


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
||||
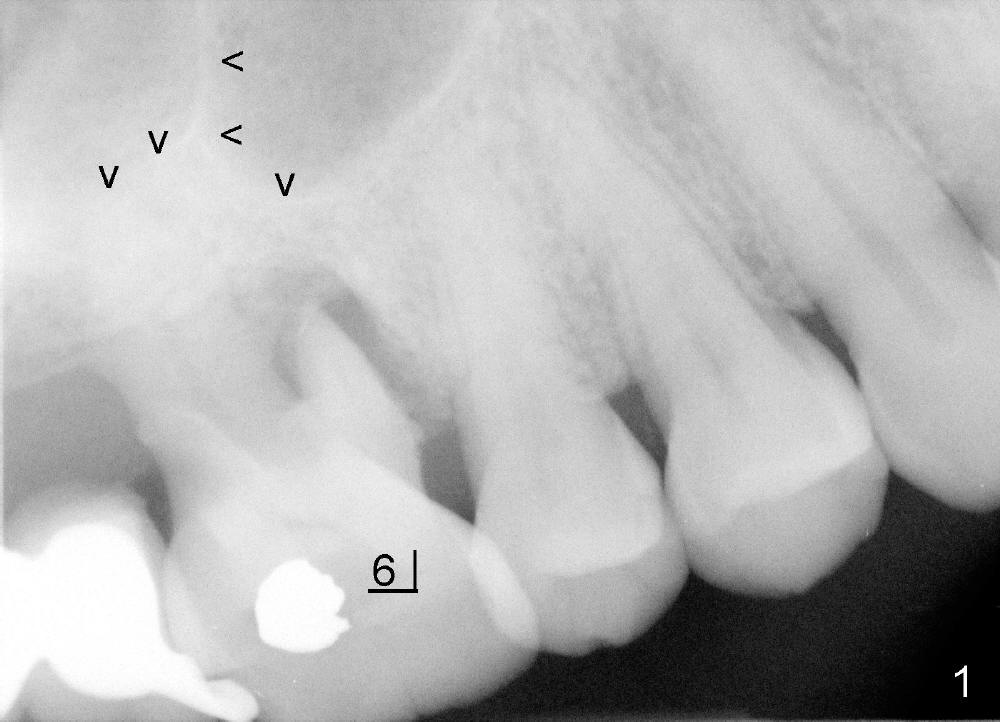
Sinus Septum for Primary Stability of Implant
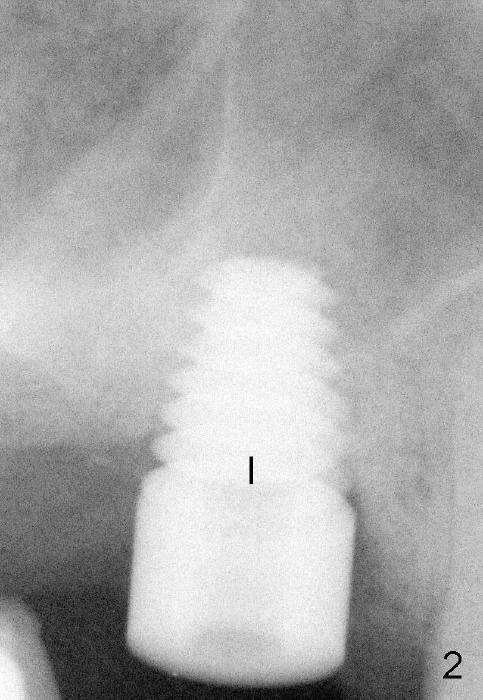
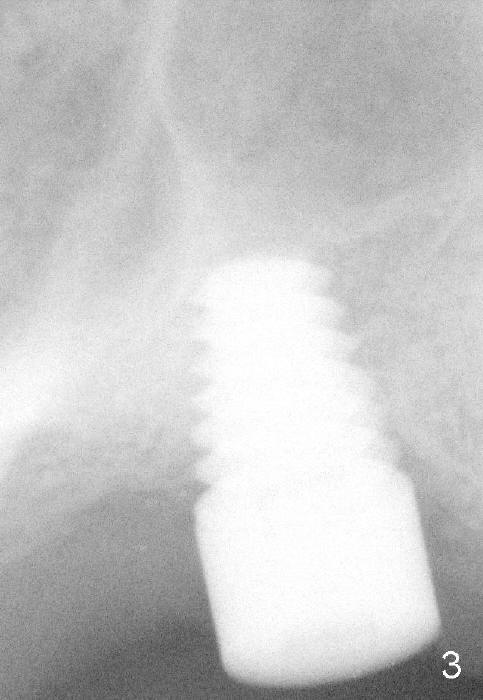
The upper right 1st molar of Mrs Chen has endo/perio disease (Fig.1). The bone height is limited (~ 3mm), but there is a sinus septum above (arrowheads). Approximately 4 months post extraction, a 6x11 mm implant is placed with insertion torque >60 Ncm, partially due to engagement into the sinus septum (Fig.2). There is apparent osteointegration 3 months postop (Fig.3).
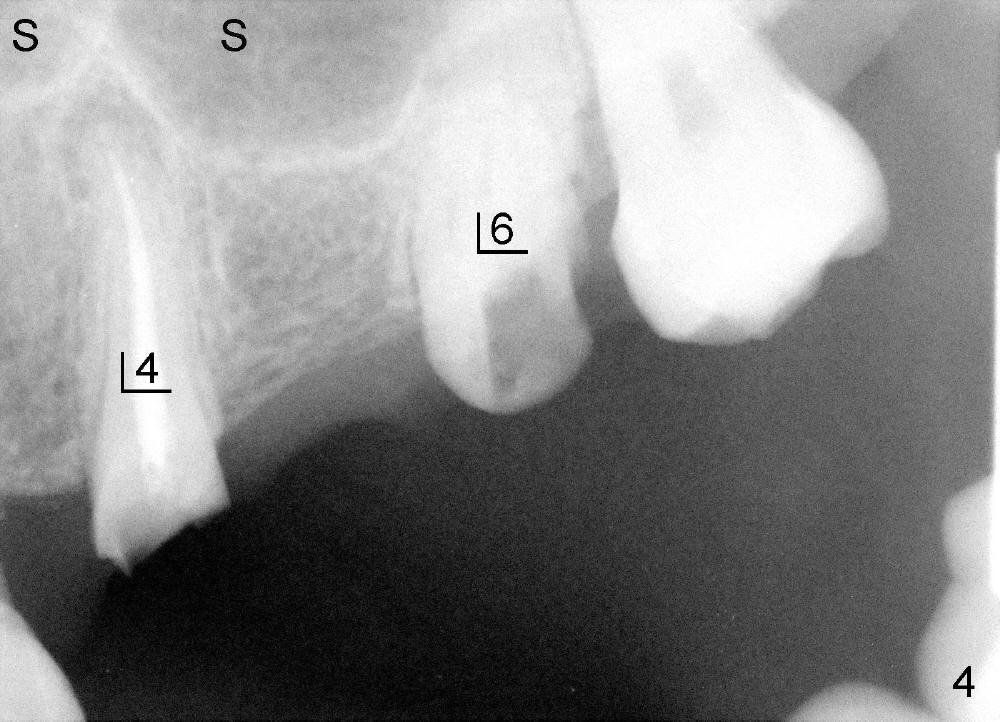
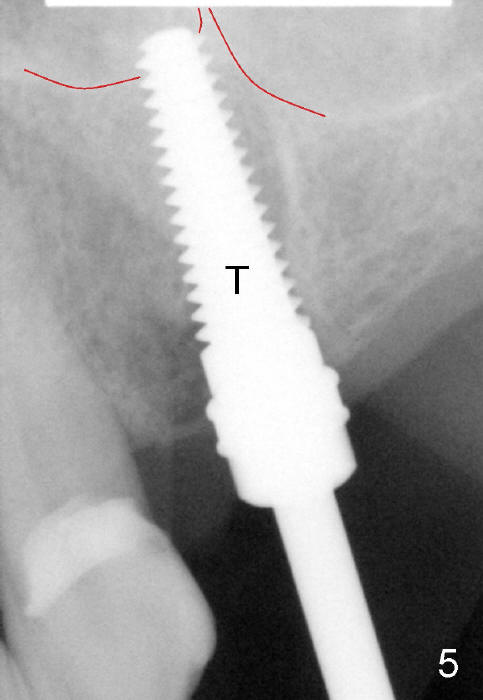
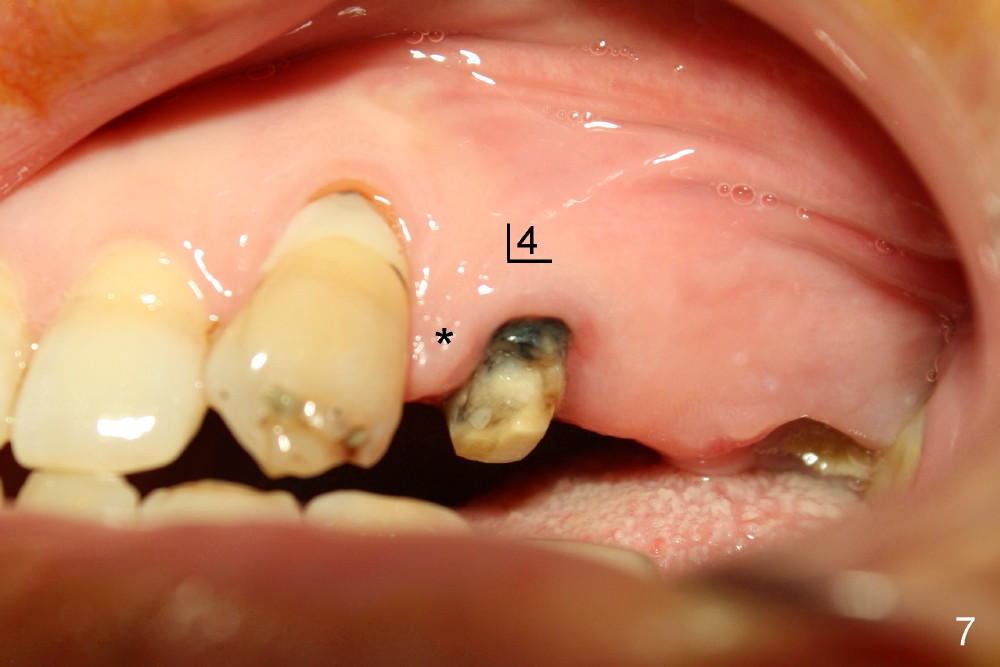
A 47-year-old lady has lost an upper left bridge (Fig.4,7). She is a dental phobic, but is concerned about cosmetics. Immediate implant and immediate provisional for the 1st bicuspid are easily accepted. There is a sinus septum above. Intraop PAs show that 4.5x17 mm tap (Fig.5) and 5x17 mm implant (Fig.6, insertion torque > 60 Ncm) are placed mesial to the septum without sinus membrane perforation. An abutment is placed immediately and an immediate provisional is fabricated.
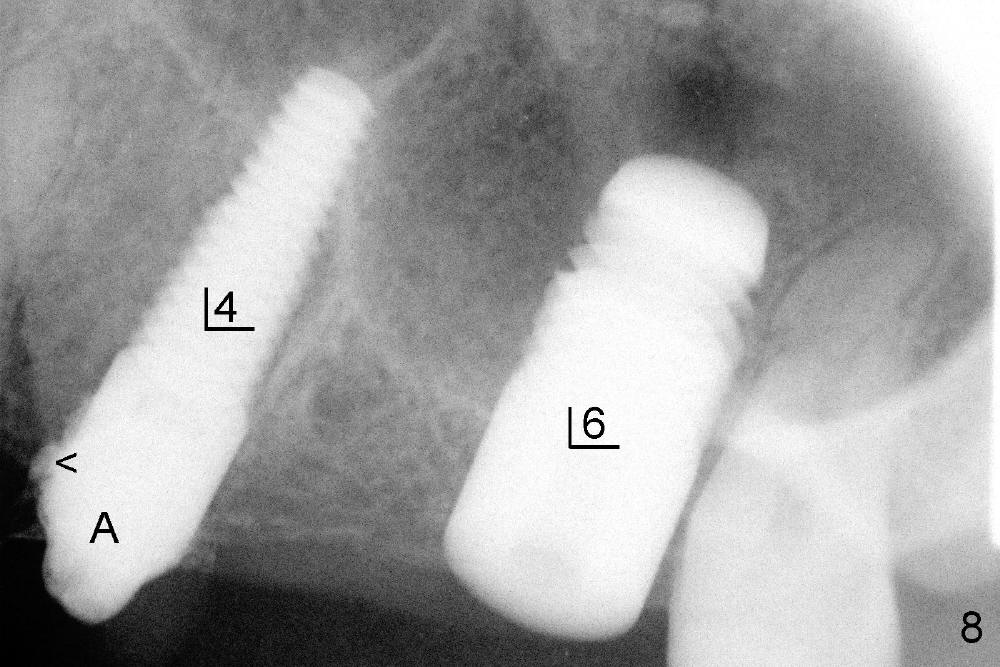
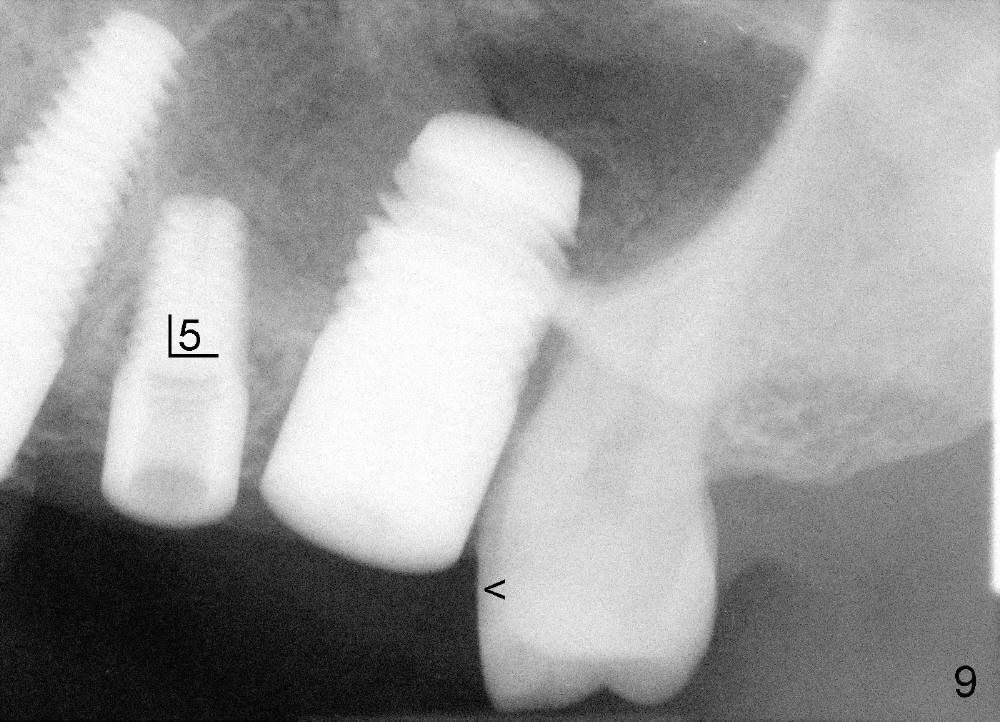
An immediate implant was tried at the site of the 1st molar without success 2 weeks earlier. One month after 1st try, a 7x14 mm cylindrical implant is placed (Fig.8). There is a space issue: the mesial surface of the 2nd molar has to be trimmed in order to place the large implant at the 1st molar (Fig.9). A 4.5x11 mm tapered implant is placed at the 2nd bicuspid at the same apppointment (Fig.9). Both implants have barely enough primary stability. No immediate provisionals are fabricated. In fact there should no problem doing so, considering 3 neighboring implants. Splinting can compensate for lack of primary stability in 1 or 2 implants.
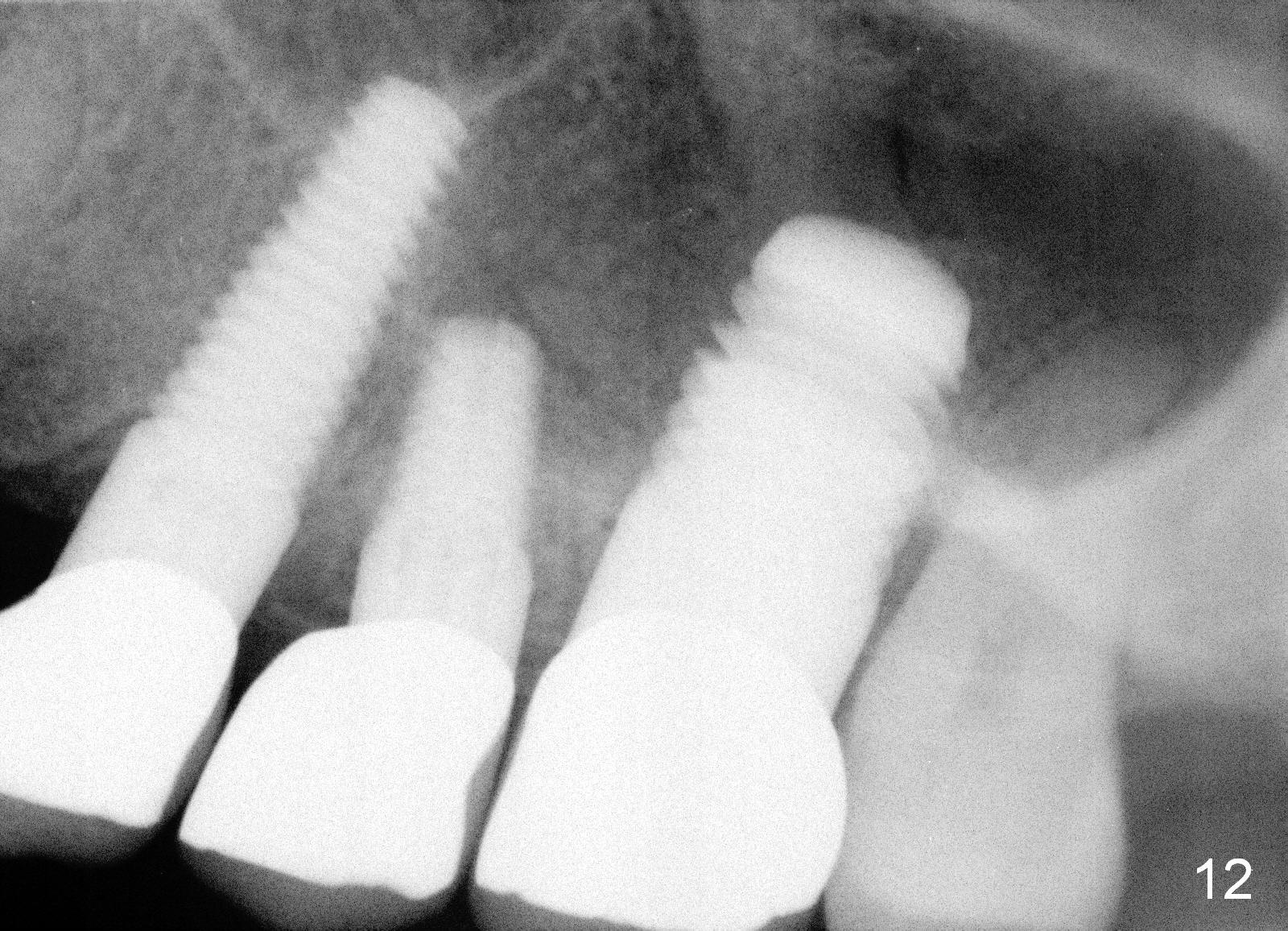
Anyway, three of the implants heal normally 3 months postop (Fig.10) and restore together. Fig.11 and 12 are taken 11 and 21 months post cementation.
It appears that the sinus septum helps increase primary stability.
Return to Upper Bicuspid Immediate Implant, Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 06/23/2013, last revision 08/09/2015