

|
|
|
|
|
|
|
|
|
|
|
|
|
|
Immediate Implant Placed in the Buccal Sockets of an Upper Molar
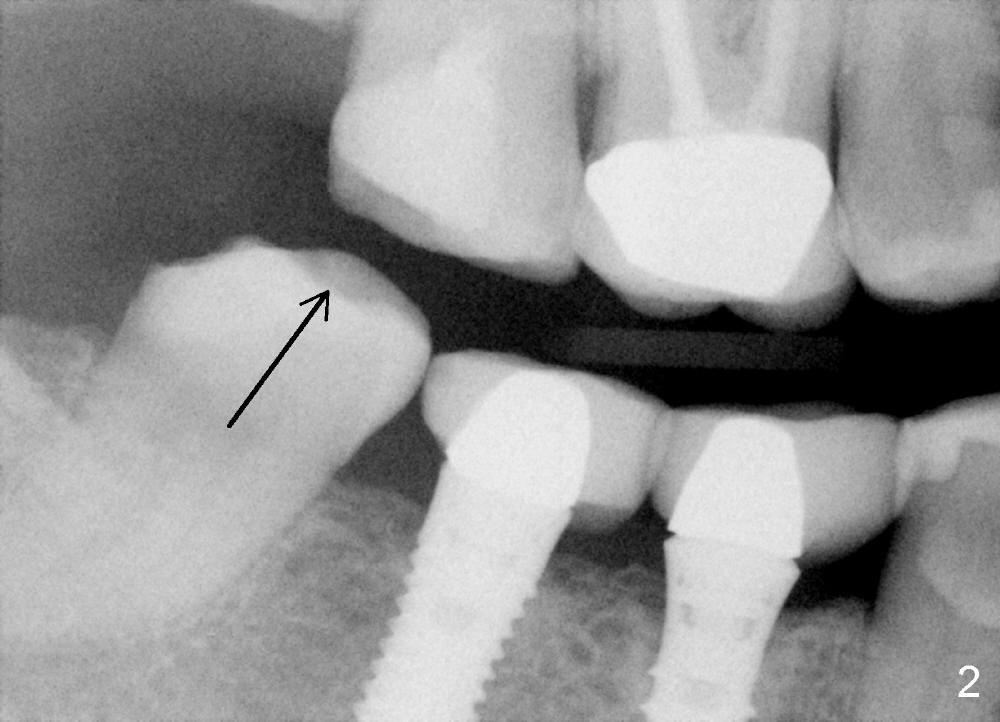
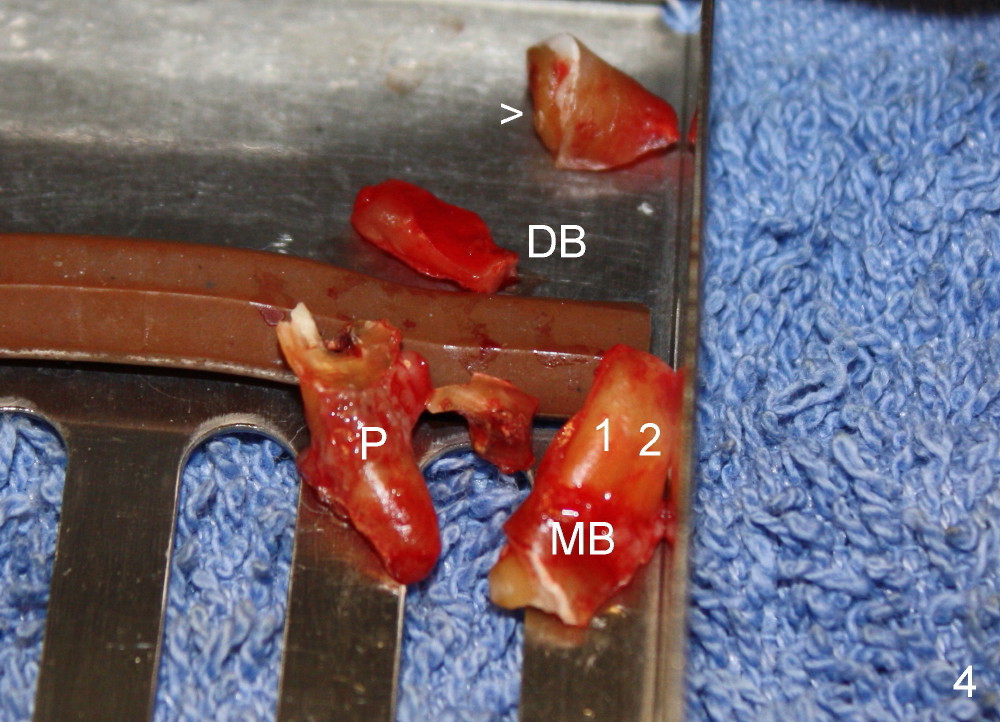
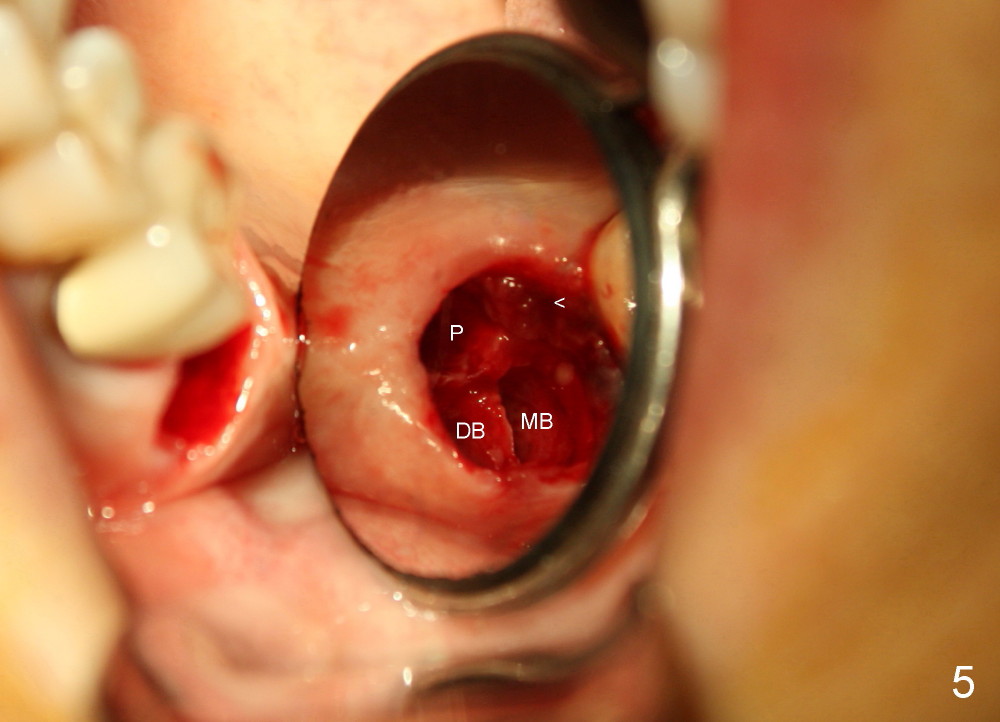
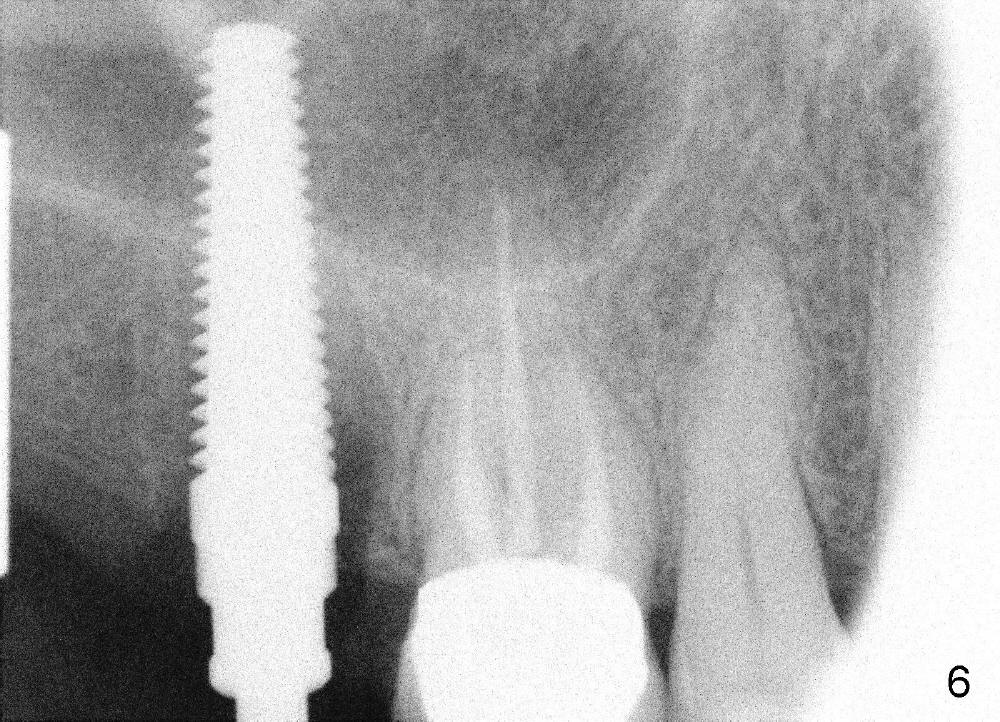
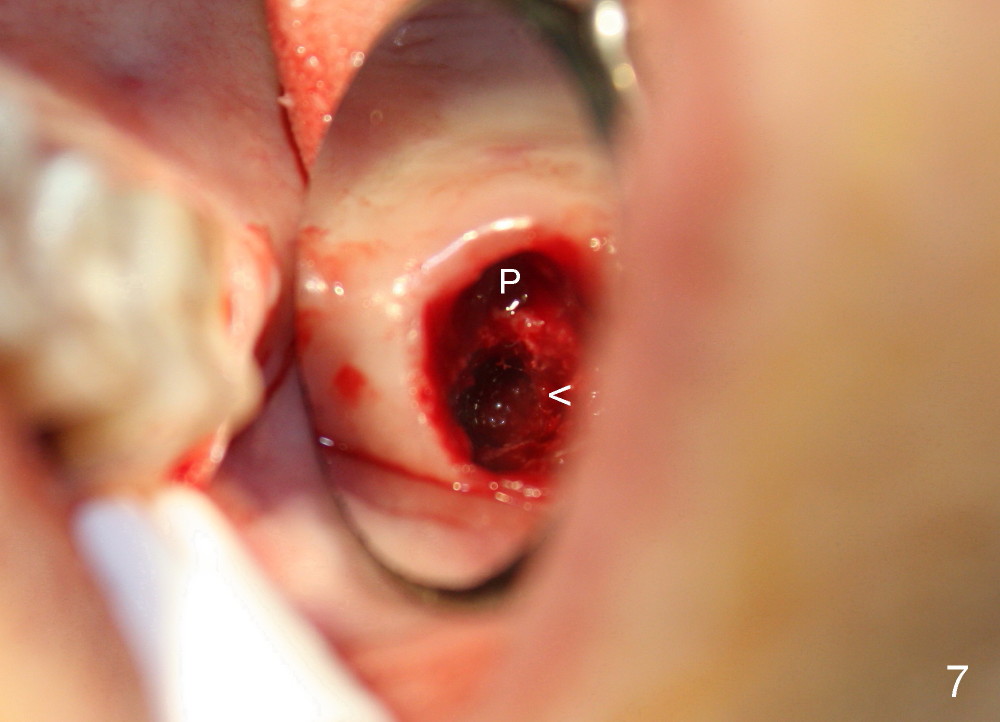
A 51-year-old lady has multiple restorations (Fig.1-3), e.g., amalgam (A in Fig.1) of the upper right 2nd molar as well as history of pulpotomy. The 1st molar has periapical radiolucency (* in Fig.1) and needs root canal therapy. The lower 3rd molar occludes (Fig.2 arrow) with the upper 2nd molar. The latter fractures subgingivally (Fig.3 <) and is extracted with a large MB root (Fig.4) and MB socket (Fig.5). The gingival one third of the palatal wall is defective, as indirectly indicated by granulation tissue palatally (Fig.5 <). So the osteotomy for the immediate implant will not be placed in the palatal socket. The septum is pointed coronally. The pointed portion of the septum is removed; initial osteotomy is formed by 1.5 mm pilot drill in the septum, followed by 2-5 mm osteotomes with the depth of 17 mm. The enlarging osteotomy is deviating buccally; drills are being used to move the osteoomy palatally without much success. When a 5 mm tap is inserted, it is stable and appears to be inside the maxillary sinus (Fig.6). In fact the osteotomy has bony walls around (Fig.7 <), including apical, when the tap is removed. Preop PA shows that the palatal root is apical to the sinus floor (Fig.1 between arrows).
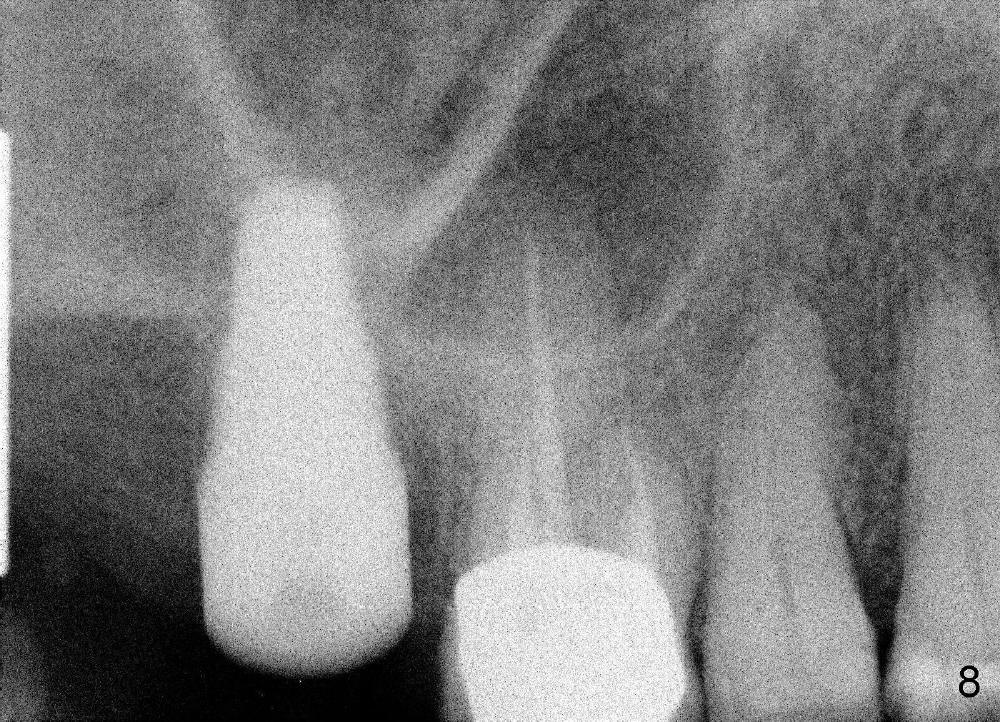
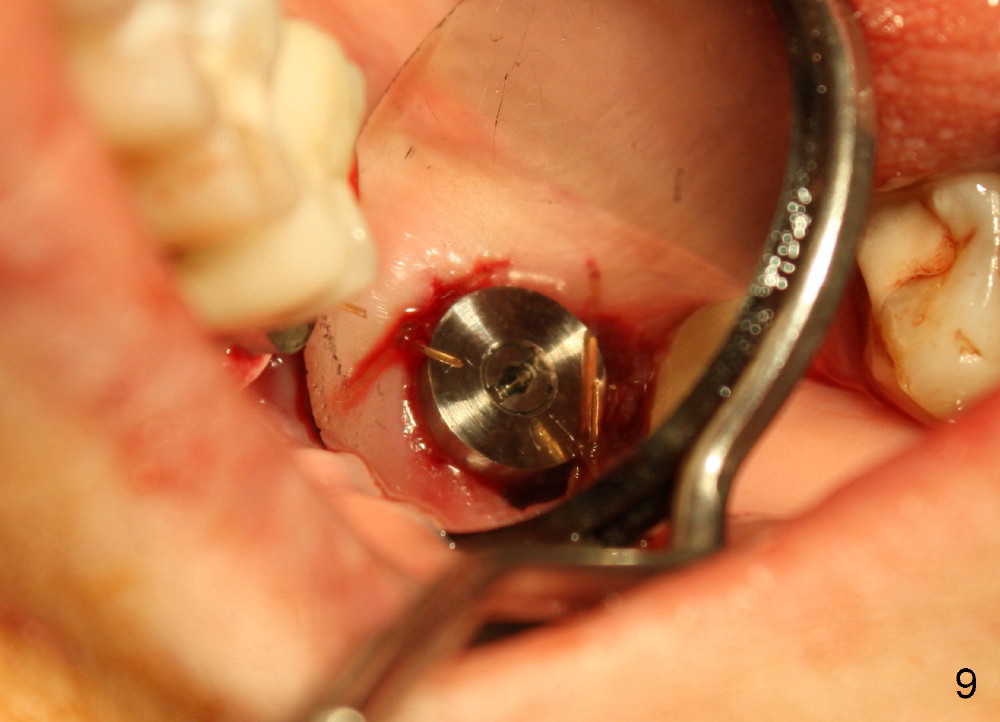
Although the osteotomy appears mainly located in the buccal aspect of the socket apically, the implant (7x17 mm, Fig.8) is placed more or less in the middle of the socket (Fig.9). The trick is to lean the implant palatally while it is being inserted.
Fig.10 shows the implant 5.5 months postop with apparently bone growth in the former mesiobuccal socket (*). The implant is stable with healthy gingiva around it.
Xin Wei, DDS, PhD, MS 1st edition 11/22/2013, last revision 09/08/2014