

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Large Implant or Large Healing Abutment is Needed for Molar Immediate Implantation
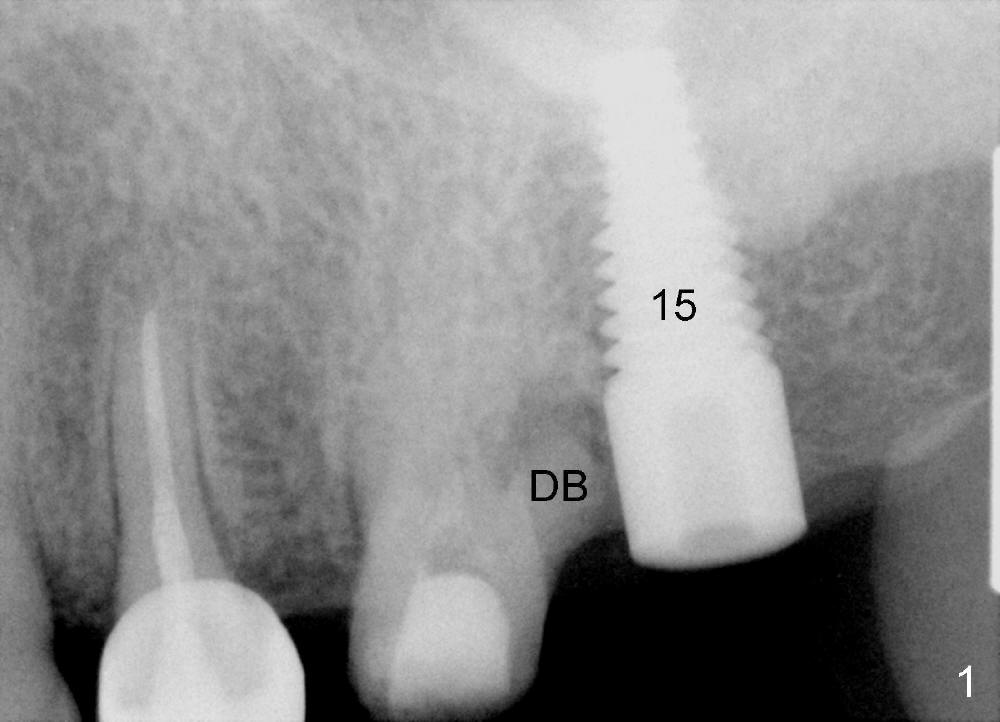
A 50-year-old man has history of a cantilever bridge in the upper left quadrant (from #13 to 15, Fig.1). After bridge removal, a 6x17 mm implant is placed at the site of #15 and root canal therapy is attempted in #14 without success, because of canal obliteration. The tooth is deemed non-salvageable due to the distobuccal root fracture and associated periapical lesion (DB).
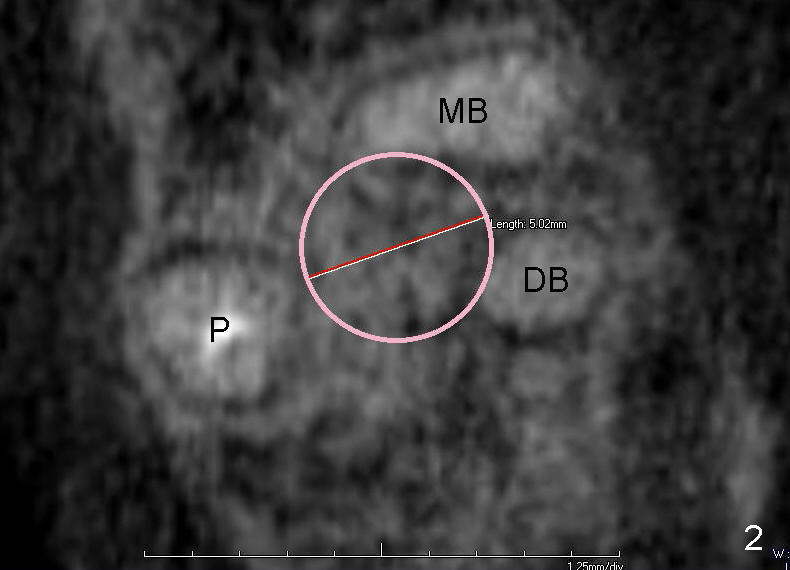
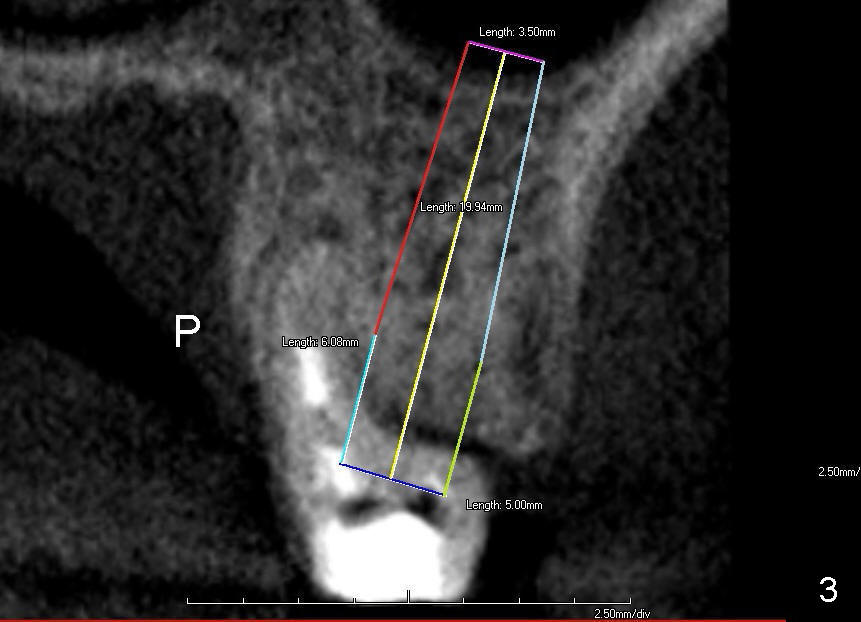
The tooth #14 has a large septum, which can hold an implant with diameter of 5 mm (Fig.2, CT axial section). Coronal section shows that the length can be 20 mm (Fig.3).
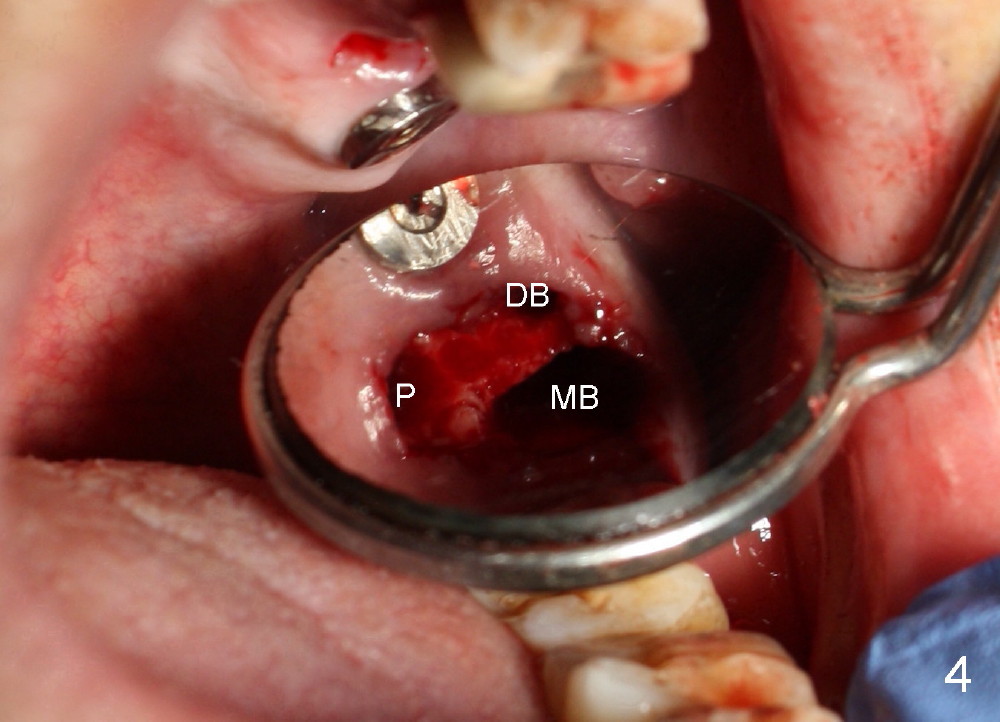
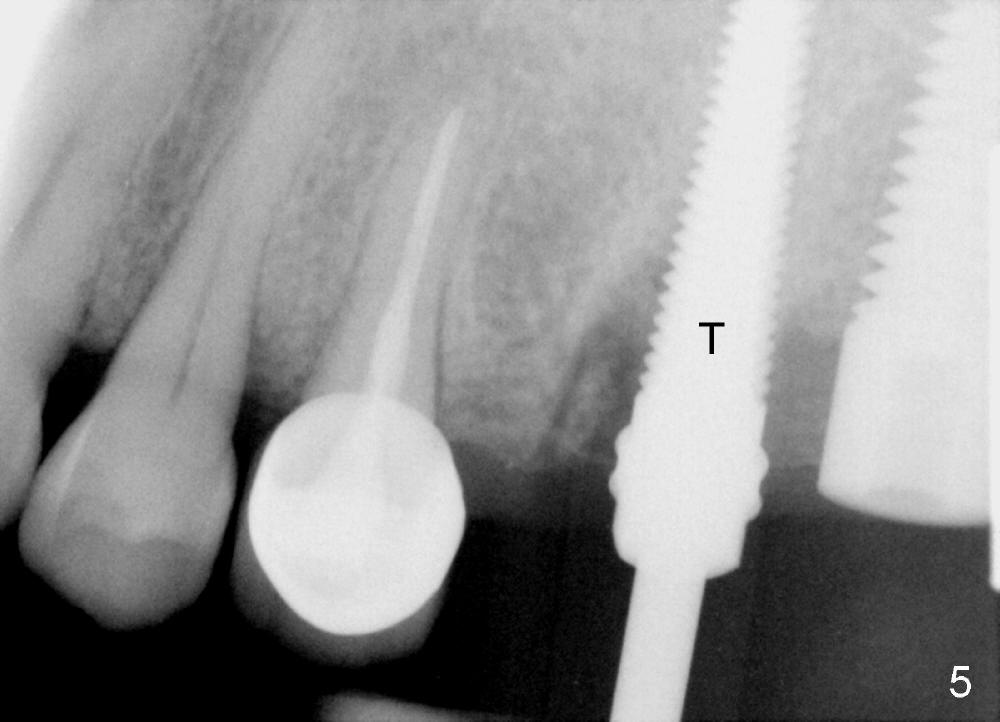
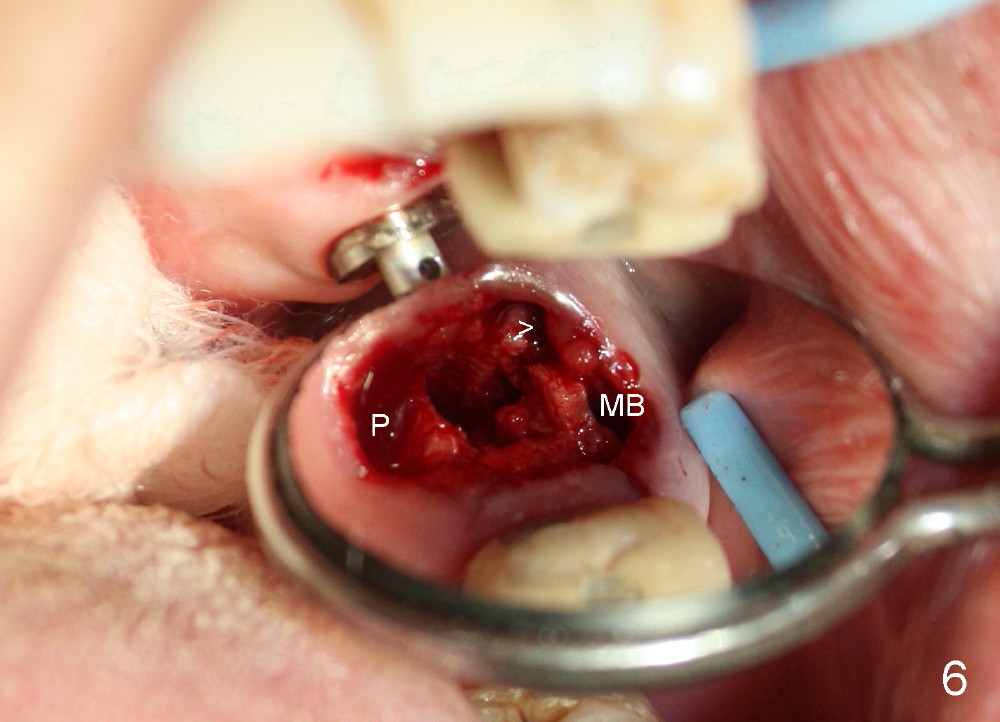
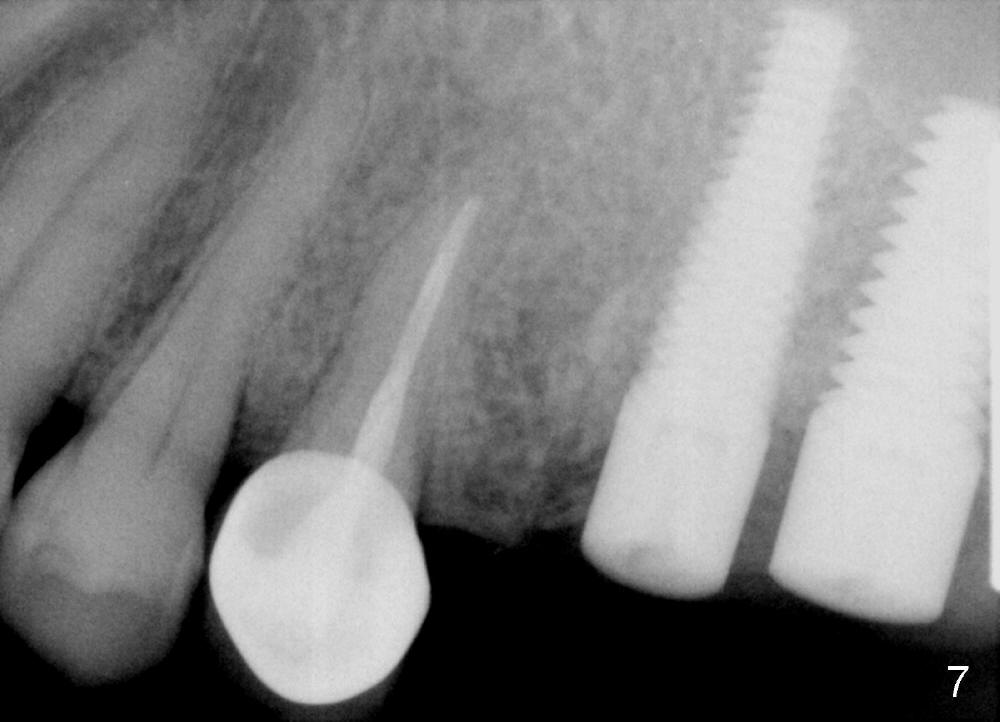
Fig.4 shows the septum between 3 roots (P: palatal, MB: mesiobuccal, DB: distobuccal) after extraction. Osteotomy is formed in the septum mainly by using osteotomes, followed by tap drill (Fig.5: 4.5x20 mm). When a 5x20 mm tap is removed, the osteotomy deviates buccally (Fig.6 arrowhead and MB). Finally a 5x20 mm implant is placed at the site of #14 (Fig.7).
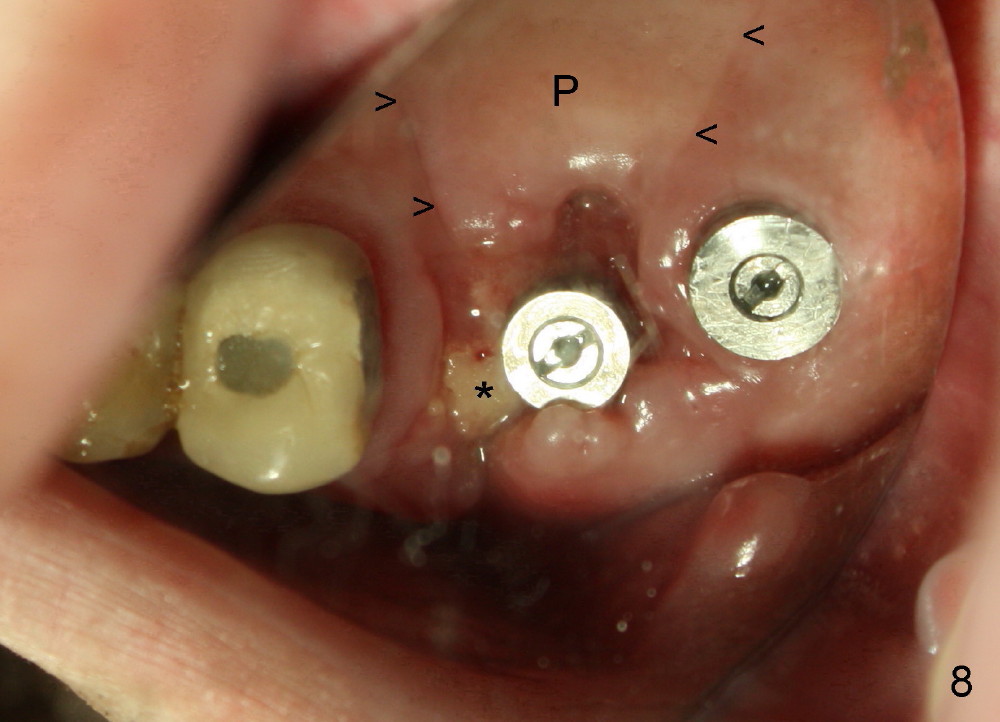
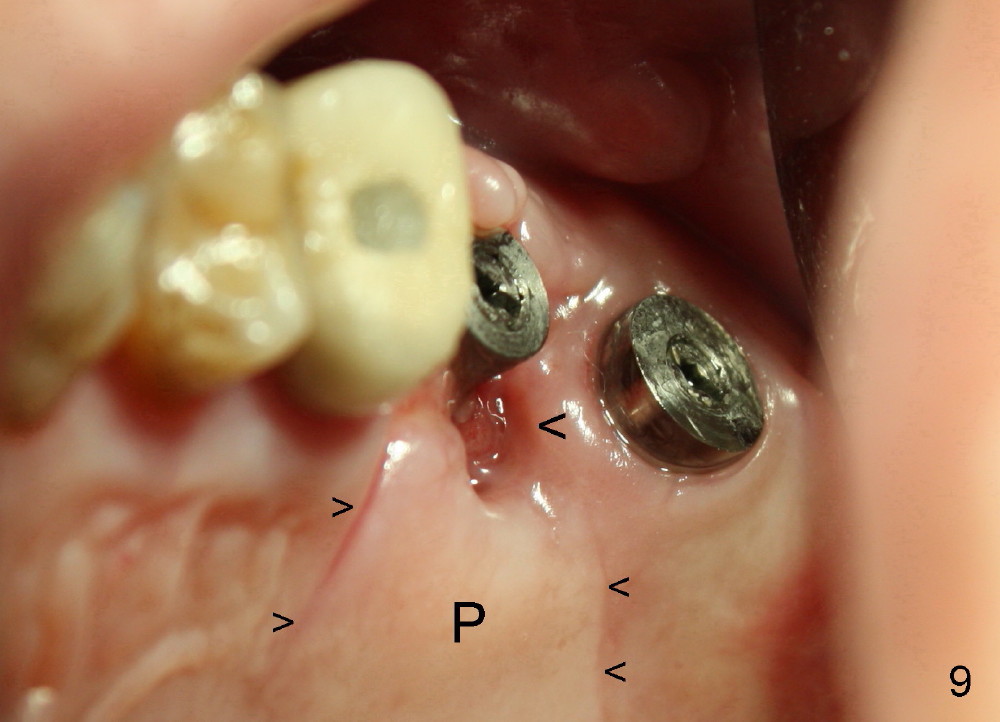
In spite of releasing buccal and palatal (P) flaps with suturing (Fig.8,9 small arrowheads), the palatal socket is exposed 2 weeks postop (big arrowhead and ). The mesiobuccal bone is also exposed (Fig.8 *). The patient reports bleeding and pain immediately postop. Both can be prevented if a large healing abutment is used (8 or 9 mm in diameter) or an immediate provisional is fabricated.
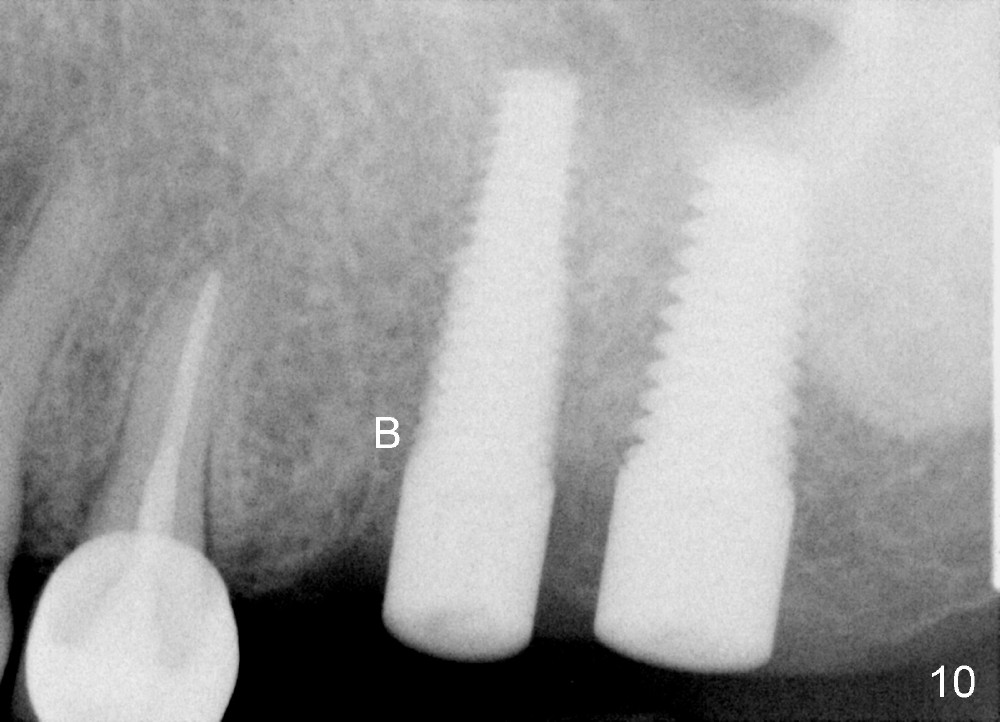
Three months and a half postop, there is bone growth in the previous mesiobuccal socket (Fig.10 (B), compare Fig.5,7). Soft tissue also heals (Fig.11). Using a larger implant (7 mm in diameter) may facilitate wound healing (Fig.12, as compared to Fig.2).
With critical eyes, you may notice that the implant at the site of #14 is placed distally. How to prevent it?
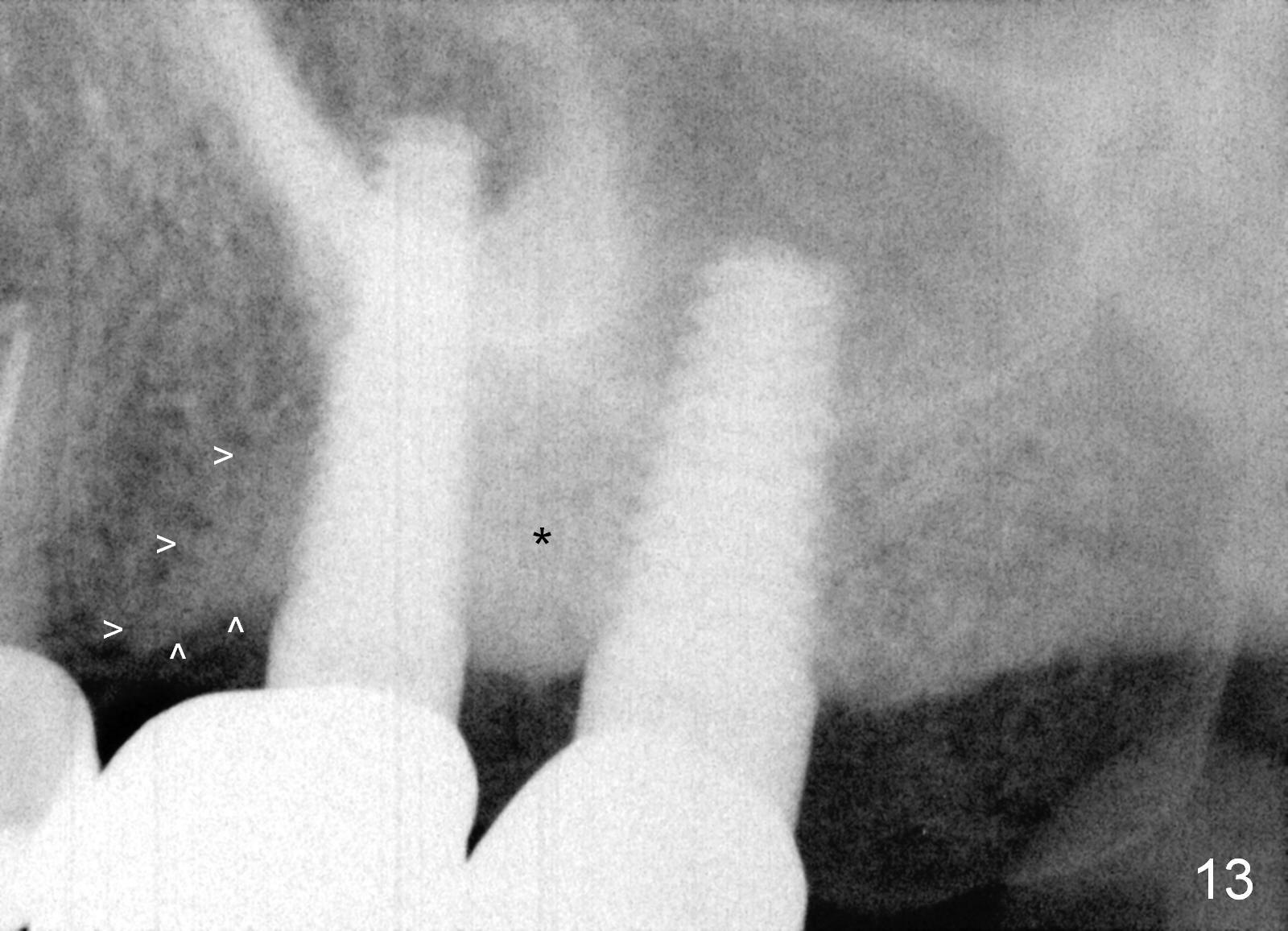
Bone density increases mesially (Fig.13 arrowheads) and distally (*) 1 year 2 months post cementation, 1 year 7 months postop, probably due to the response to the cantilever effect.
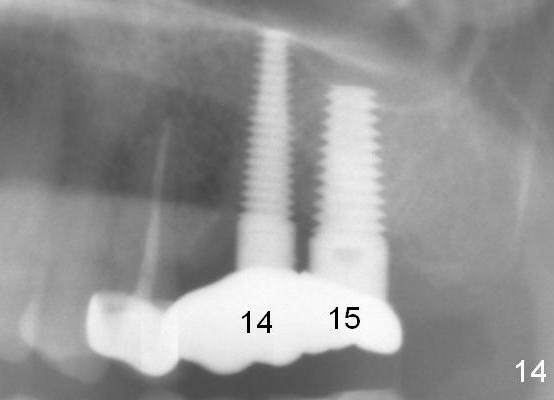
Partially due to severe food impaction on the right, the crown at #15 fractured and dislodged 2 years 6 months post cementation. The unipost was found to be loose. When the new crown at #15 was delivered, the abutment at #14 was mobile. After rebonding the abutment, the crown was redone. Fig.14 is taken after cementation at #14. The looseness of the abutments is the result of off-centered implant placement and bruxism.
Upper Molar Immediate Implants, Introduction to Immediate Implants
Xin Wei, DDS, PhD, MS 1st edition 12/10/2013, last revision 12/23/2016