
|
|
|
|
|
|
|
|
|
|
|
Preparation for Upper Molar Immediate Implants
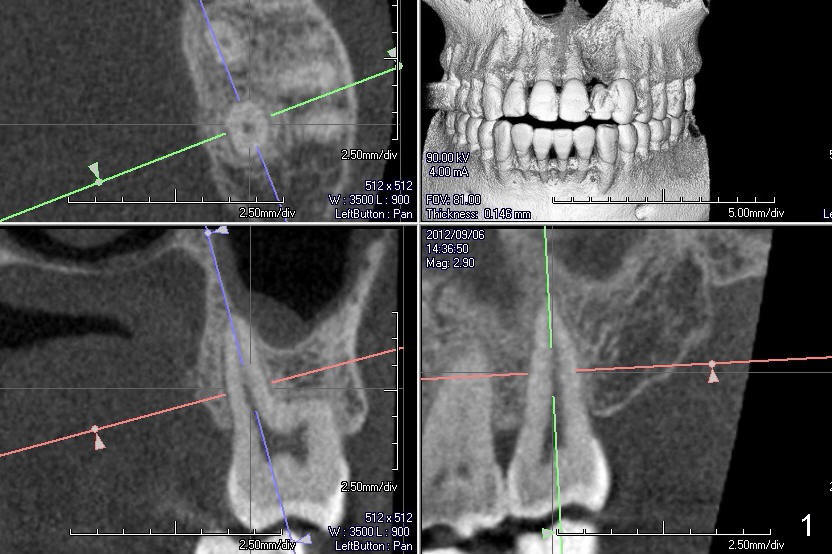
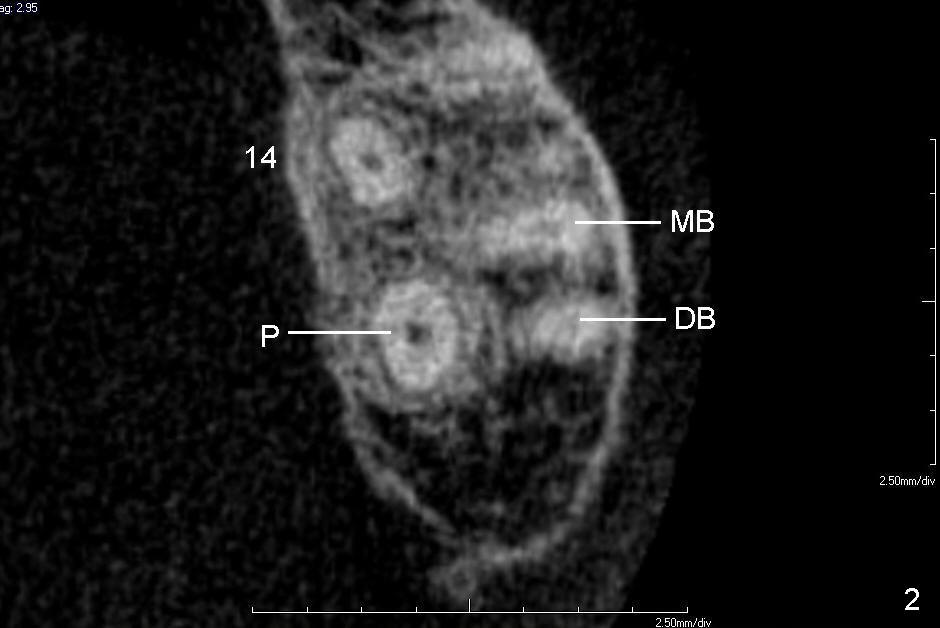
A 60-year-old man requests replacing the teeth #2 and 3, which have root fracture. Both of these two teeth have 3 roots (palatal (P), mesiobuccal (MB) and distobuccal (DB) (X-ray not shown). CT images from a different patient are used instead (Fig.1-3). The upper left image of Fig.1 (i.e., Fig.2) is an axial section, lower left (Fig.3) coronal and lower right sagittal.
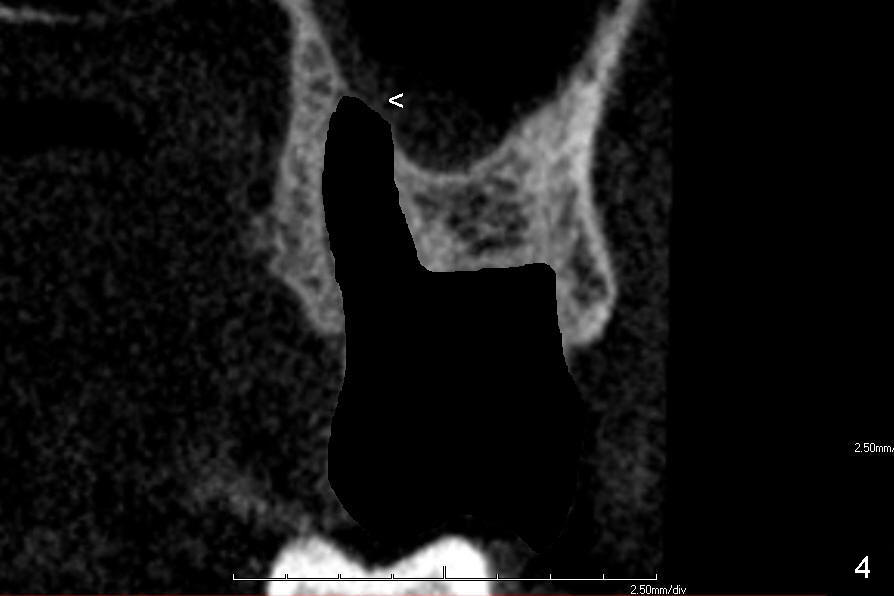
One of these two teeth is to be extracted first (Fig.4). Granulation tissue is removed, followed by copious irrigation. The socket morphology is studied. The apicobuccal aspect of the palatal socket is so thin that it may be perforated during tooth extraction and/or bone expansion mentioned below (Fig.4 <). Clindamycin gauze is placed in the extraction socket while the other tooth is being extracted.
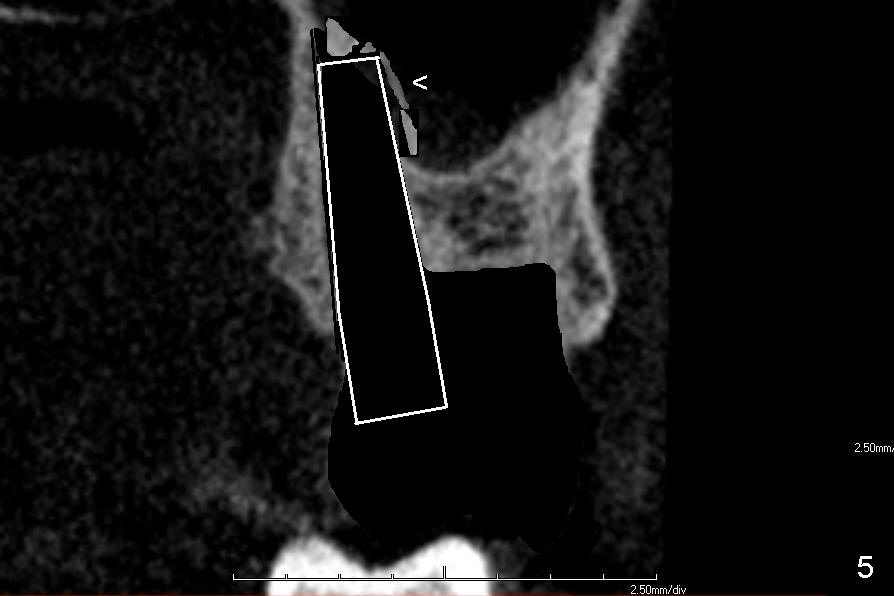
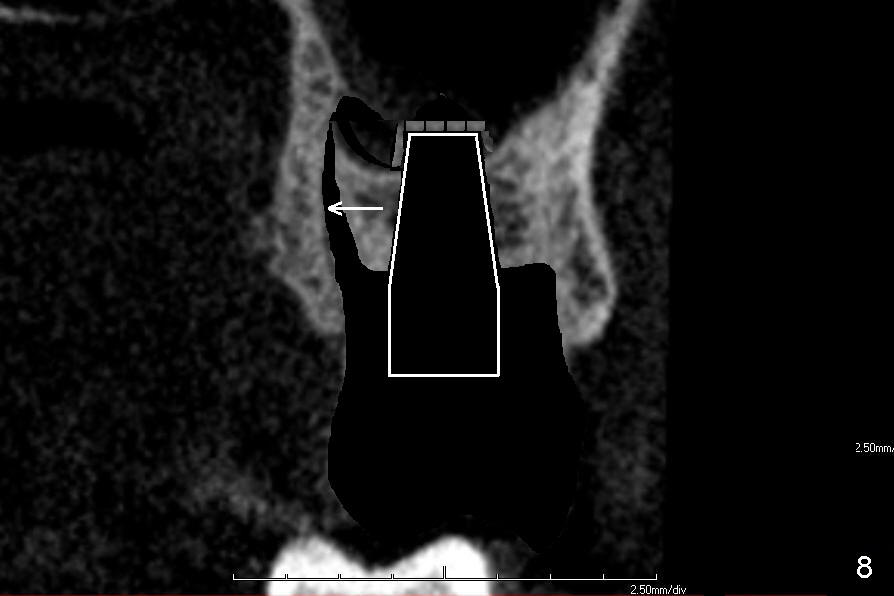
If the septum is small or destroyed by the infection, an implant will be placed in the palatal root (Fig.5), since it is the biggest among these 3 roots (Fig.2). The advantage is that the implant is longer than that placed in the septum (Fig.8). The drawback is that the implant is off center (Fig.5, as compared to that placed in the septum (Fig.8)). The implant placed in the palatal socket is relatively small in diameter. The whole socket will not be occupied by the implant. Collagen membrane will be used to help close the socket as well as bone graft.
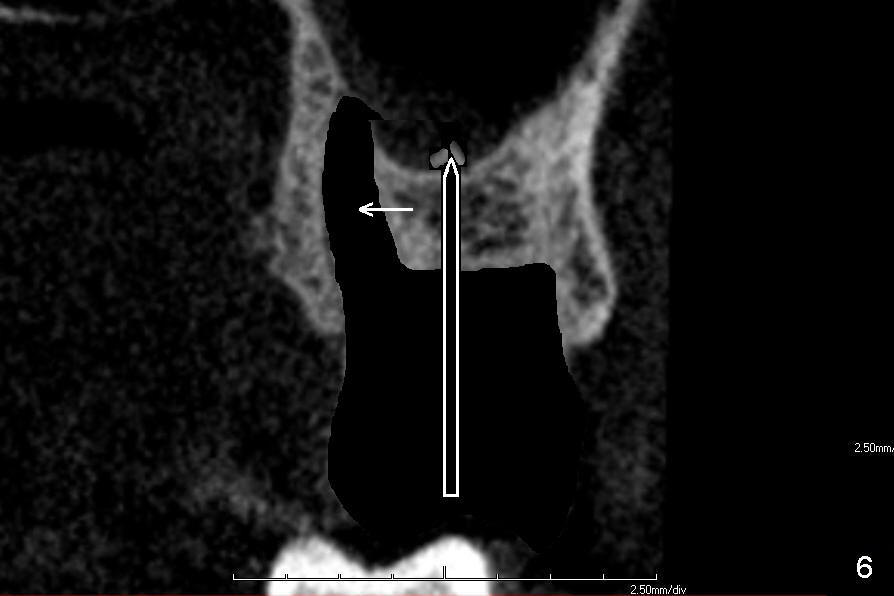
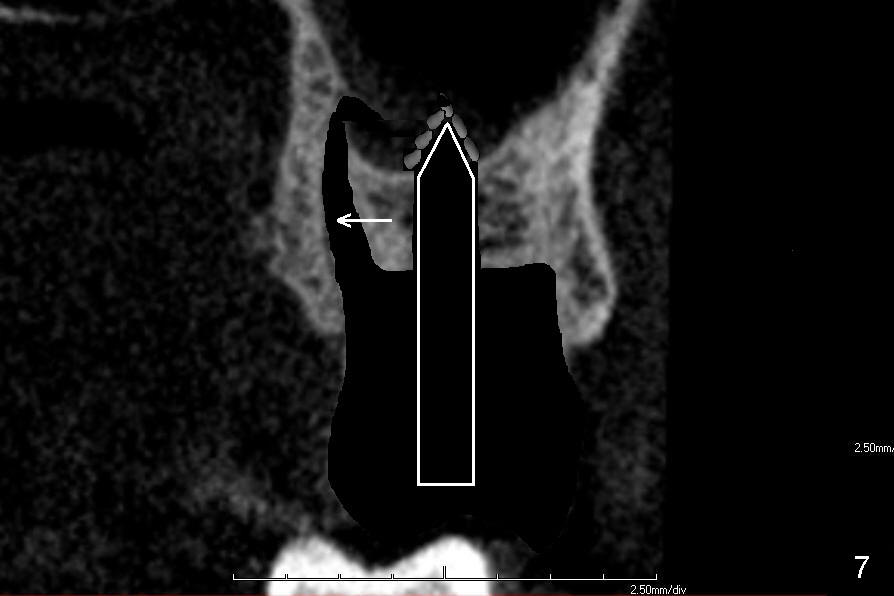
If the septum is not so bad in size, osteotomes (RT series) will be used to expand it (to obliterate 3 sockets) and finish sinus lift to increase implant length if bone is not too hard to manipulate (Fig.6,7). Osteotomy is finished by using proper size and length of taps. Finally a large, but relatively short implant is placed in the septum (Fig.8). Arrowheads in Fig.6-8 indicate that as osteotomes are driven in sequentially (Fig.6,7 white box) and the implant is placed (Fig.8), bone segment may be moved palatally to obliterate the palatal socket gradually.
If the maxilla is too hard for osteotomes, reamers are used to create osteotomy. The bone is to be saved for grafting. If the sepum is totally destroyed, the largest implant is placed in the middle of the socket (7 or 8 mm in diameter).
Xin Wei, DDS, PhD, MS 1st edition 12/22/2013, last revision 12/22/2013