

|
|
|
|
|
|
|
|
|
|
|
|
Watch Closely Implant Trajectory and Change it In Time
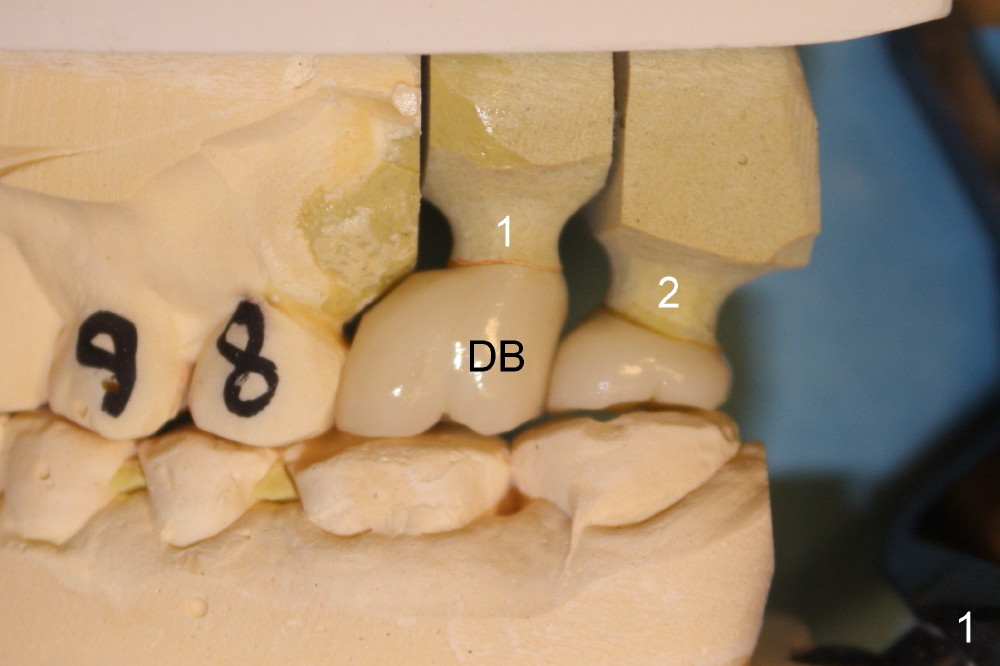
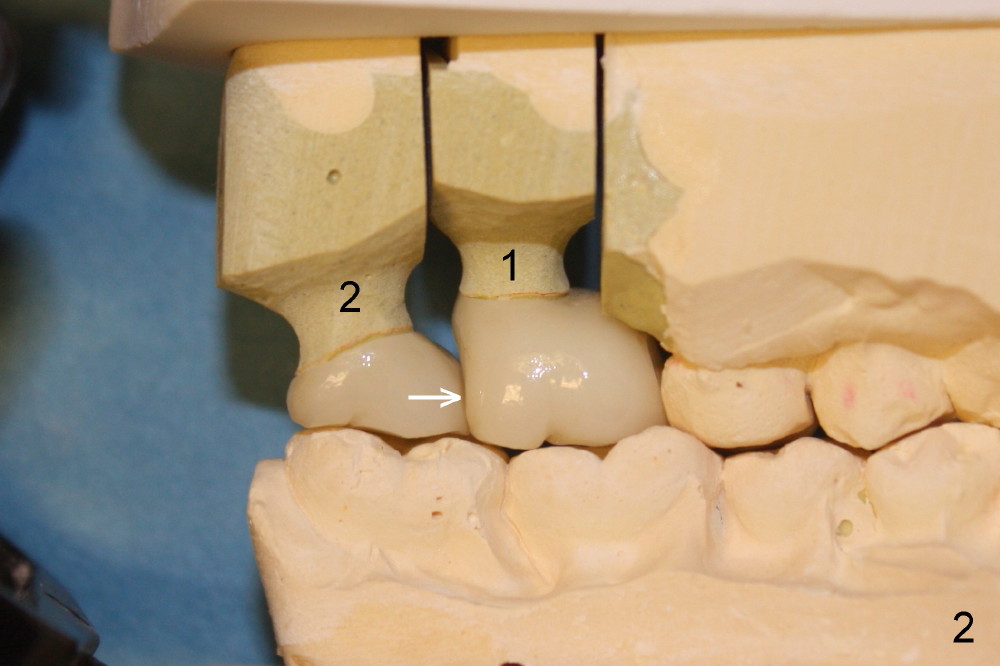
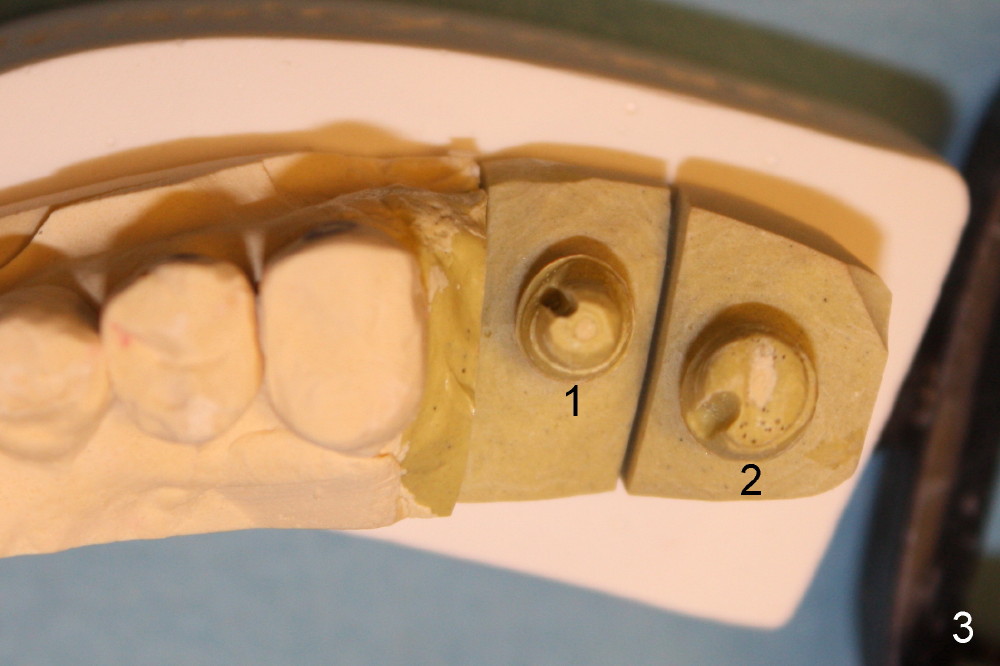
On the day of delivery, the model is studied (Fig.1 (buccal), 2 (lingual), 3 (occlusal)). The implant at the site of the1st molar (#1 in Fig.1-3) is placed distally; it is at the distobuccal cusp (DB in Fig.1). The crown of the 2nd molar (#2) has to extend mesially (Fig.2 arrow) for compensation. The buccolingual width of these two upper molar crowns is reduced, as evidenced by the edge to edge or mild cross bite of occlusal scheme (Fig.4). Anyway, it appears that the implant at the first molar is malpositioned. How to prevent it?
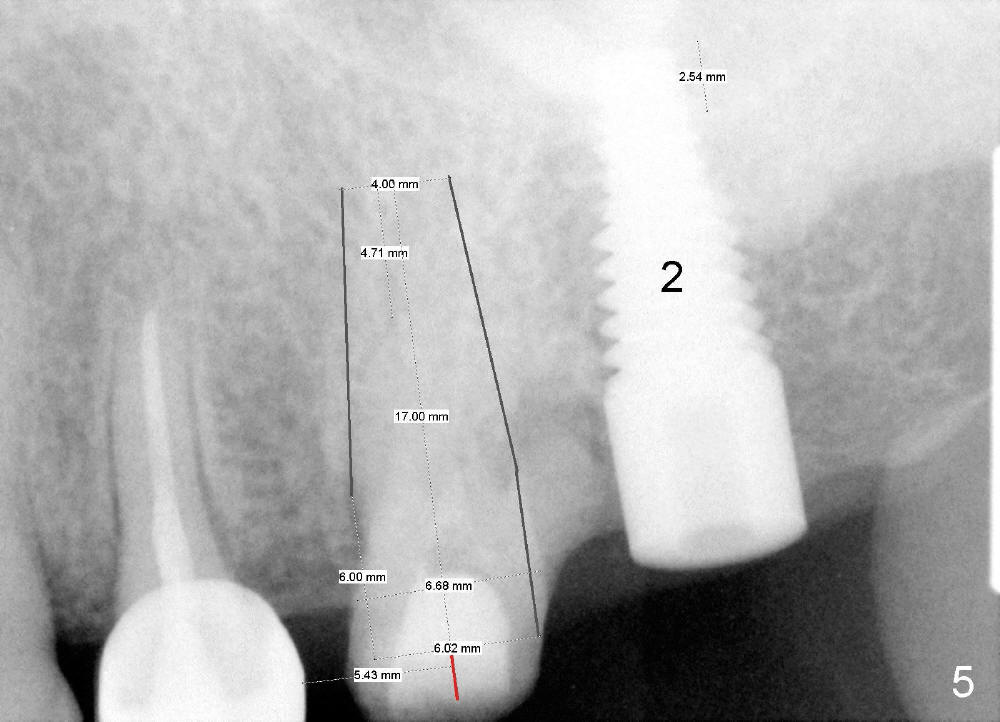
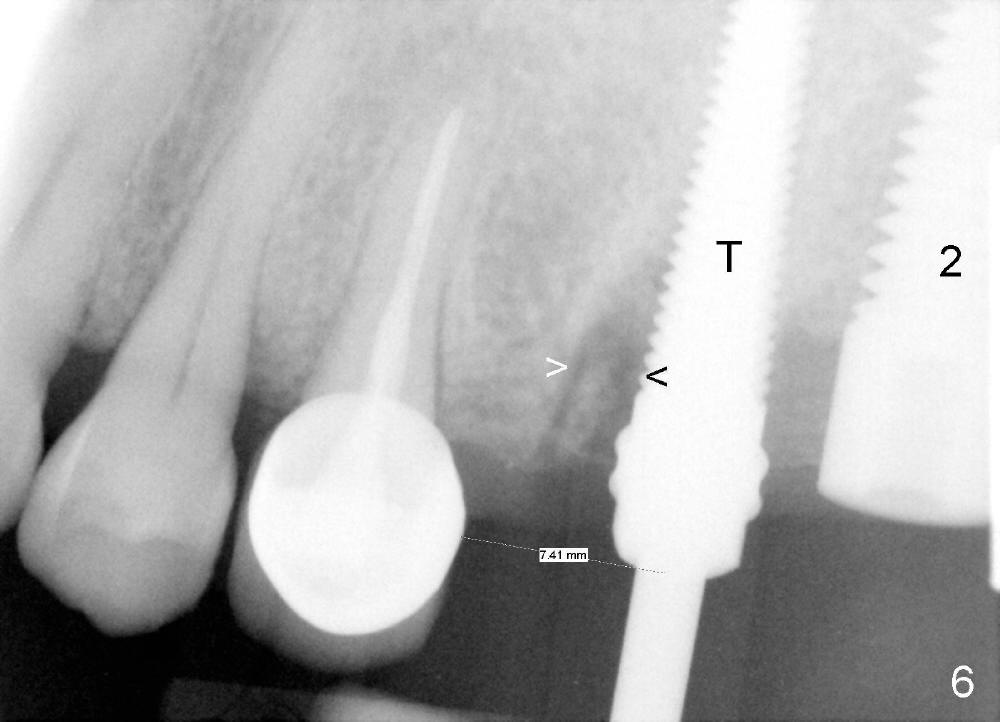
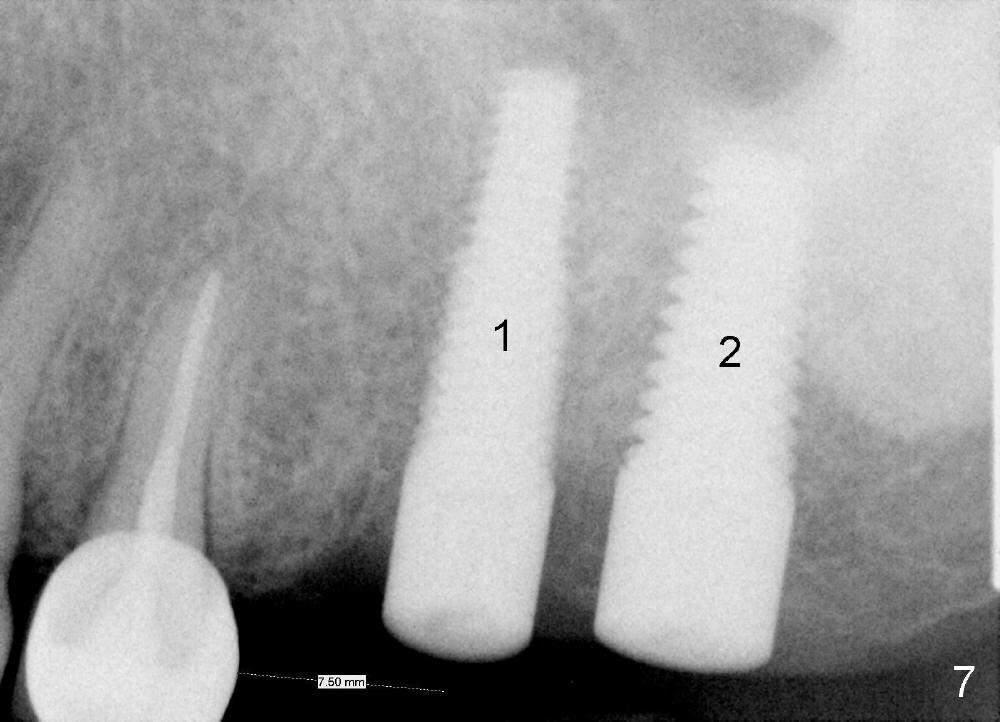
In fact, the implant at the 1st molar is planned to be placed 5.5 mm from the distal surface of the 2nd premolar (Fig.5). When the 1st intraop PA is taken with a 4.5x20 mm tap (Fig.6: T), the deviation is not noted (Fig.6: 7.5 mm vs. 5.5 mm in Fig.5). The trajectory of the implant (5x20 mm) remains deviated (Fig.7).
The trajectory should be corrected as early as possible and by changing the direction (Fig.8: from black line to red one). It should be not so difficult because of soft bone in the posterior maxilla and the mesiobuccal socket space (Fig.6 between arrowheads). It should be not too late to change the trajectory of an implant just placed.
Return to
Upper Molar Immediate Implants
Xin Wei, DDS, PhD, MS 1st edition 05/09/2014, last revision 05/09/2014