




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Use of Osteotomes to Avoid the Incisive Canal
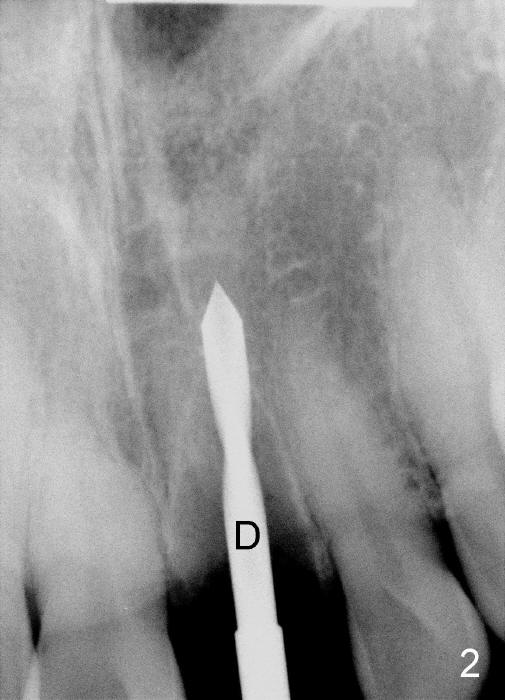
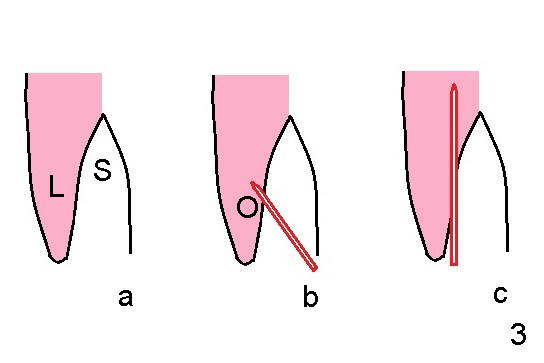
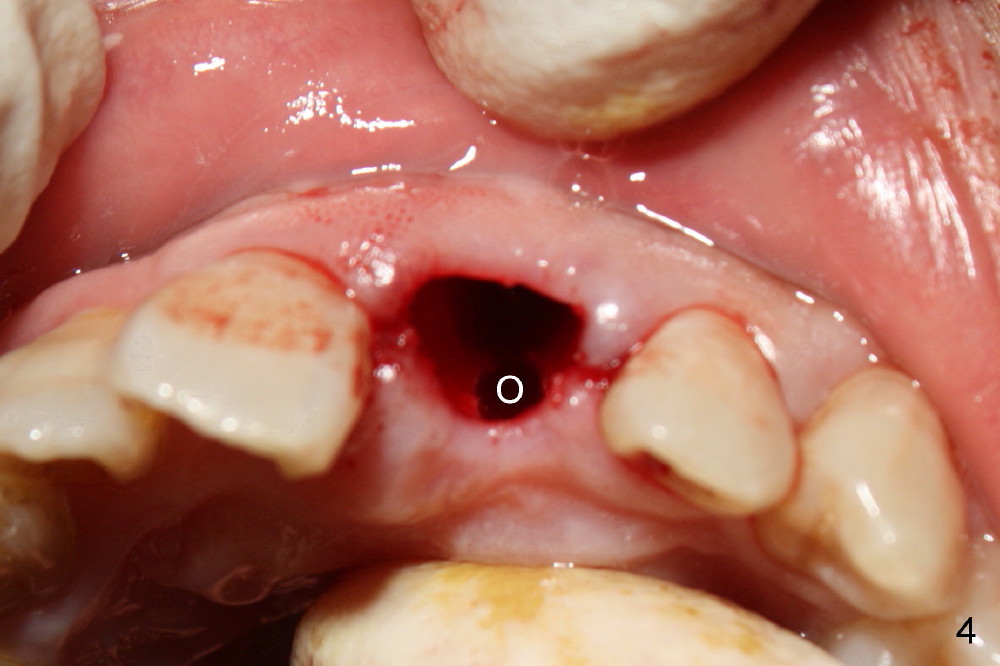
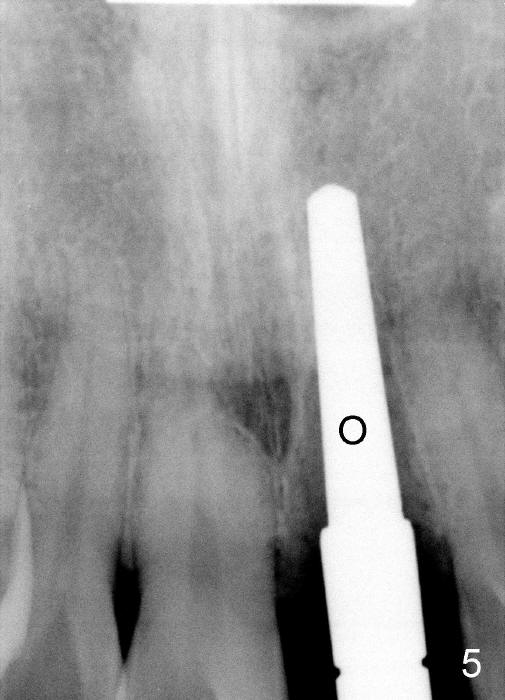
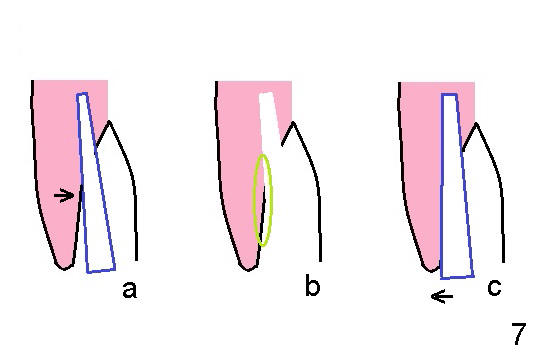
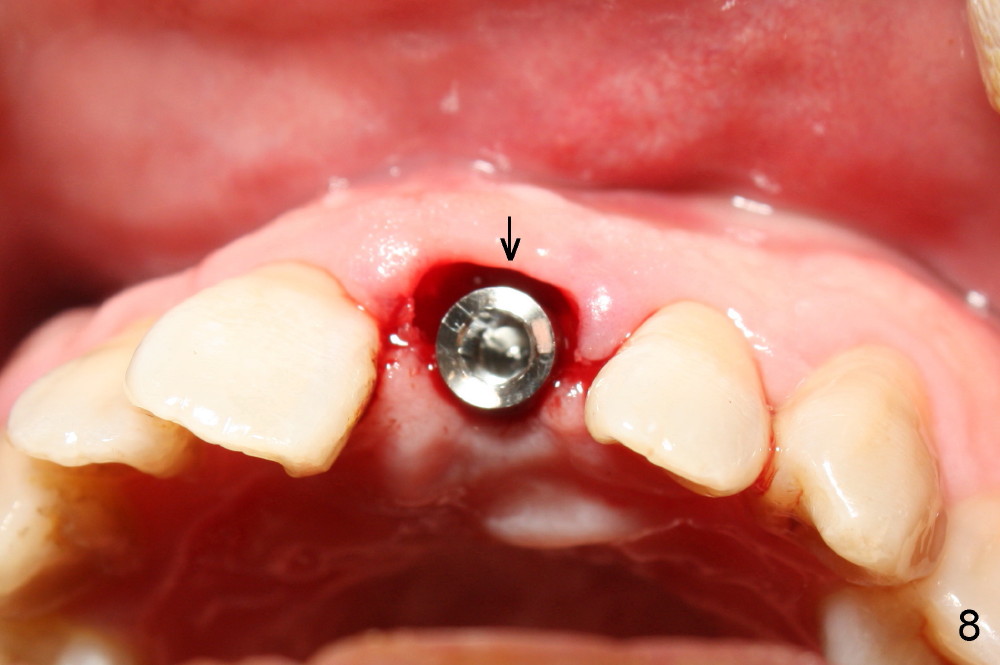
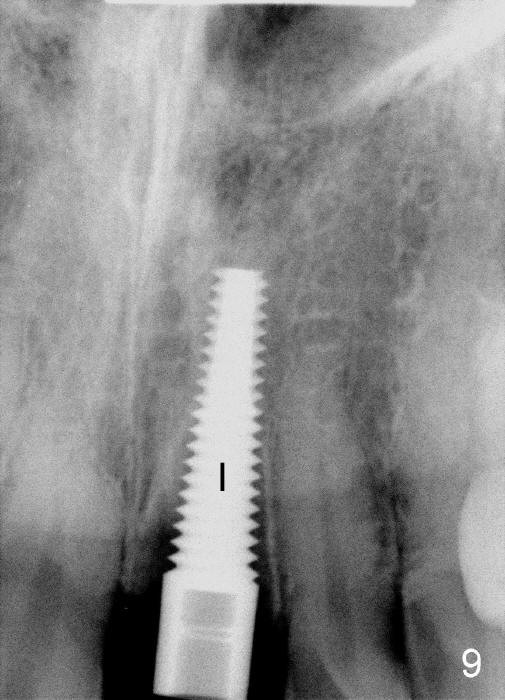
The upper right central incisor (Fig.1: #9) fractures subgingivally due to trauma for a 40-year-old man. The incisive canal is large (I) and close to the root of the central incisor. After extraction, the osteotomy (Fig.3b, 4: O) is made with 2 mm pilot drill (Fig.2: D) on the lingual wall (Fig.3a: L) of the socket (Fig.3a: S). To push the incisive canal mesially, the osteotomy is enlarged by 3.5x21 mm and 4x21 mm tapered osteotomes (Fig.5,6: O). Due to the lingual slope (Fig.7a arrow), the osteotome (blue outline) starts to deviate bucally. To reduce this tendency, the coronal portion of the lingual slope is removed (Fig.7b: yellow circle). The final implant (4.5x20 mm) is able to be placed as lingually as possible (Fig.7c, 8).
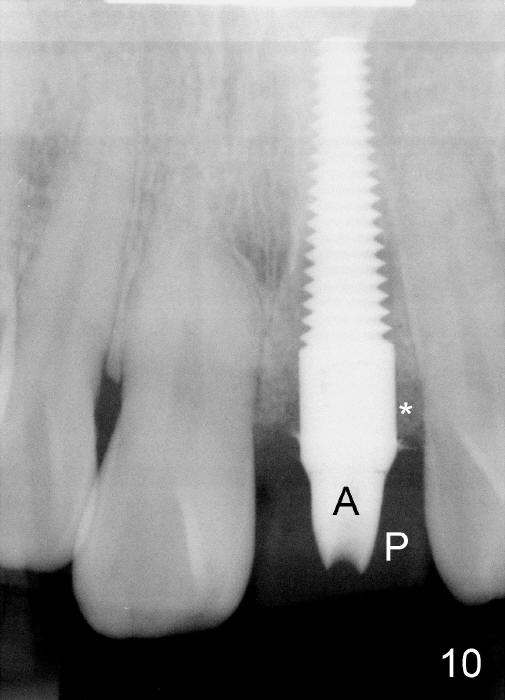
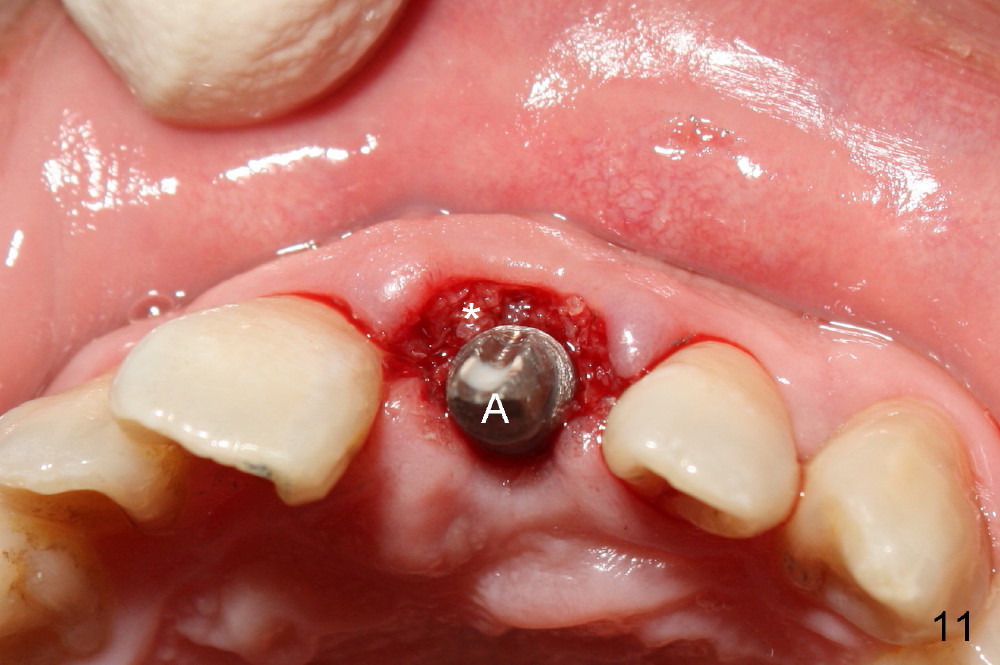
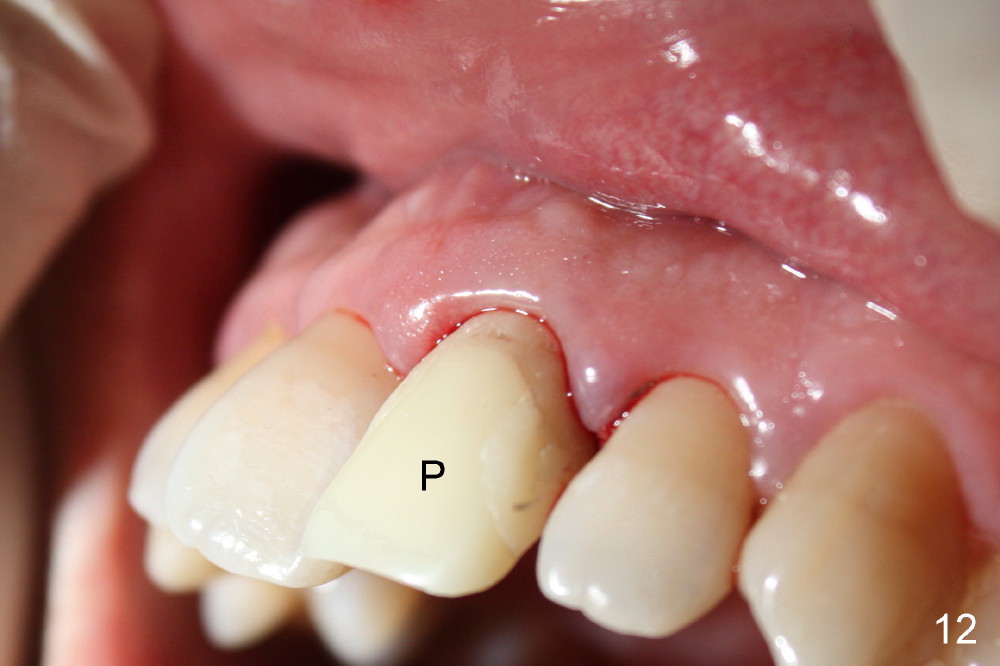
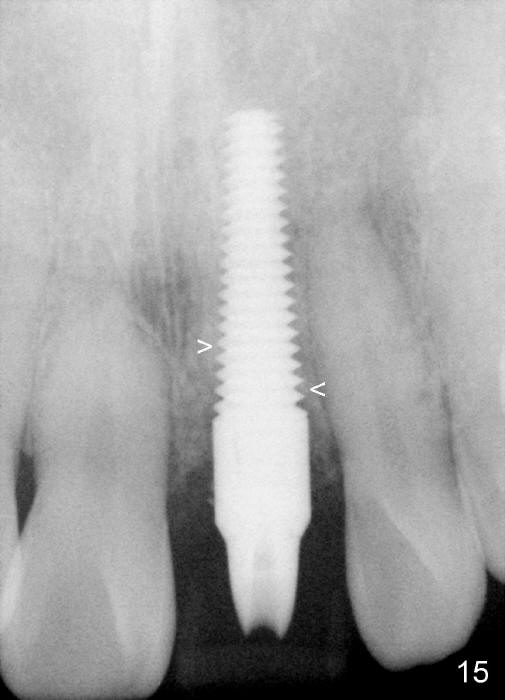
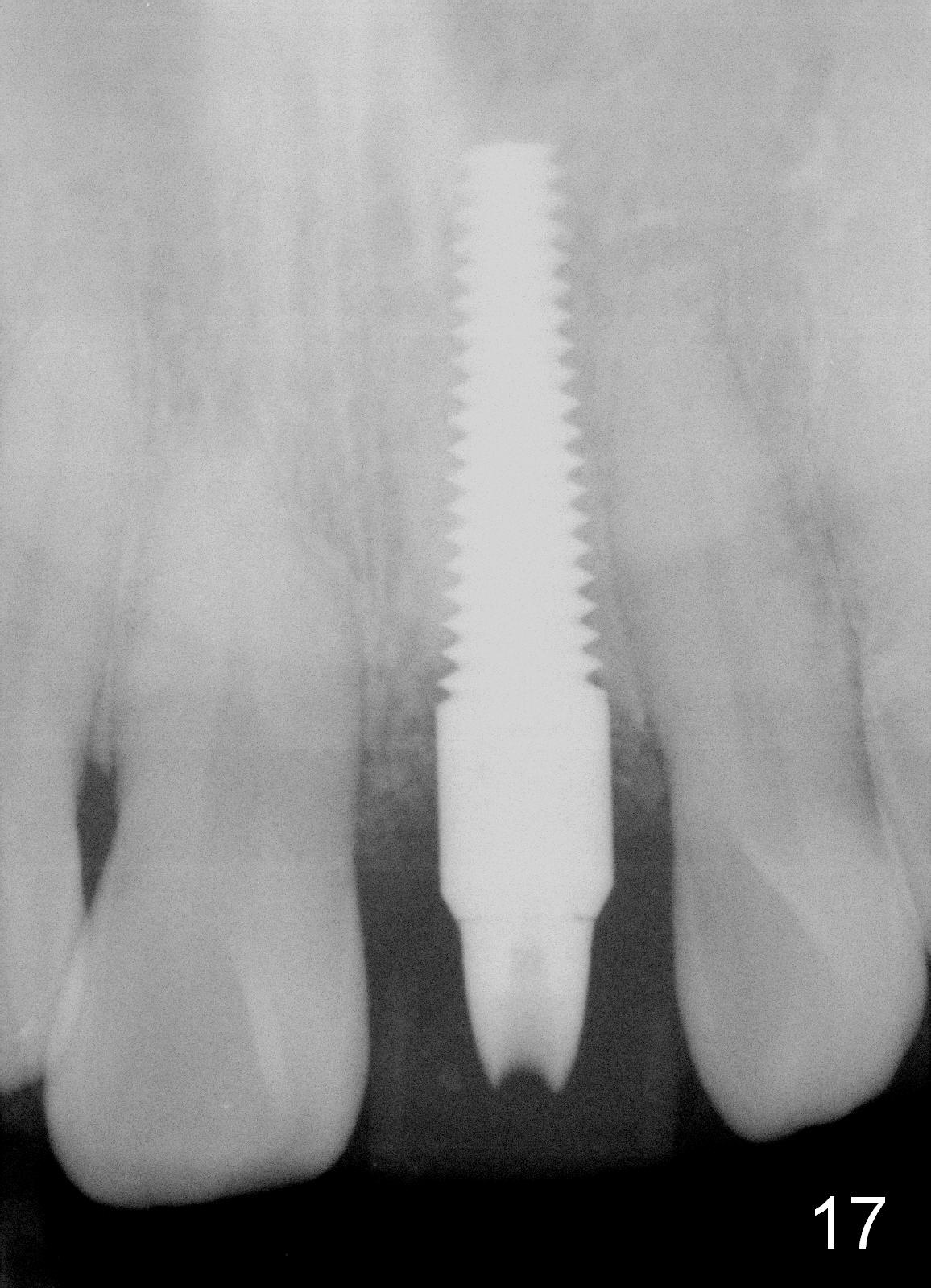
Bone expansion allows the implant (Fig.9 I) to have primary stability (insertion torque between 50 and 60 Ncm), since the cortex of the incisive canal is apparently intact. Allograft is placed in the labial gap (Fig.10, 11 *) following installation of the abutment (A). Finally an immediate provisional (Fig.10,12 P) is cemented. Fig.13,14 are taken 8 days postop. The patient returns 3 months postop (Fig.15,16). Osteointegration appears to have occurred (Fig.15 arrowheads) and is more obvious 9 months postop (Fig.17).
The permanent crown is temporarily cemented because of misshade and undercountour at the cervix (Fig.18).
Return to Upper Incisor Immediate
Implant,
Dr. Wu
Xin Wei, DDS, PhD, MS 1st edition 06/19/2014, last revision 04/02/2015