





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mission is Accomplished (Septal Implantation)
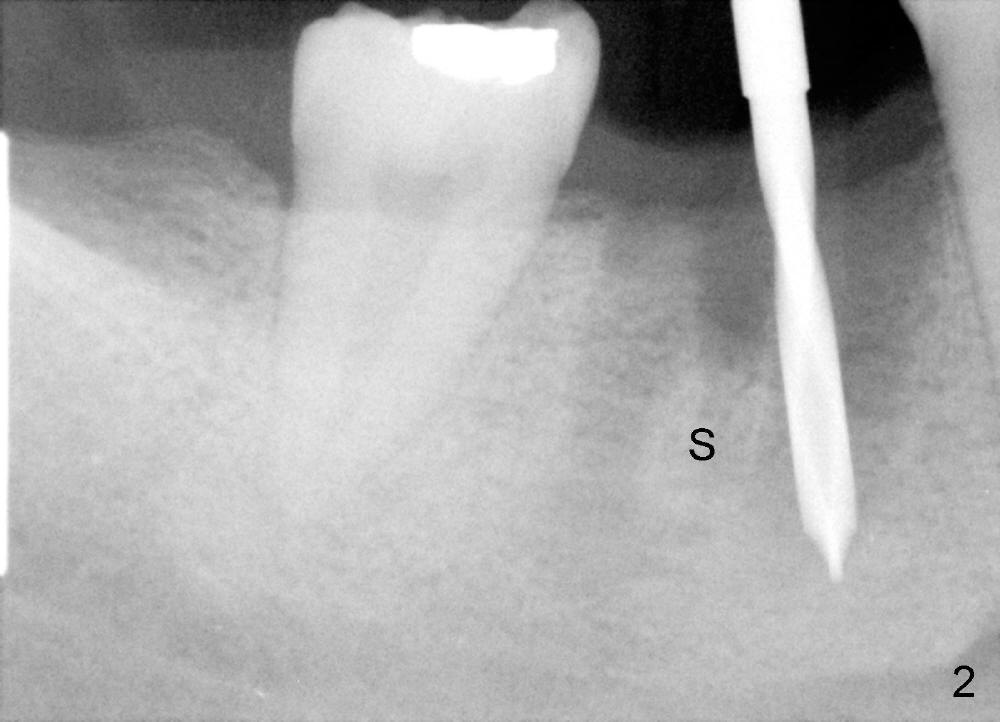
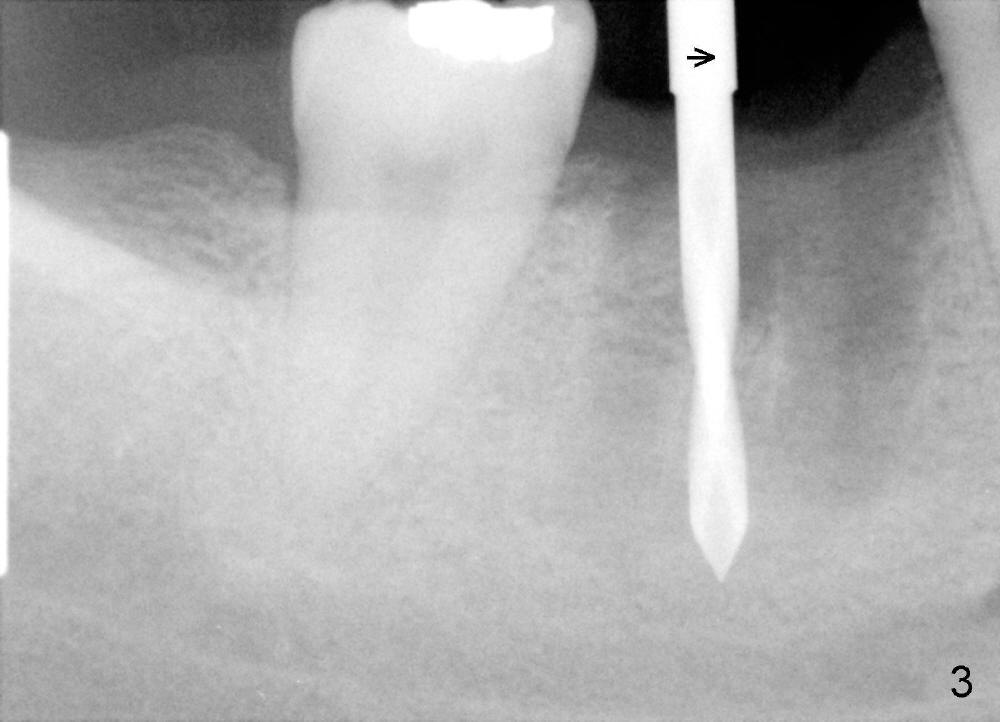
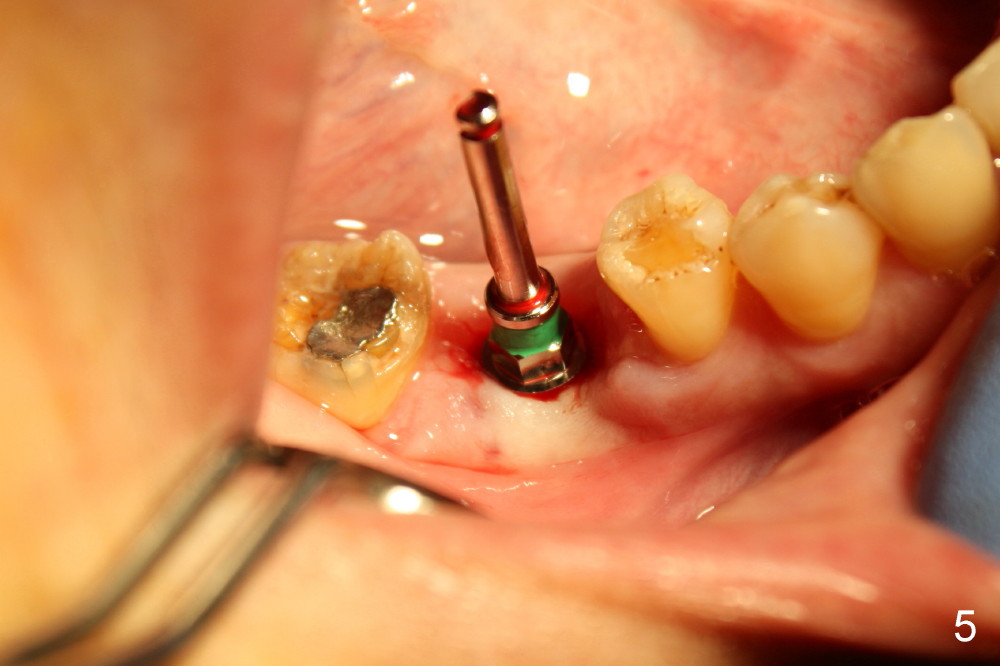
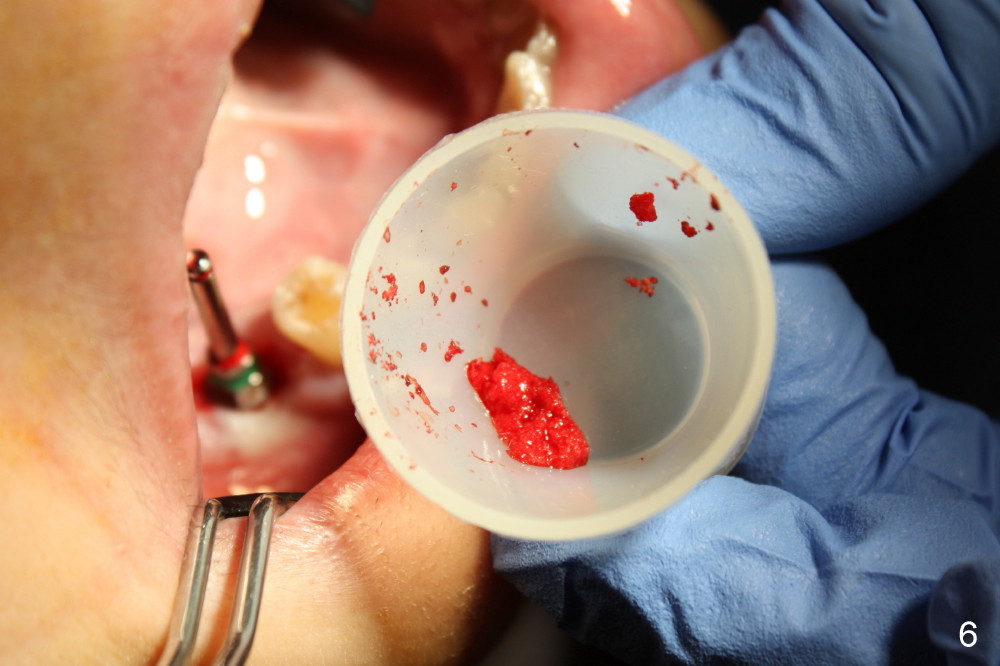
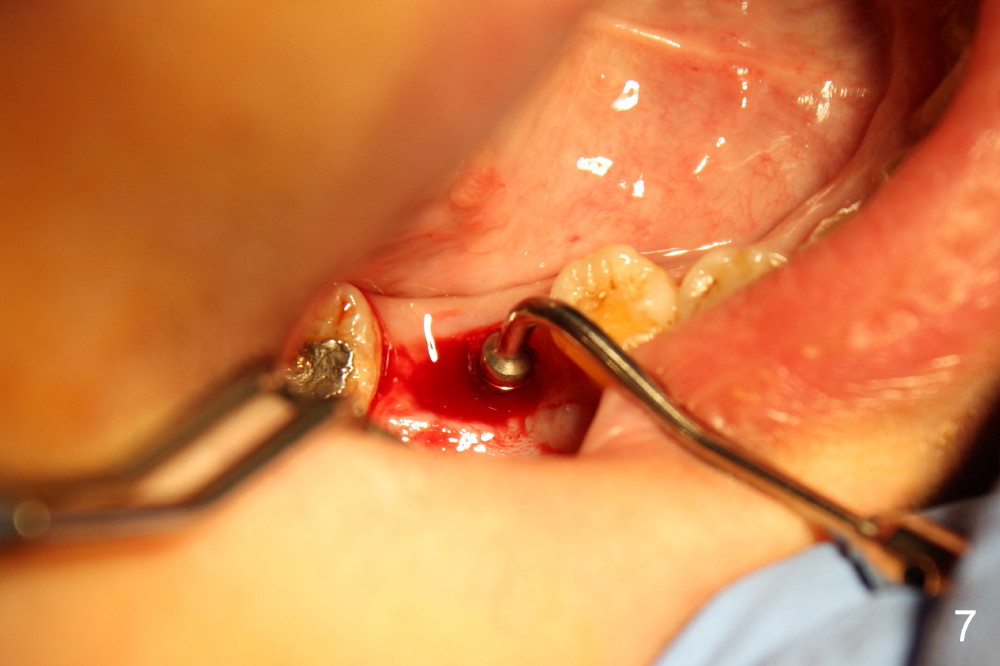
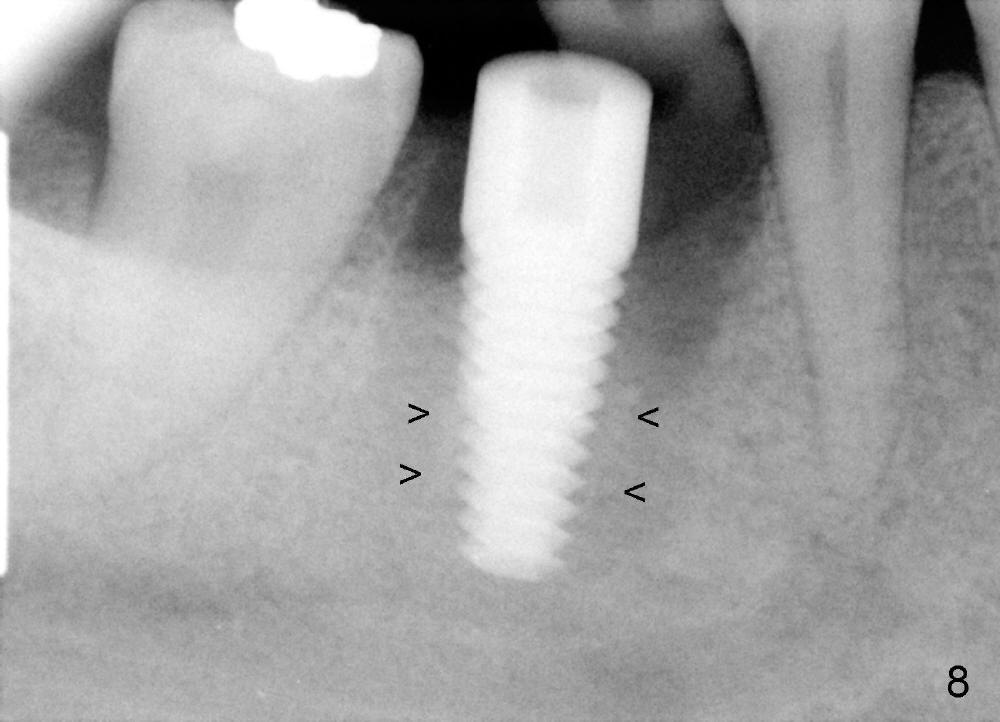
The socket of #30 heals one month after extraction (Fig.1 *). What is unexpected is that the alveolus has started to shrink (follows arrowheads). It is also unexpectedly easy to tap in RT2 (flapless). With insertion of a 2.0 mm pilot drill, PA reveals that osteotomy is not inside the septum (Fig.2 S). Redirecting osteotomy with the same pilot drill leads to insertion into the septum, but the upper end of the pilot drill should be moved mesially in next steps (arrow). With that and treatment plan in mind, combination of osteotomes, Bicon reamers and taps results in right trajectory (Fig.4 * (5x20 tapered tap), Fig.5 (6x17 tapered tap)). Harvested bone (Fig.6) is transferred to the mesial socket and condensed (Fig.7). Insertion torque of 6x17 mm implant is more than 60 Ncm. The lower end of the implant remains in the center of the septum (Fig.8 <). The gingiva contacts the implant tightly (Fig.9, 10) except mesiobucally (Fig.9 <). Periodontal dressing is used to protect the wound (Fig.11,12).
Unfortunately infection occurs postoperatively. The periodontal dressing is dislodged less than a week postop. The wound/bone graft lacks protection. In order to keep perio dressing longer in the mouth, a short abutment is placed immediately on a temporary basis. Once the perio dressing has achieved its goal, the abutment is replaced with a cover screw.
Xin Wei, DDS, PhD, MS 1st edition 09/29/2013, last revision 07/26/2014