











|
|
|
|
|
|
|
||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|||
|
|
|
||||||
Potential Infection Site
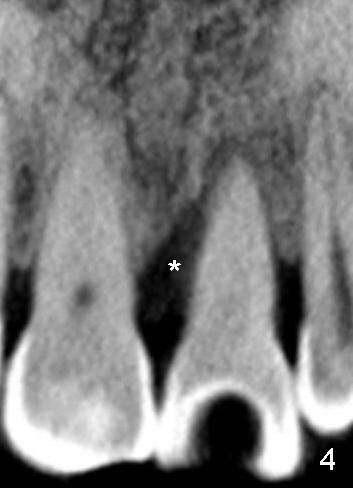
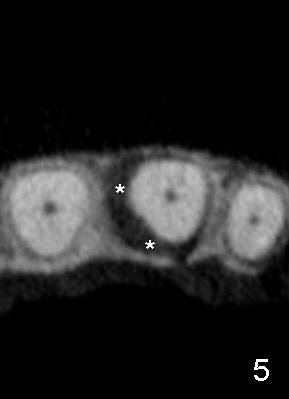
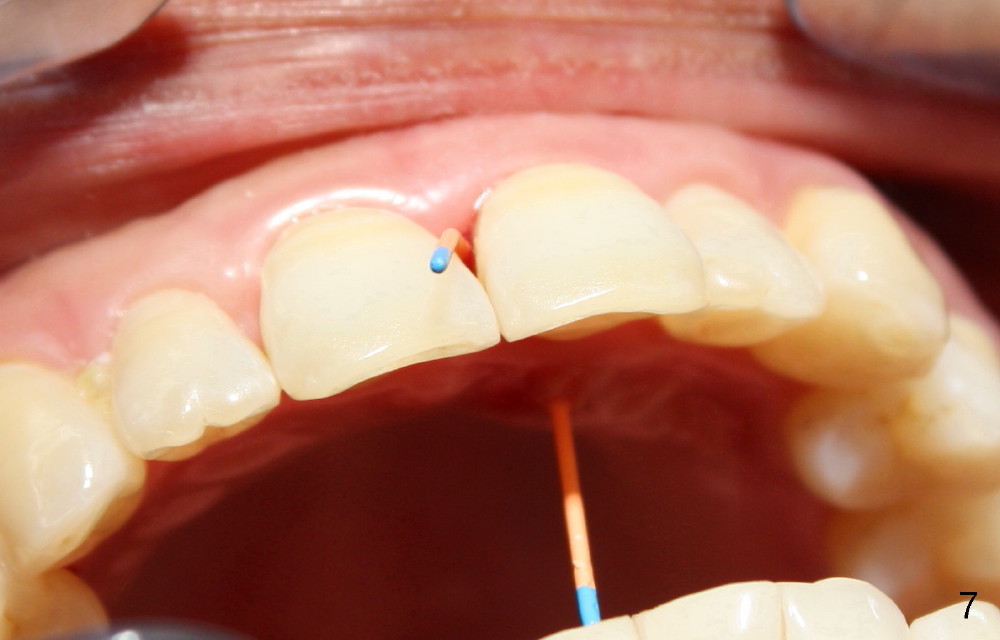
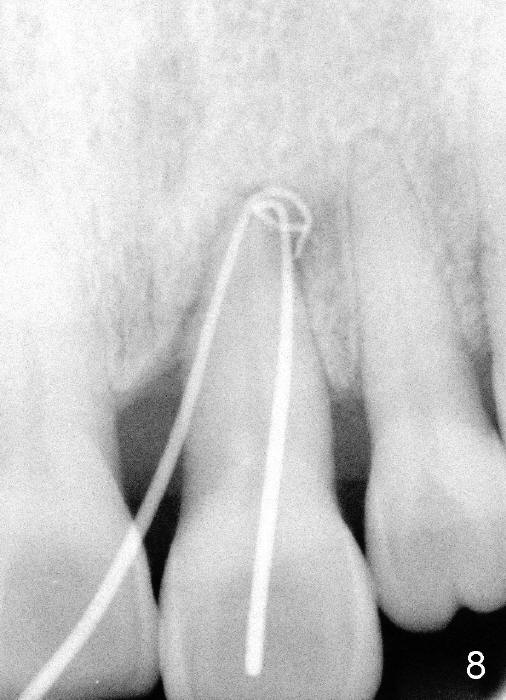
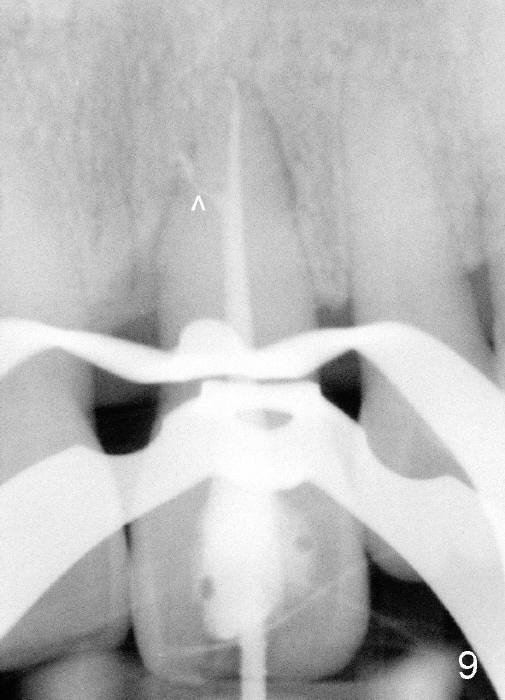
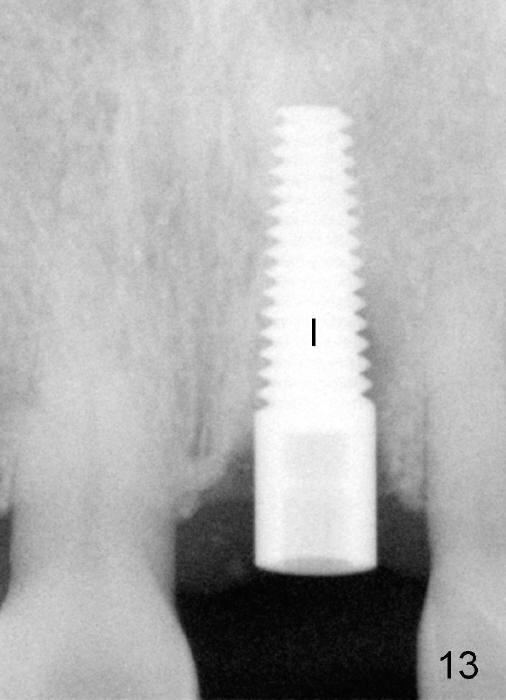
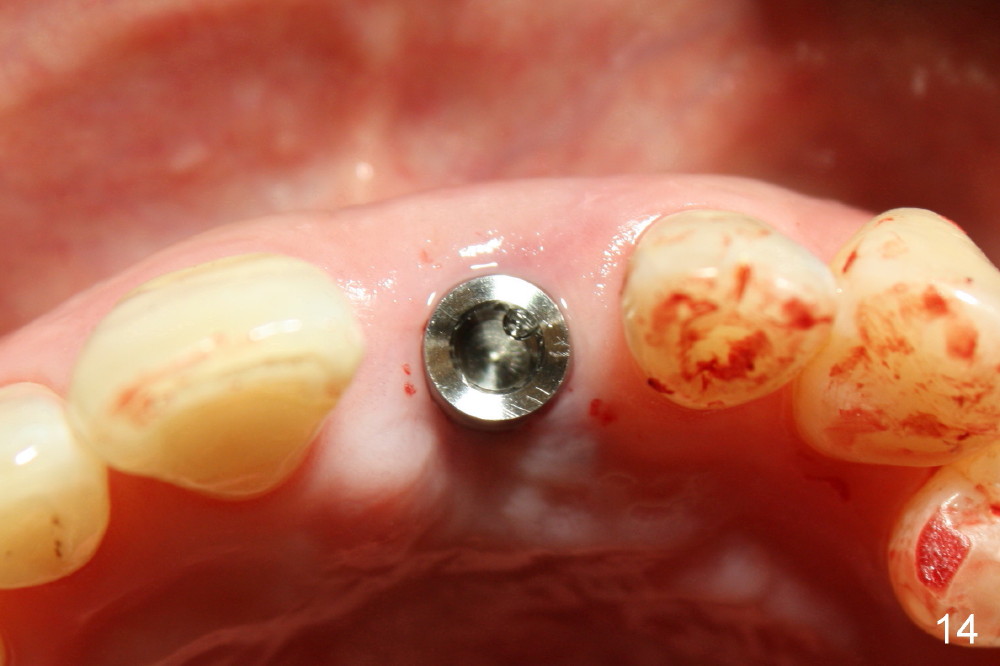
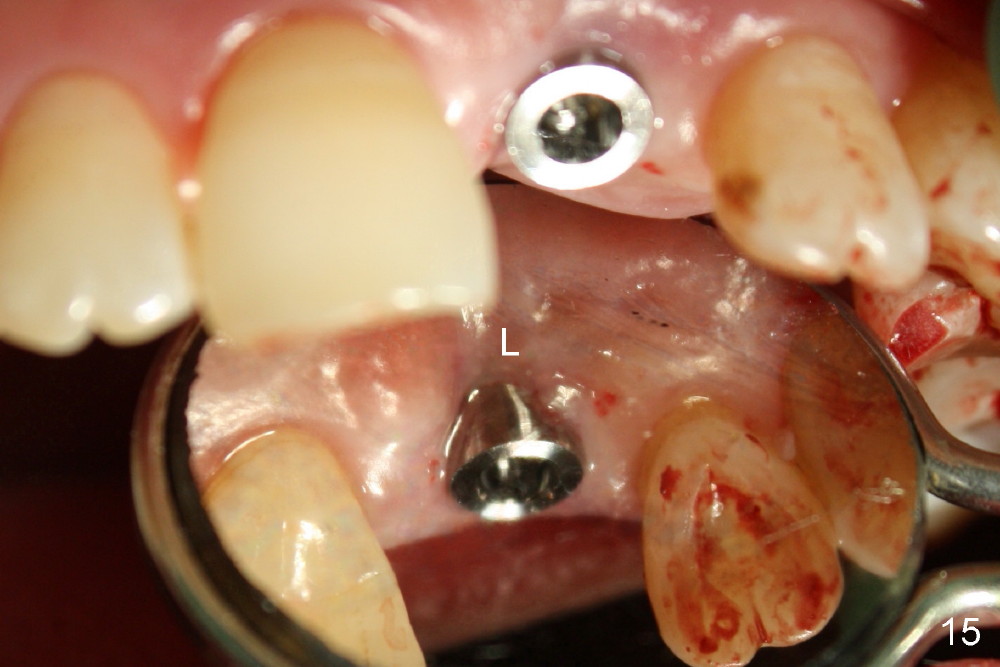
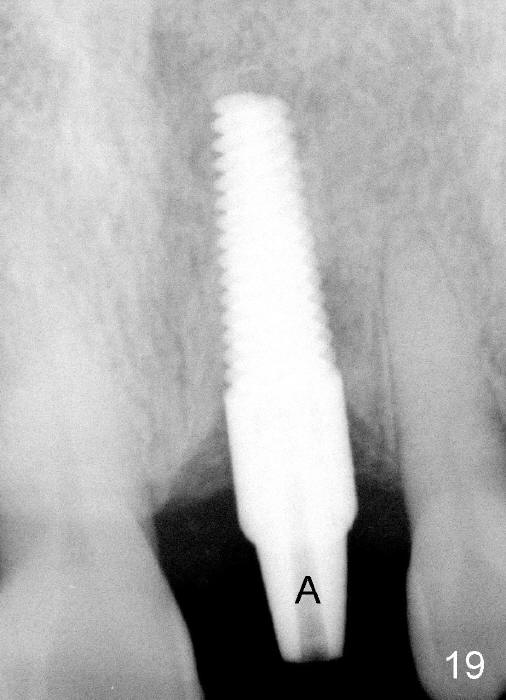
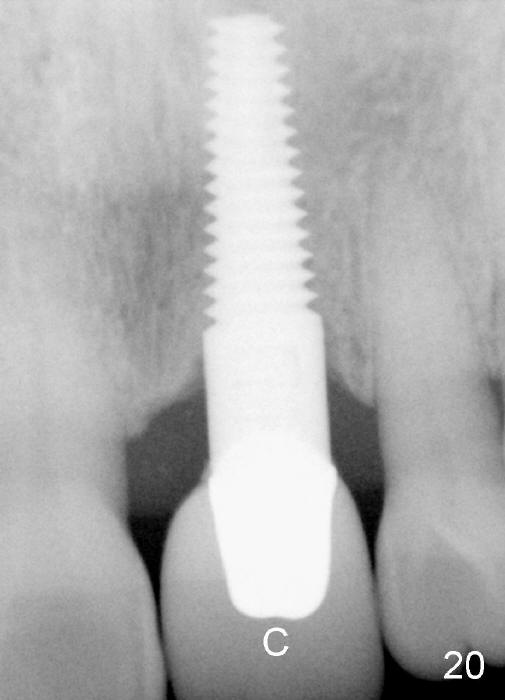
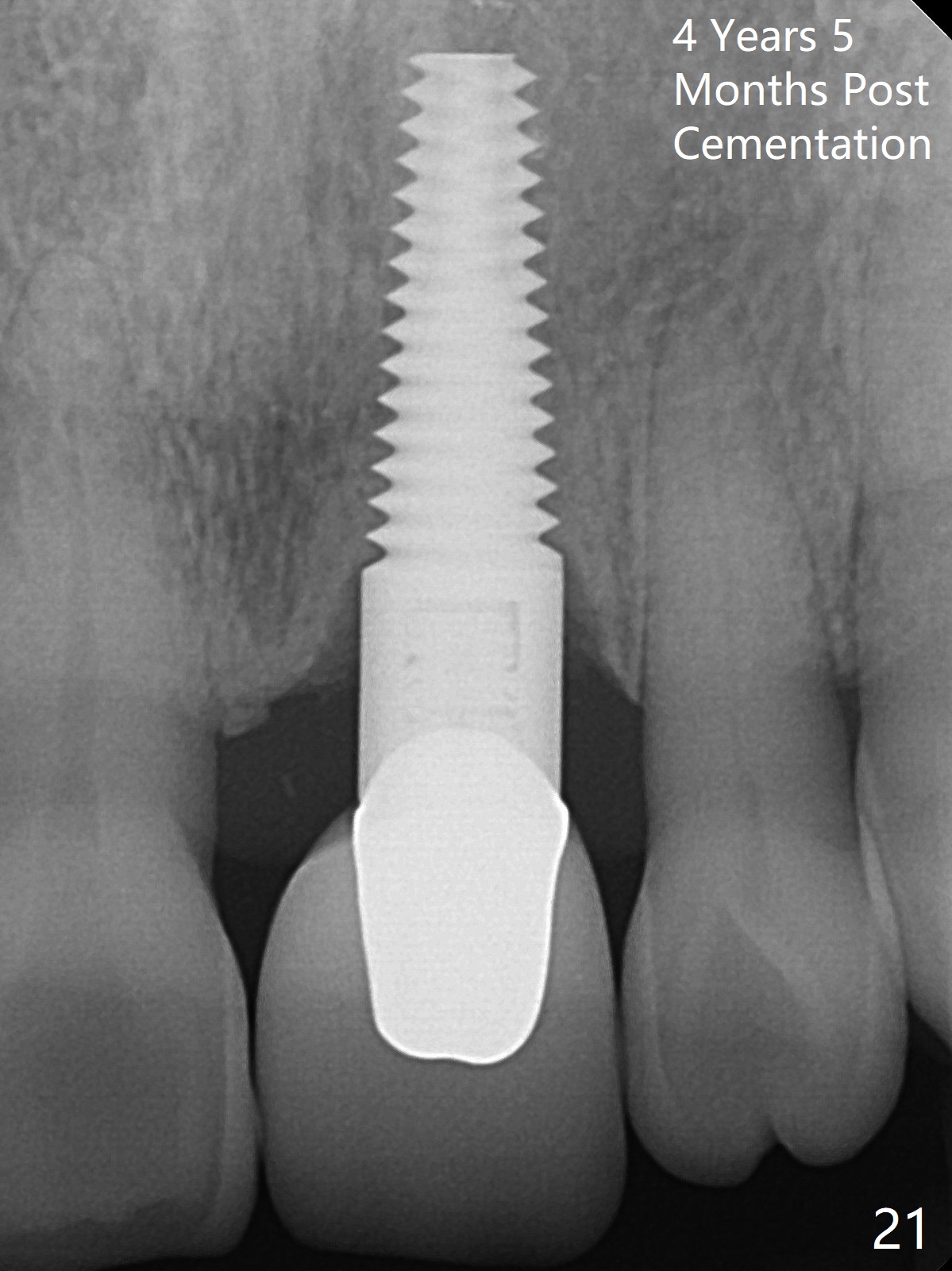
A 60-year-old lady had an abscess mesial to #9 six years ago (Fig.1,2 <), treated as a perio lesion by laser (Fig.3) and osseous surgery without bone graft (Fig.6, followed by CT exam revealing semi-circumferential bone loss (Fig.4,5). When the perio treatment failed, attention was paid to endo aspect (Fig.7-9). In fact the pulp was found to be vital when access to root canal therapy was made. As expected, the treatment failed again. The palatal fistula persisted. The infection was suspected to be a source of remote immediate implant site (#30). The tooth #9 was extracted. It appears that there is a semilunar crack line in the linguomesial root (Fig.12). When the socket healed 2 weeks post extraction (Fig.10), the #30 buccal defect was debrided with bone graft. There was no bone resorption 4 weeks post extraction (Fig.11); a 4.5x17 mm implant was placed (Fig.13-15). An immediate provisional was fabricated (Fig.16-18). Fig.19,20 were taken 3 months post implantation and 7 months post cementation, respectively. Dense bone forms around the implant coronally 4 years 5 months post cementation (Fig.21), while the gingiva is healthy palatally (Fig.22) and buccally (Fig.23).
Return to
Upper Incisor Immediate
Implant
19
Xin Wei, DDS, PhD, MS 1st edition 11/02/2014, last revision 07/08/2018