






|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|
||
|
|
|||||
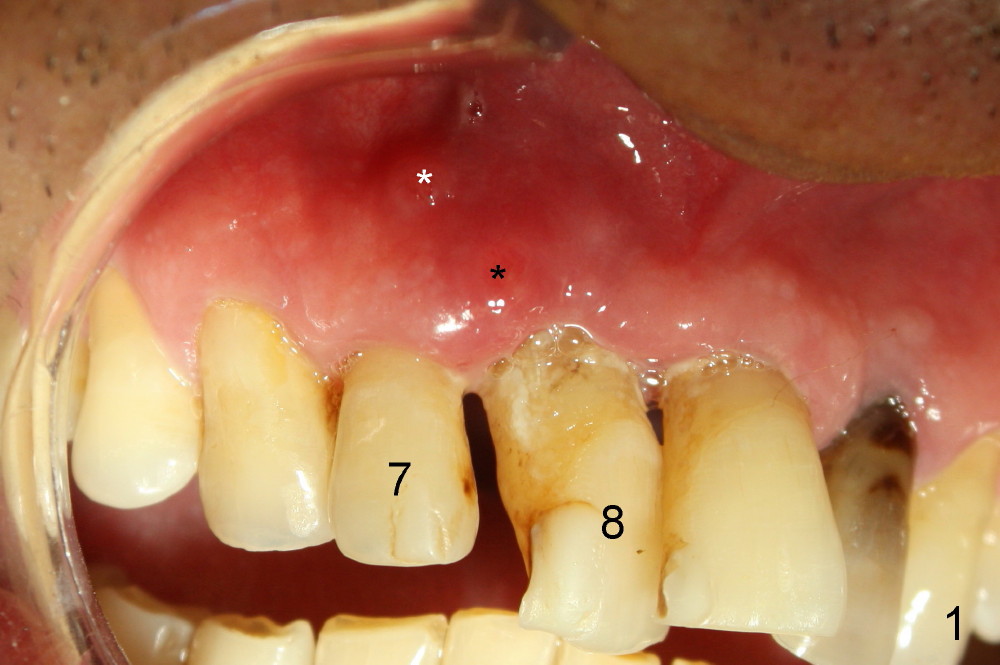
Immediate One-Piece Implant between an Infected Lateral and the Incisive Canal
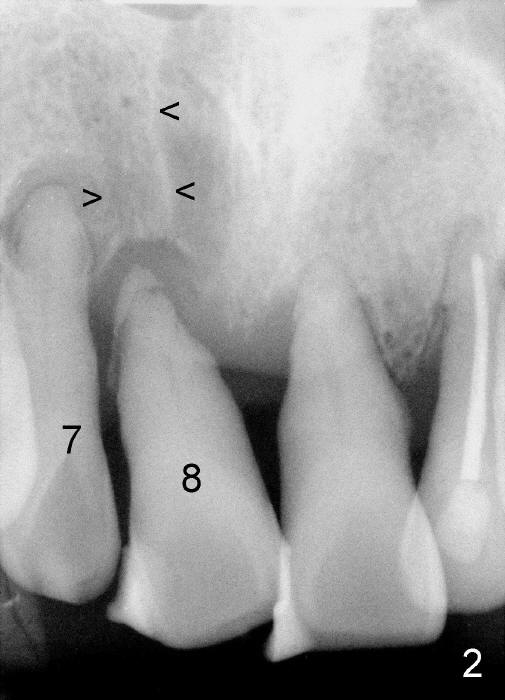
A 64-year-old man has had two episodes of trauma to his upper incisors with different degrees of mobility (Fig.1,2). He chooses implants, but his finance is limited. The tooth #8 is most mobile, but there is limited mesiodistal width of bone (between Fig.2 arrowheads) available for implant placement. Mesial is a large incisive canal and distal apical radiolucency of the lateral incisor (#7). Ideally root canal therapy (RCT) should be conducted for the lateral prior to implant placement at the site of #8.
We choose to extract #8 with immediate implant first. If the implant placement compromises the root of the #7, the latter will be extracted as well with immediate implant.
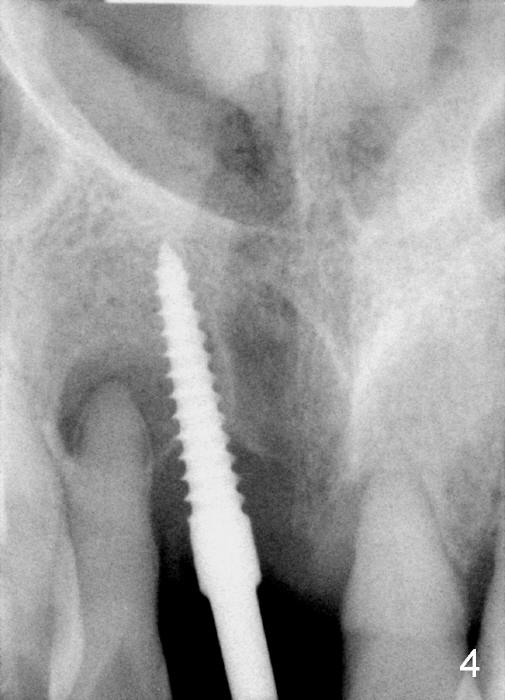
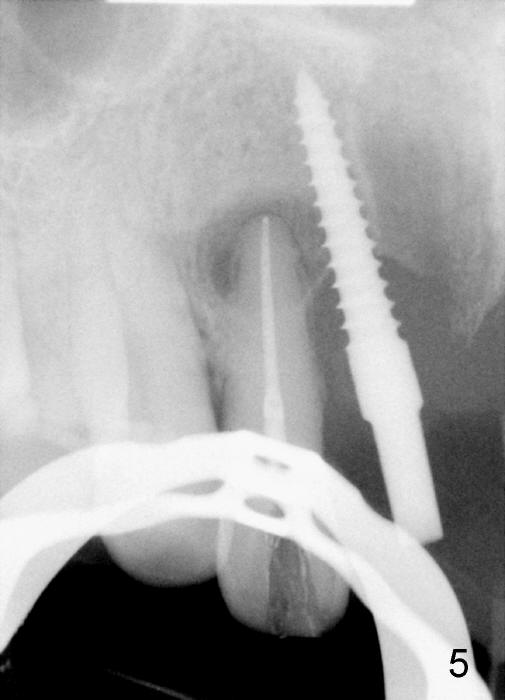
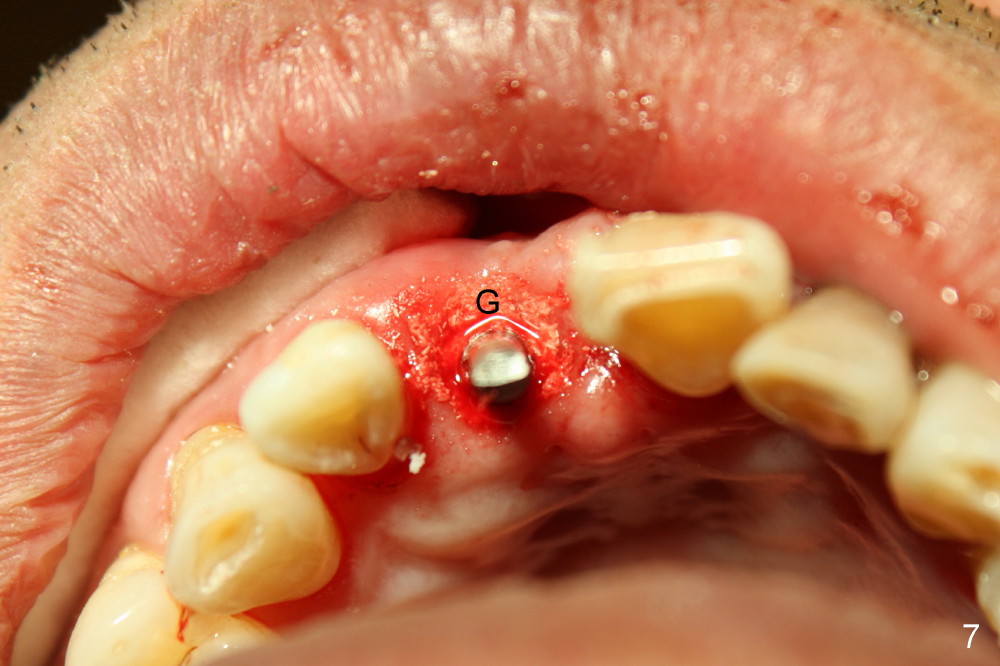
Fortunately, the trajectory of the initial osteotomy for #8 (Fig.3) needs minor adjustment before placing an angled (15º) 3x17 mm one-piece implant (Fig.4 with insertion torque 40/45 Ncm). RCT is then carried out for #7 (Fig.5). The two abscesses associated with #7 and 8 are reduced immediately following the treatments (Fig.6, as compared to * in Fig.1). The gap buccal to the implant is filled with allograft (Fig.7 G) before placement of an immediate provisional. The patient returns 6 days postop and has the provisional modified (Fig.8-11). He is pleased with the outcome. He says "one implant makes three teeth stable".
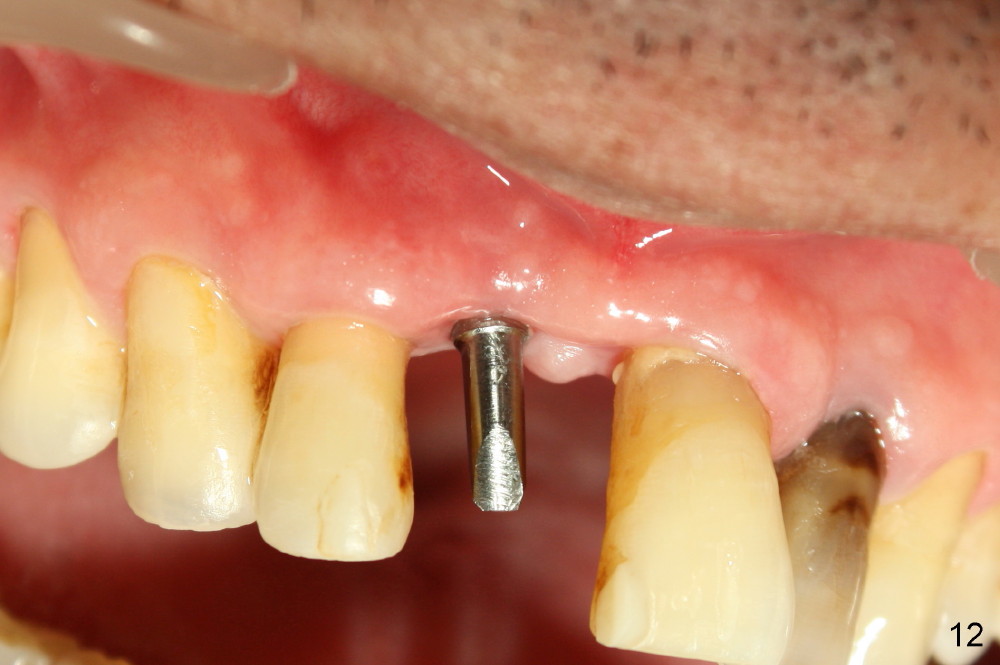
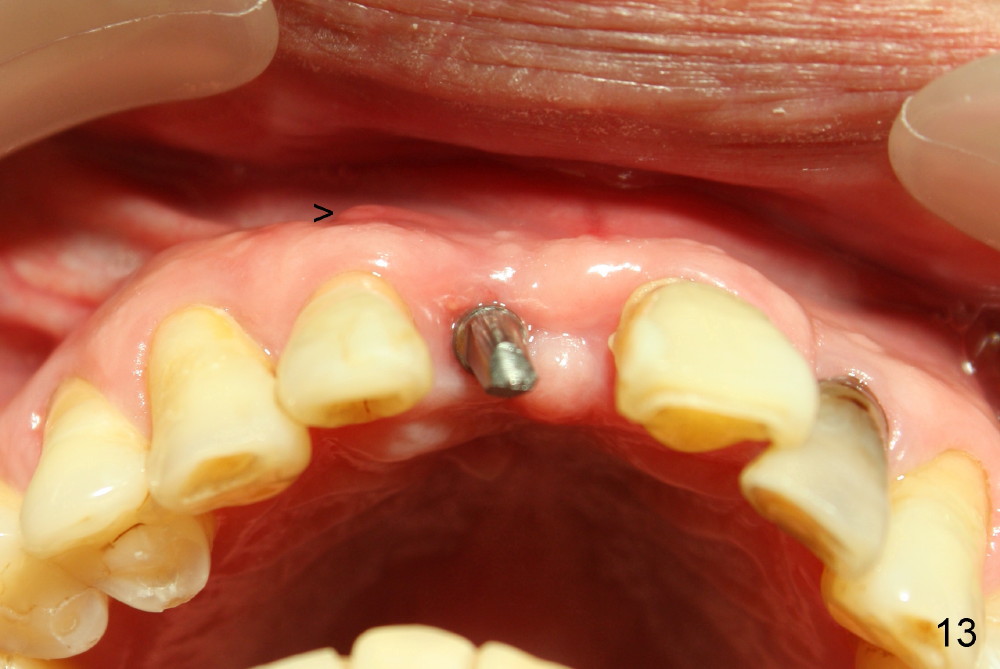
The patient returns because of dislodgement of the provisional less than 4 months postop (Fig.12). In spite of placement of a small (3 mm one piece) implant, there is no buccal atrophy (Fig.13). Distally, bone has grown to cover the 3rd thread of the implant (Fig.14: #3, as compared to 4), while the bone has apparently deposited in the mesial threads of the implant (*).
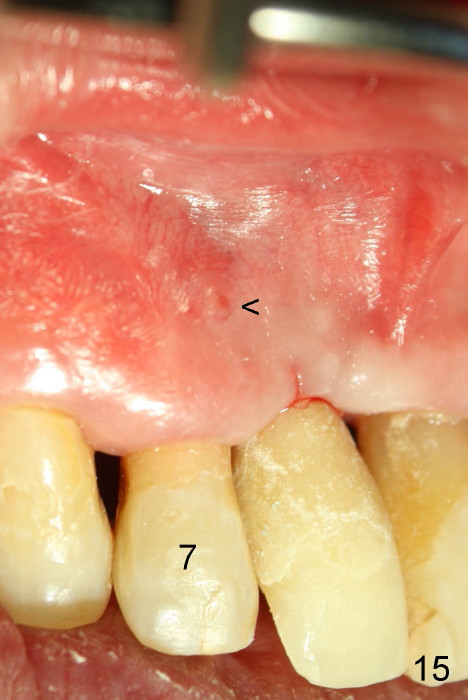
The periapical radiolucency of #7 has not disappeared (Fig.14), associated with persistence of the fistula (Fig.13,15 <). Apicoectomy with bone graft is planned before the definitive crown is cemented at the site of #8.
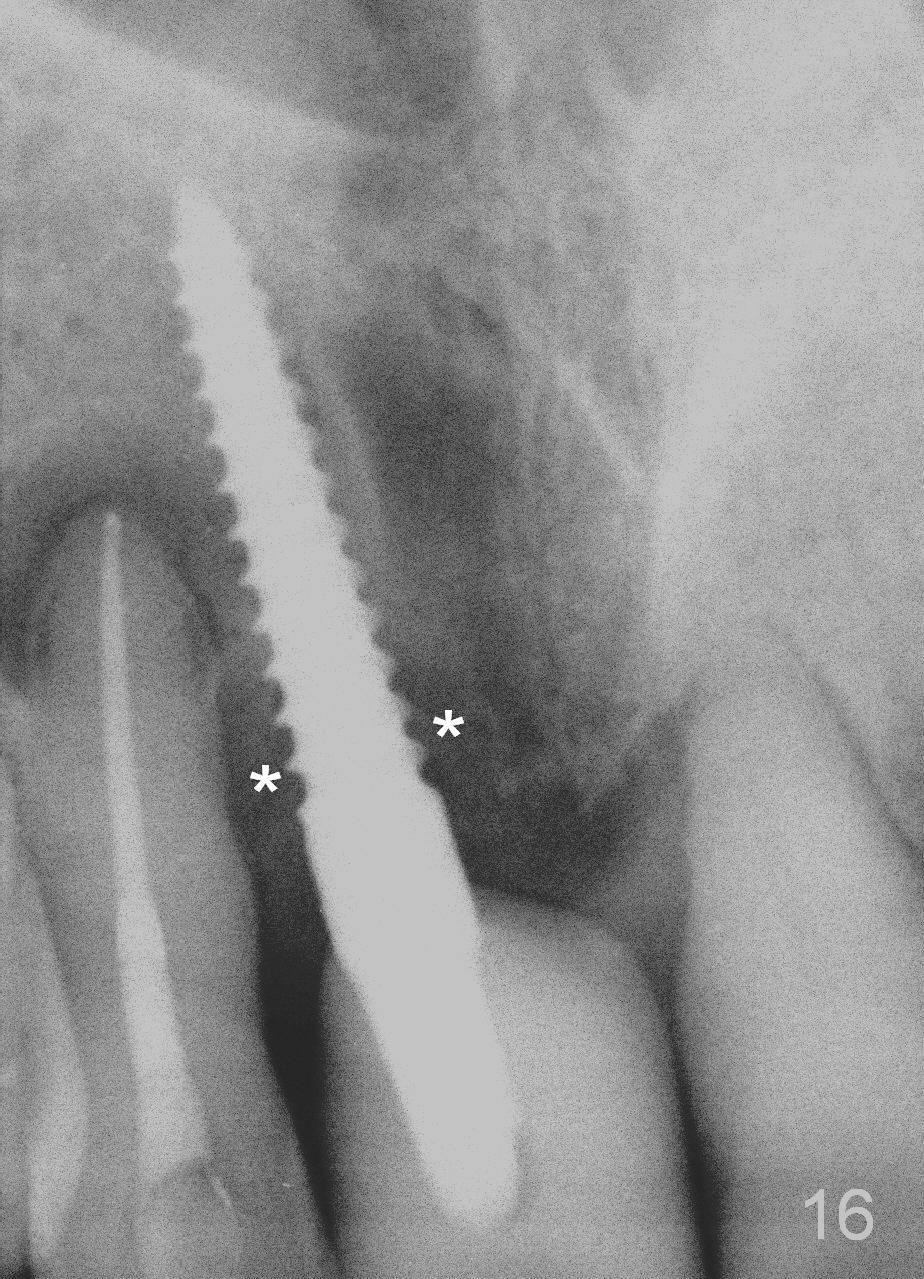
The patient returns for follow up 3 months post cementation. More bone deposits around the coronal end of the implant (Fig.16 *).
Return to Upper Incisor Immediate
Implants
Xin Wei, DDS, PhD, MS 1st edition 06/07/2014, last revision 03/28/2015