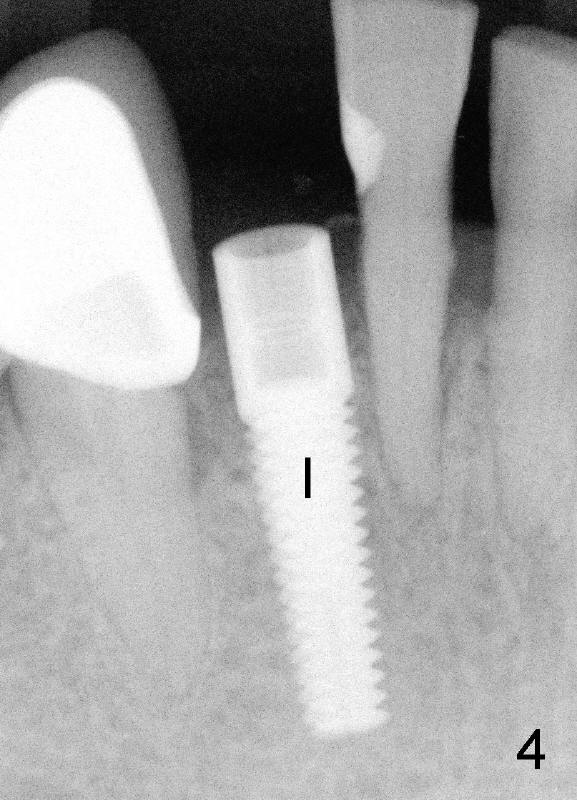
A 4x17 mm implant is immediately placed with primary stability clinically (Fig.4 I). Torque wrench has yet to be purchased. There is gap proximally between the bone and the implant.
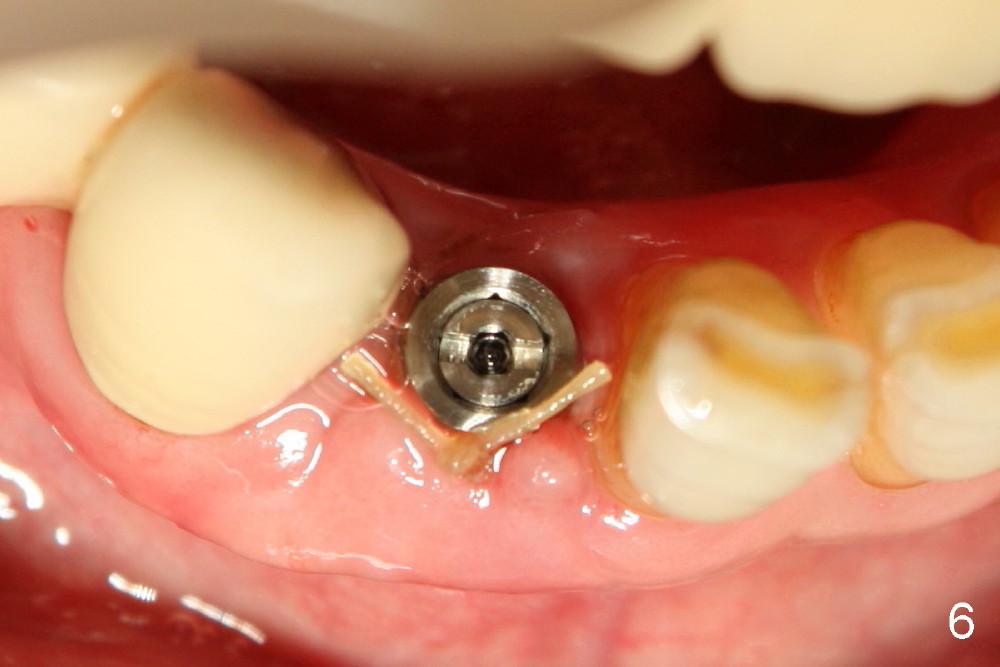
The buccal gap is closed by elevating and then suturing the buccal flap (Fig.5). The white oval outline represents the original socket. The wound heals uneventfully, 6 days postop (Fig.6) .
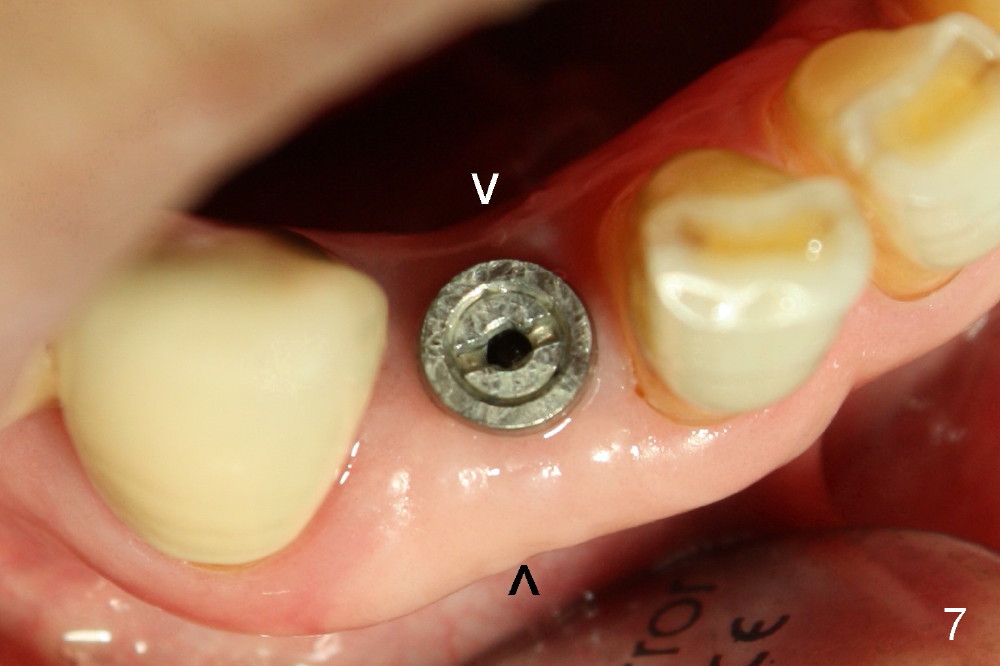
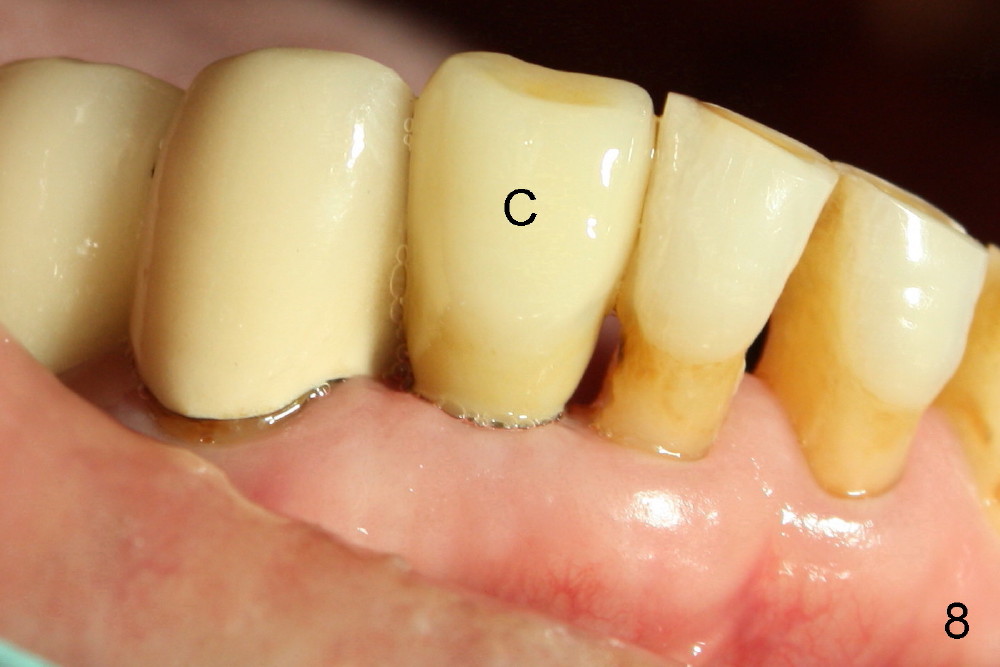
There is no alveolar atrophy seven months postop (Fig.7 between arrowheads, as before (Fig.5,6)). A definitive crown looks natural with the gingiva (Fig.8 C).
The next immediate implant in the lower incisor region is going to be immediately loaded since the edentulous space (occlusal table) is quite narrow and the occlusal force should be low.
Preface to Immediate Implant for Lower Incisors
Xin Wei, DDS, PhD, MS 1st edition 09/11/2012, last revision 01/21/2014