







|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
||
|
|
|
||||
|
|
|||||
How does Immediate Implant Reduce Possibility of Injury to Mental Loop?
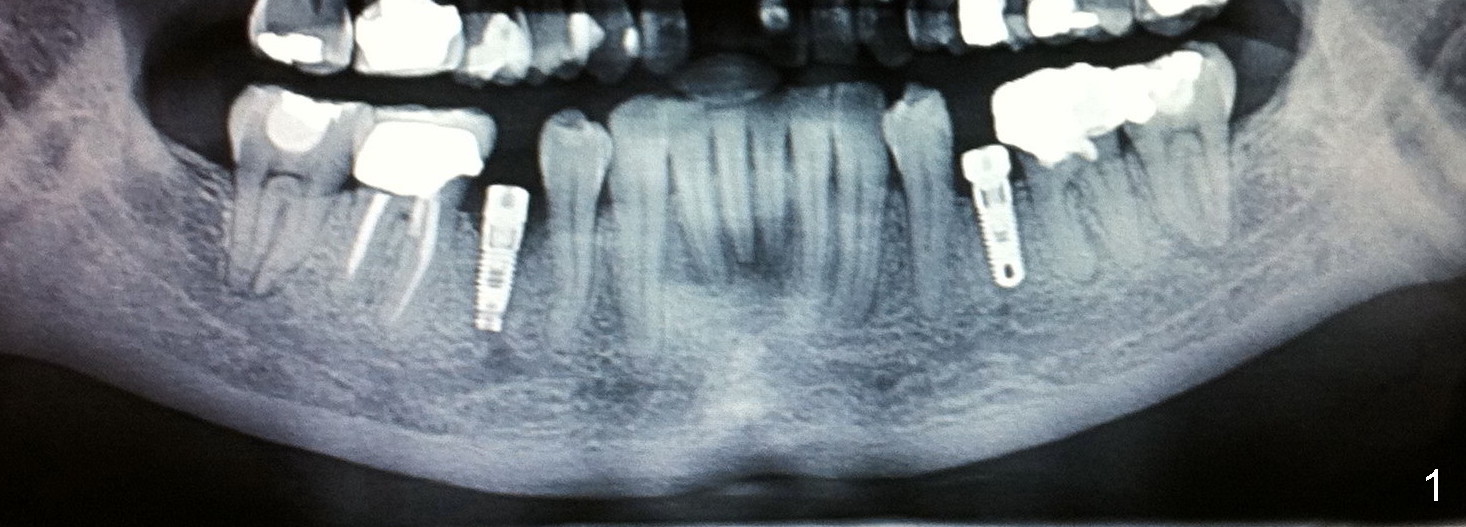
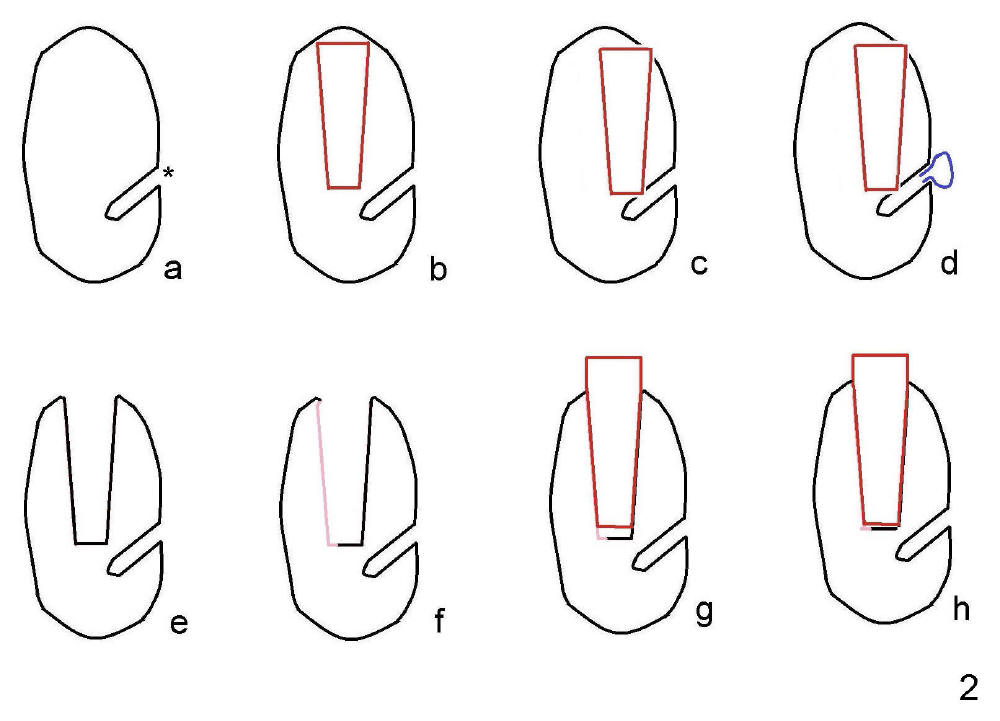
Fig.1 shows two implants placed at the sites of the lower 2nd premolars after multiple surgical procedures: extraction, soft and hard tissue graft. The patient experiences lower right lip paresthesia immediately post implantation and tenderness over the mental foramen 6 months postop. In my opinion, the depth and position of implant is difficult to control once the socket heals unless CT is taken every step of osteotomy. Fig.2 illustrates why and how immediate implant should be placed in anatomically challenging areas.
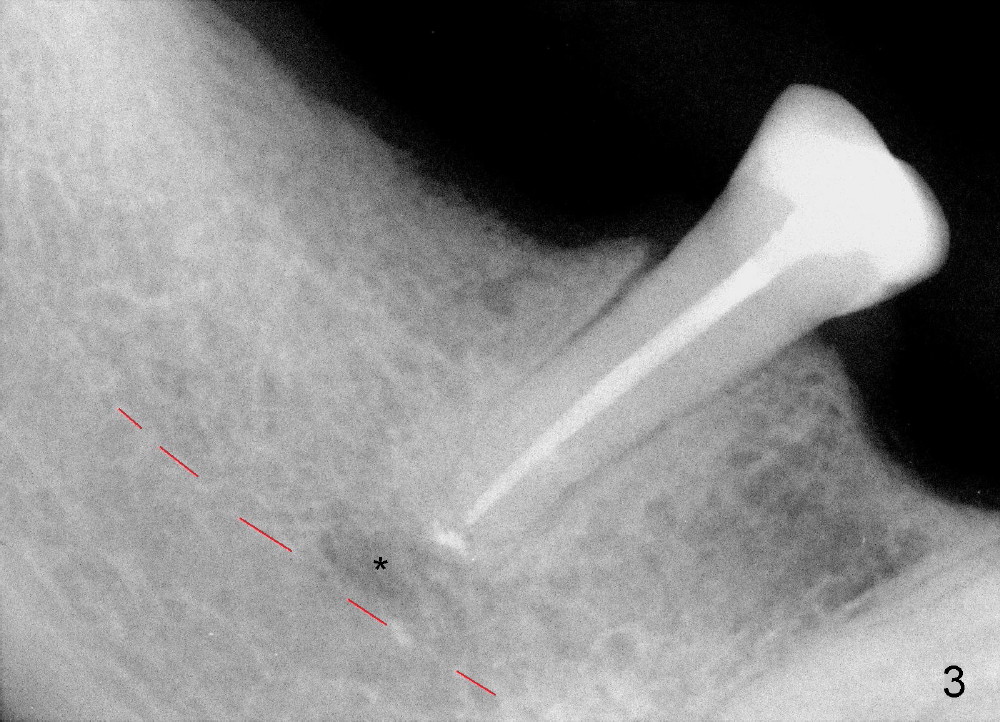
A 57-year-old lady has a lower partial. One of the abutments fractures (Fig.4). The apex is close to the presumably mental loop (Fig.3*; red dashed line: upper border of the inferior alveolar canal).
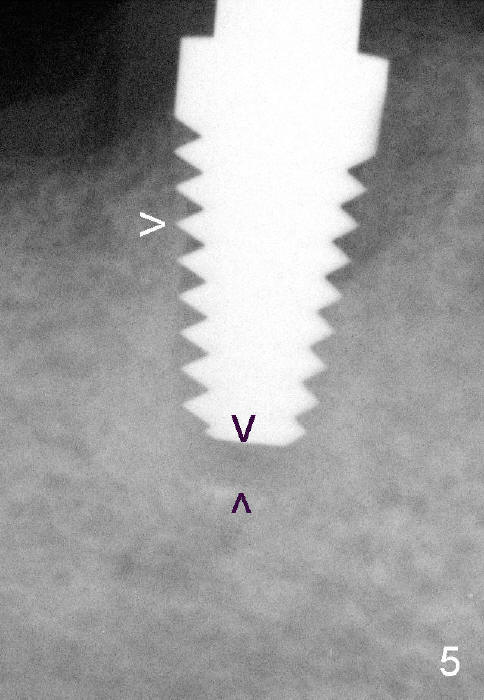
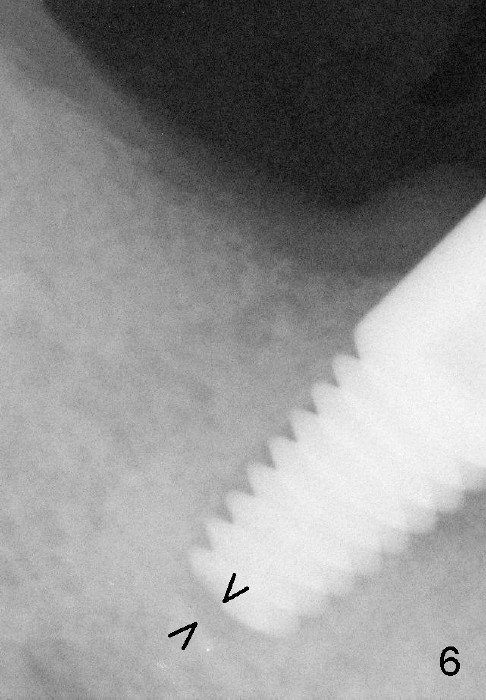
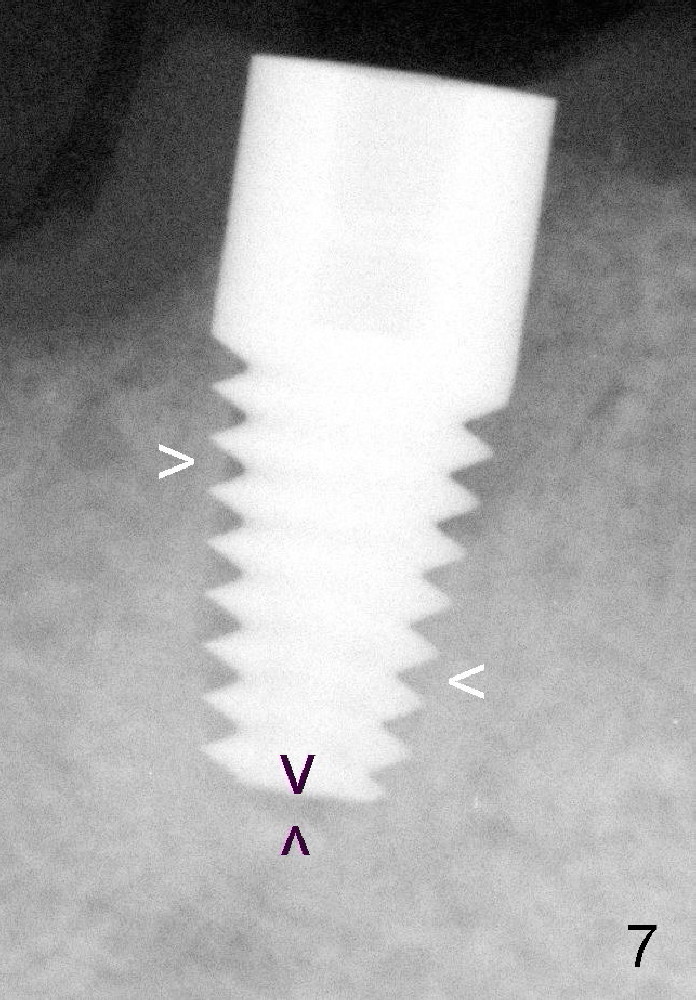
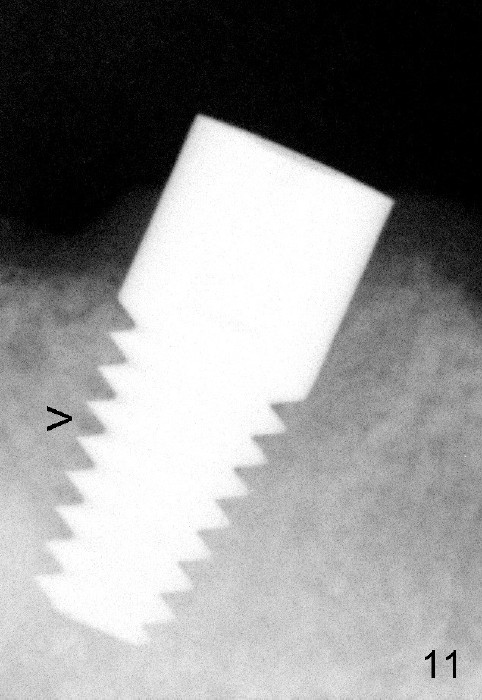
To be safe, immediate implant is planned to be confined to the socket. To achieve primary stability, the largest implant is to be used. The root of the extracted tooth is 5 mm mesiodistally and 6.5 mm buccolingually. The buccal plate is thin. Drills are used minimally, mainly lingually, whereas osteotomy is finished by taps. The first PA is taken when 6x14 mm tap is inserted (Fig.5). There is some distance between the tap and the bottom of the original socket (between black arrowheads). The tap is engaged to the wall of the socket (white arrowhead). The second PA is taken when 6x14 mm implant is initially inserted (Fig.6). There is still space to advance the implant (Fig.6 between black arrowheads). Fig.7 shows the final position of the implant. The implant threads are embedded into the bone (white arrowheads). The insertion torque is over 60 Ncm. When the partial is placed, the implant does not look to be over engineered. There is no sign or symptom of paresthesia or infection (Fig.9, 9 days postop). The gingiva is healthy around the implant 4 months postop (Fig.10). The bone has grown more into the threads of the implant (Fig.11 >, compare to Fig.7).
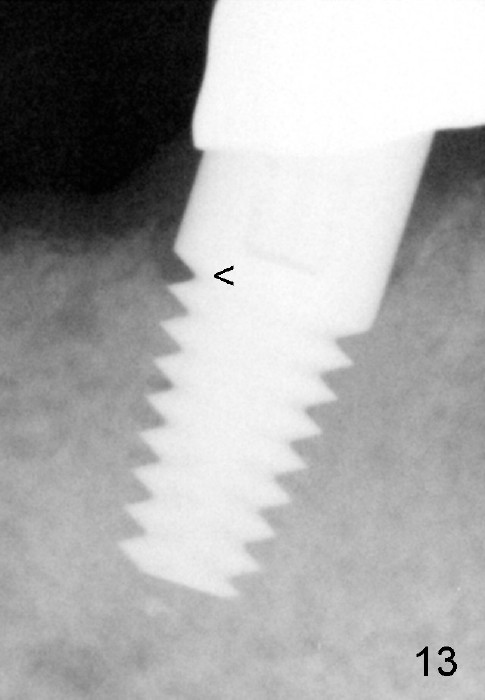
Fig.12,13 show the implant crown in function for 7 months, while Fig.14,15 for 16 months post cementation. In fact, a new RPD has been fabricated with clasp and I-bar (Fig.15 *, as compared to Fig.8,12).
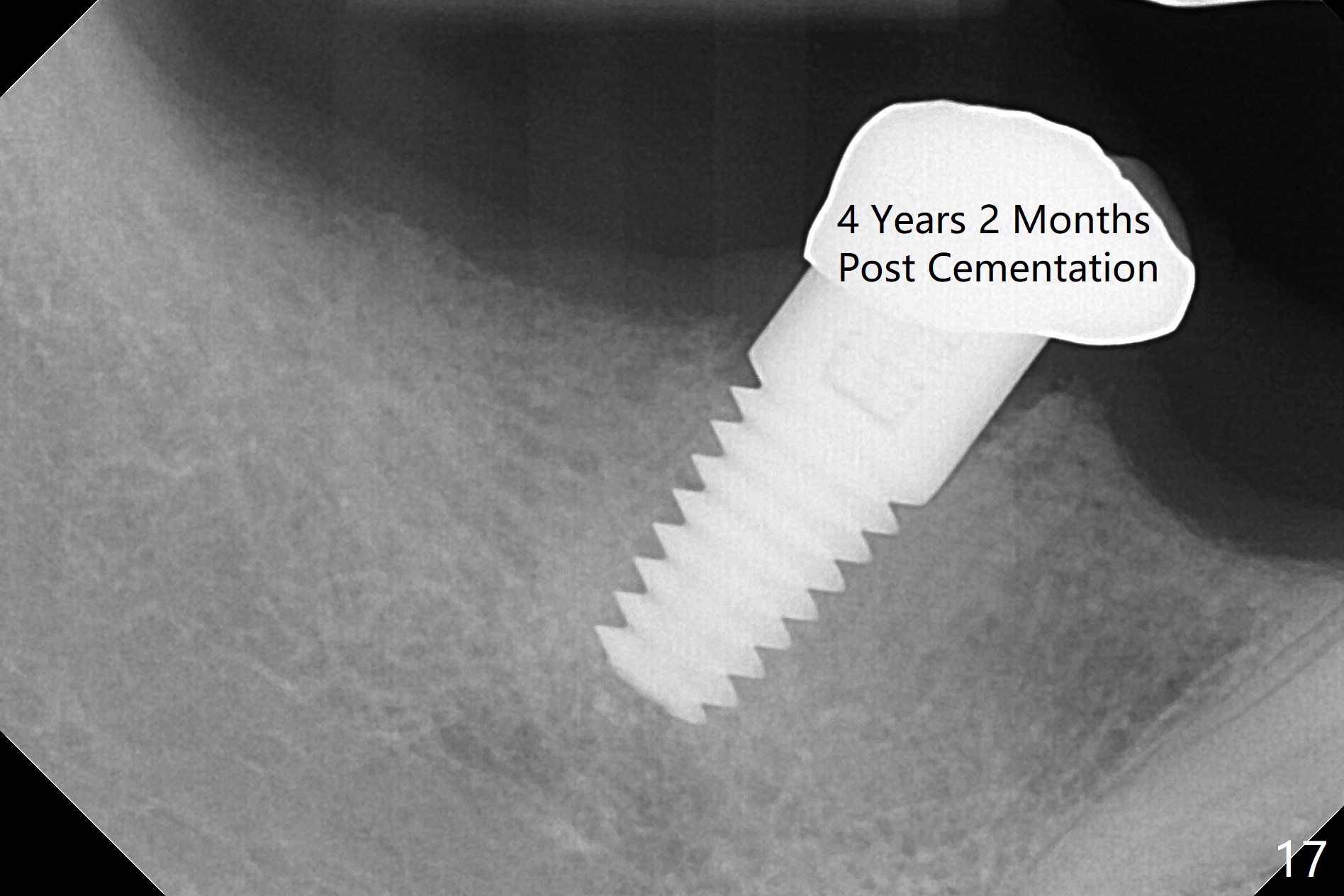
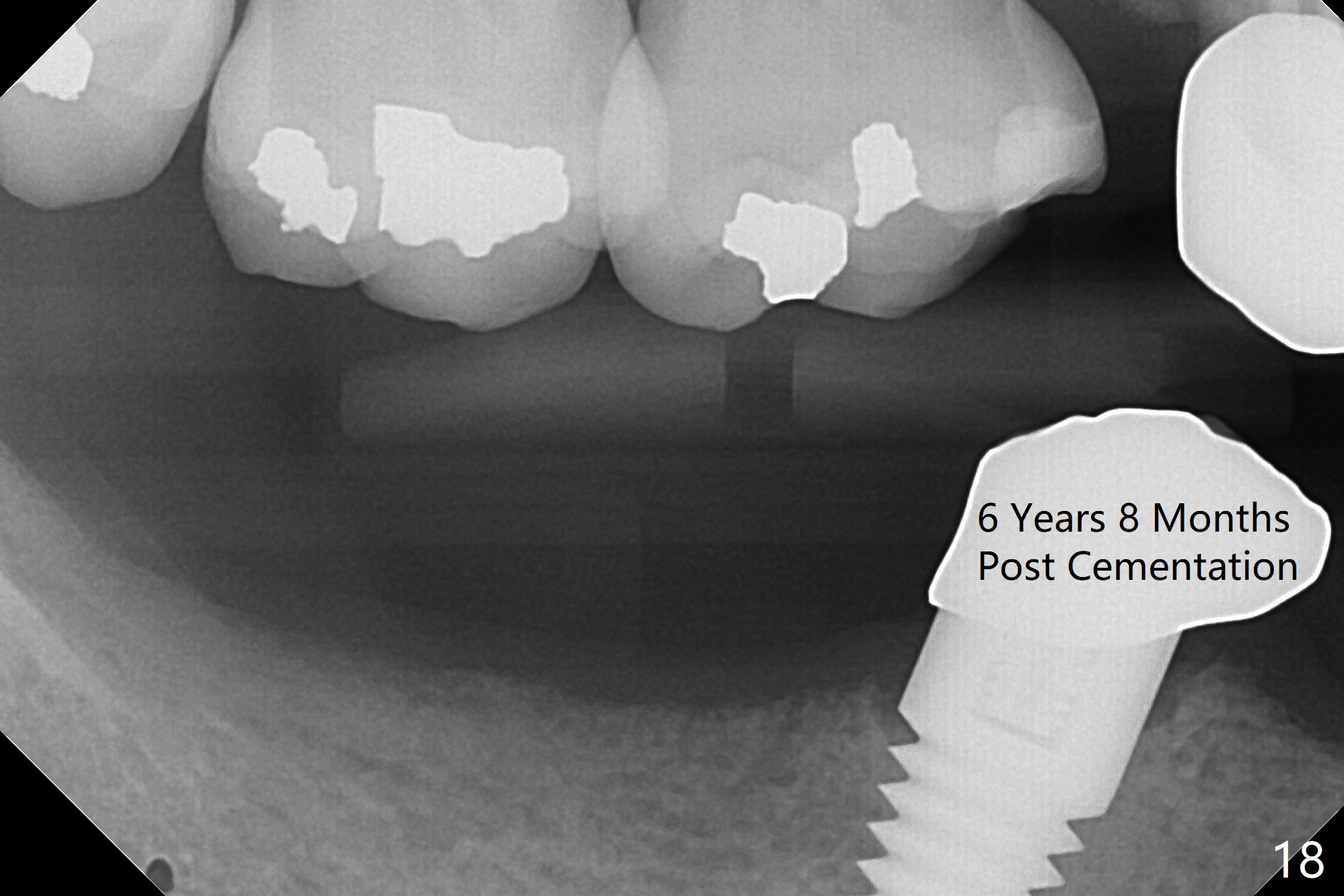
Panoramic X-ray taken 9 months post cementation shows the clearance from the Mental Loop (Fig.16). Although no drill technique is safe for the neurovascular bundle, the implant tends to deviate buccal, causing mental show through. It is still safe to make lingual osteotomy for a few millimeter and place a smaller implant (<4.5 mm). There is no bone loss 4 years 2 months post cementation (Fig.17) or 6 years 8 months post cementation (Fig.18).
Immediate Implant Safety Issues, Immediate Implants for Lower Bicuspids, Introduction to Immediate Implant #13 7
Xin Wei, DDS, PhD, MS 1st edition 11/24/2013, last revision 12/12/2020