
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Septum Expansion
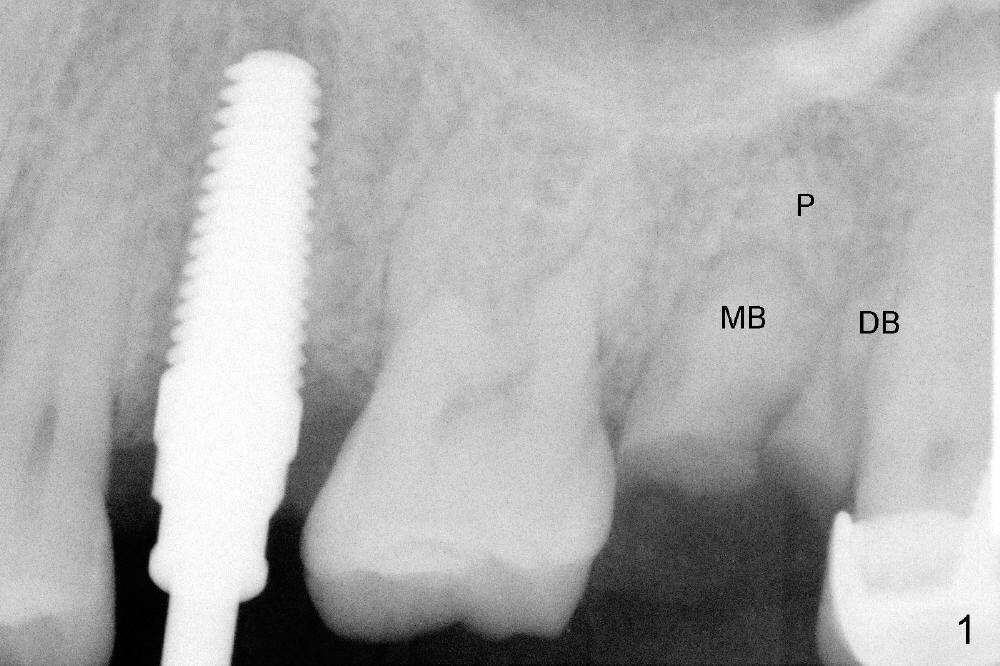
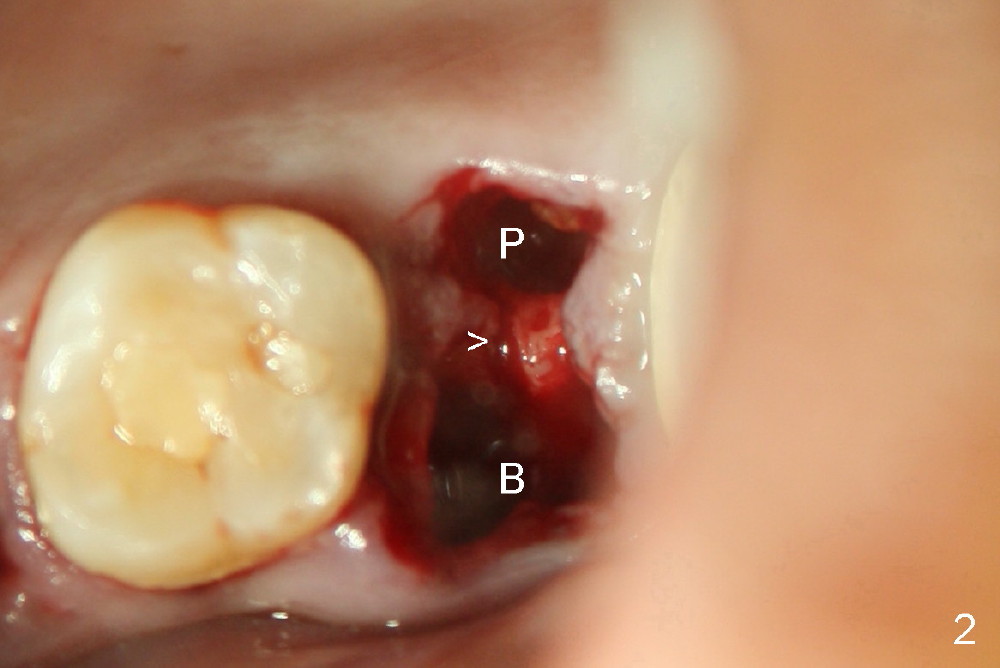
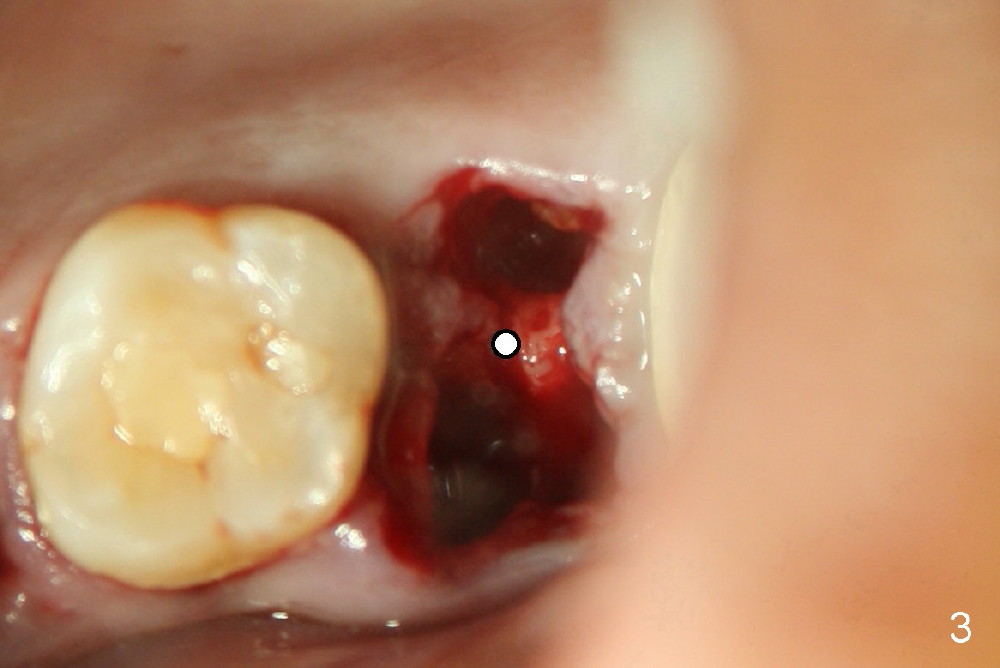
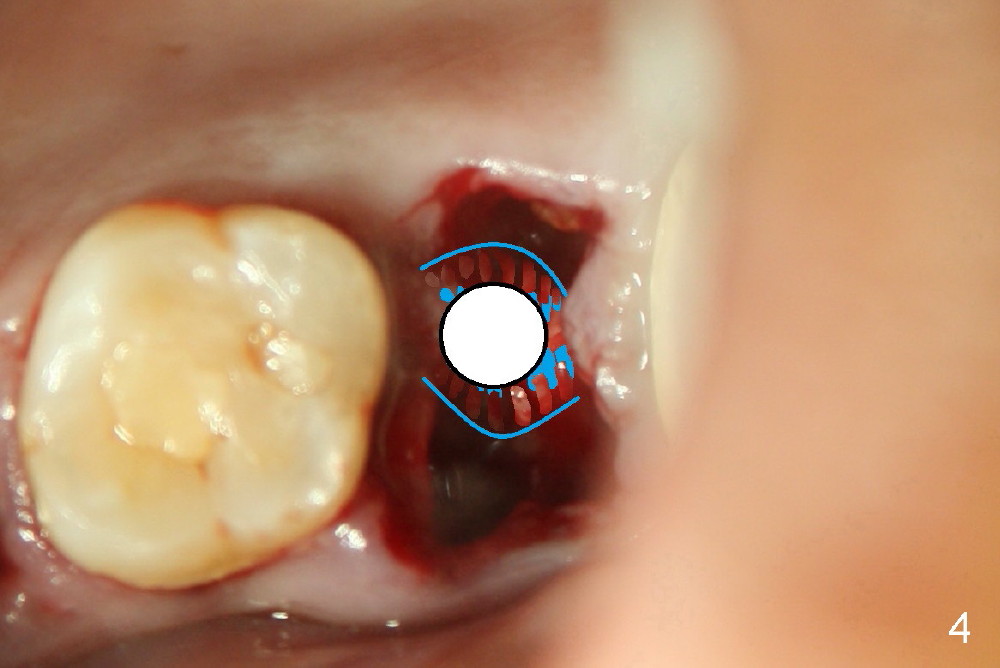
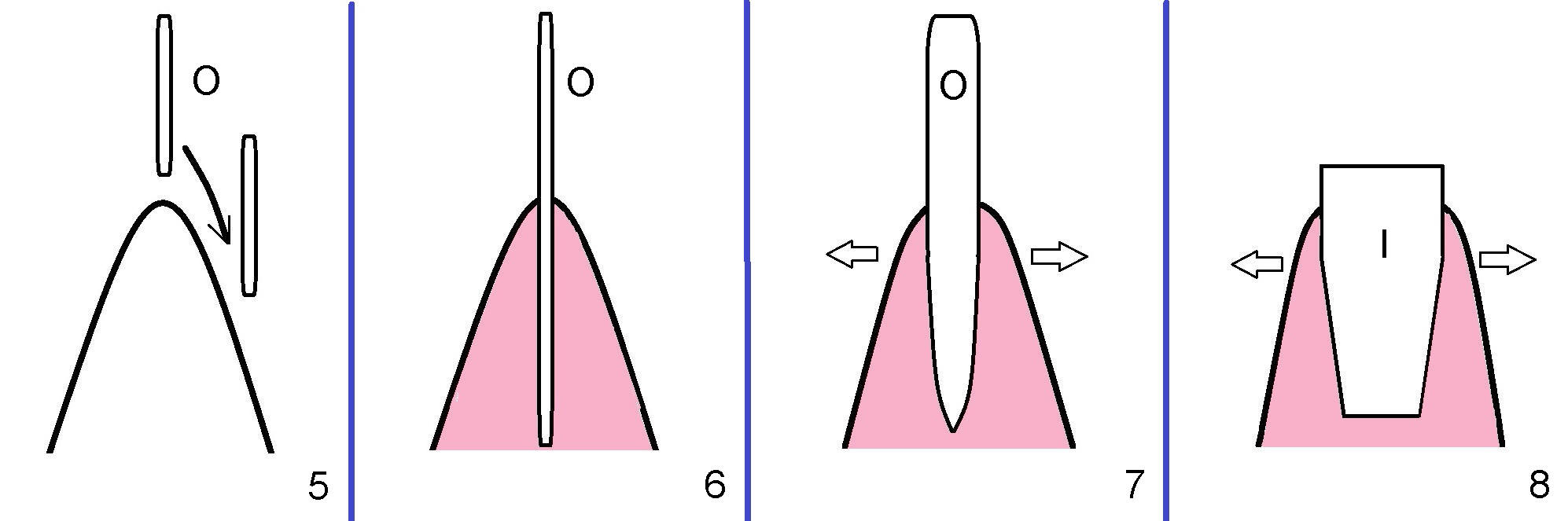
A 43-year-old lady has multiple nonsalvageable teeth. The first surgery involves two immediate implants in the upper left sextant (Fig.1: #13 and 15). The tooth #15 has 3 residual roots (MB, DB, P). There is no septum left between the first two roots when the tooth is extracted. A septum exists between the palatal (P) and buccal (B) sockets (Fig.2). Bone expansion technique is utilized to create an osteotomy in the septum. However, the smallest rounded tapered osteotome cannot be driven into the narrow septum; it slides (Fig.5). To get an initial engagement, a slot is created by high-speed surgical handpiece and fissure bur on the top of the septum. A series of blade-like osteotomes are inserted into the septum for sectioning (Fig.2 >). The smallest rounded osteotome is now easy to be inserted into the middle of the septum (Fig.3 circle, Fig.6 O). The septum is expanded by larger osteotomes (Fig.4 white circle; Fig.7 O) and tap (Fig.9 T). The septum continues being expanded when a 6x14 mm implant is placed (Fig.8,10 I). The insertion torque is more than 60 Ncm. No bone graft is placed. The palatal gap is closed by a palatal flap.
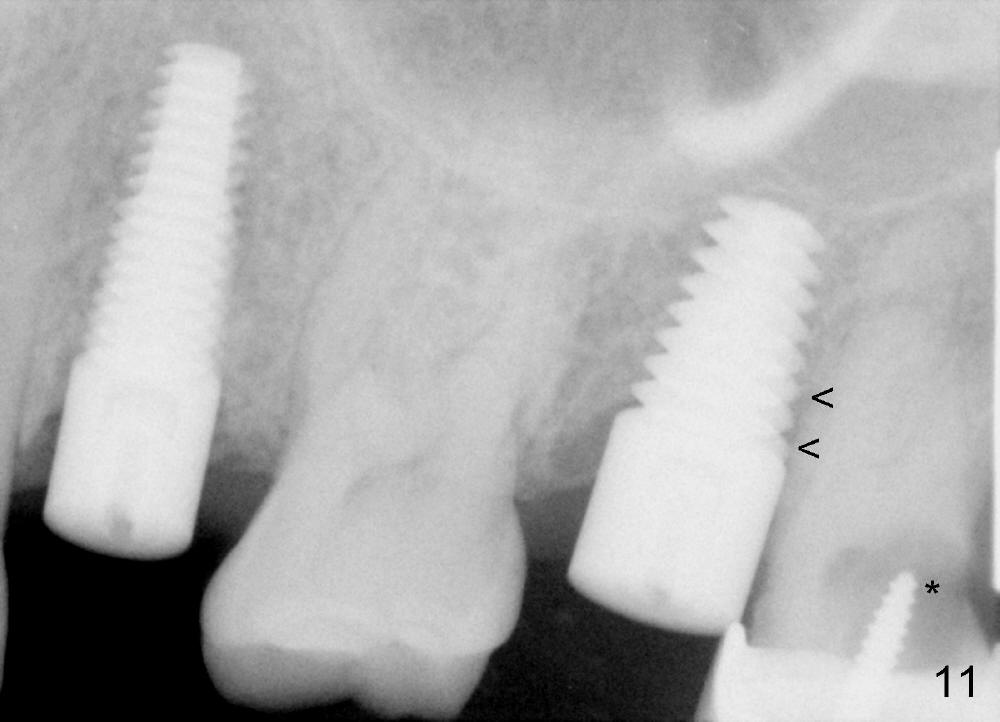
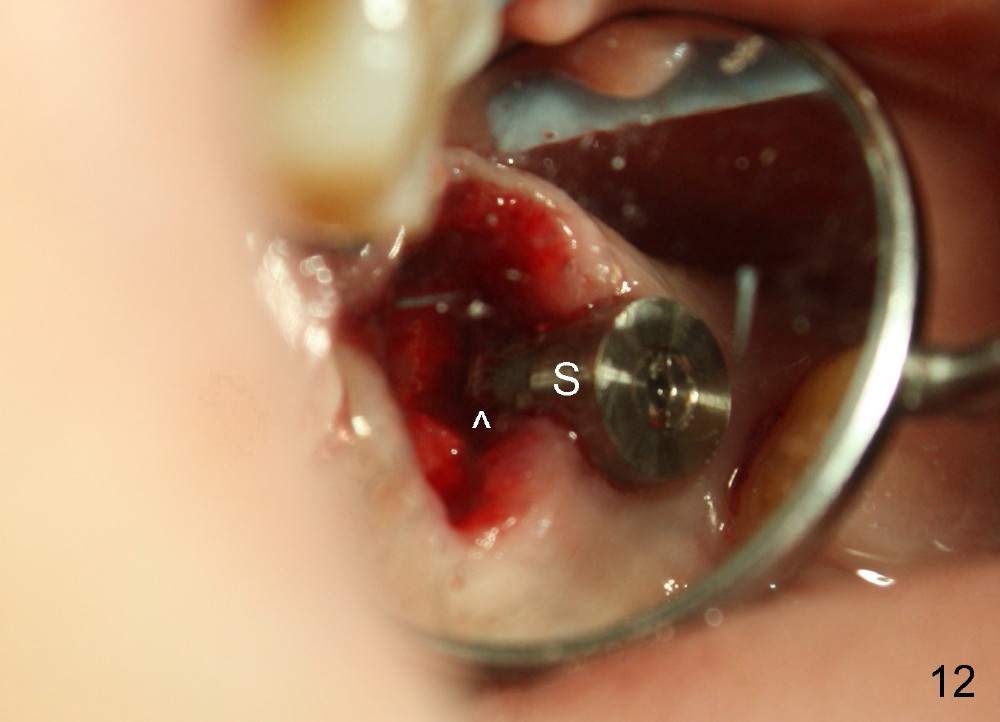
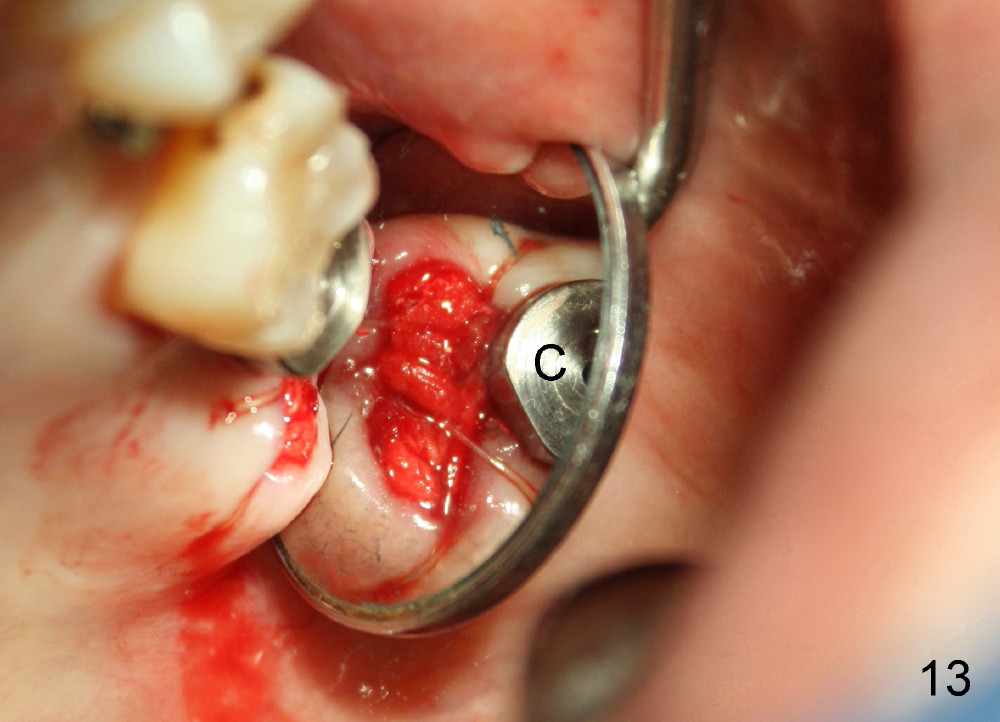
Postop, the patient has a car accident. She does not return for followup until 11 months later. The implant is stable. The neighboring third molar has caries (Fig.11 *). When it is extracted, the distal threads of the implant are found to be exposed (apical to ^ in Fig.12). A synthetic bone graft is placed to cover the exposed threads, followed by insertion of a collagen plug (Fig.13).
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 05/17/2013, last revision 05/01/2014