





|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
Nasopalatine Canal and Immediate Implants
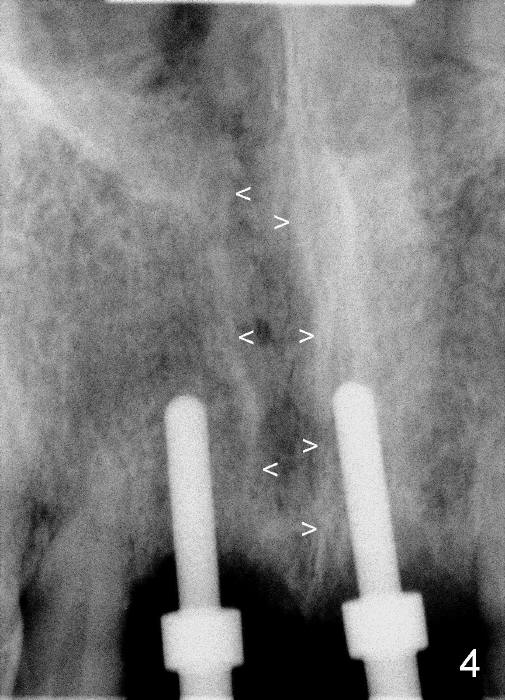
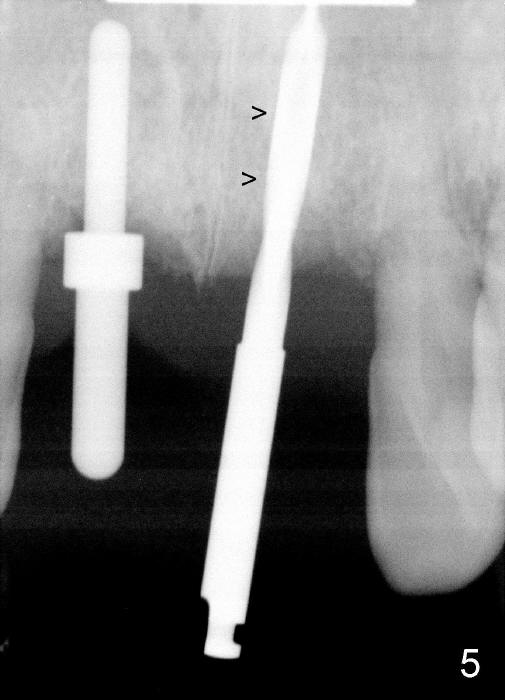
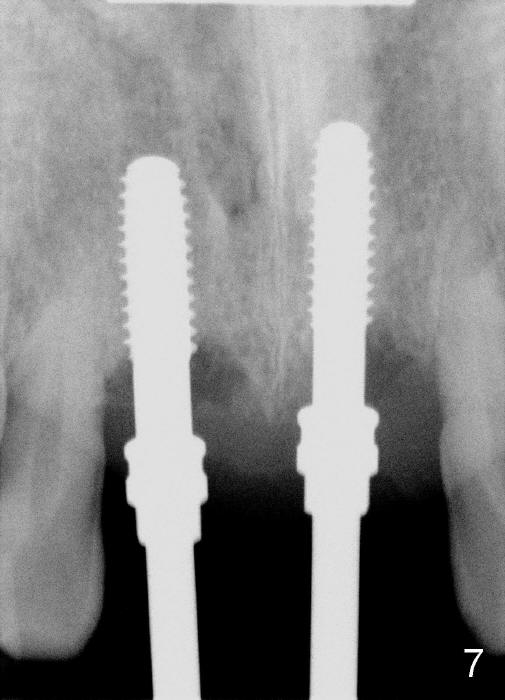
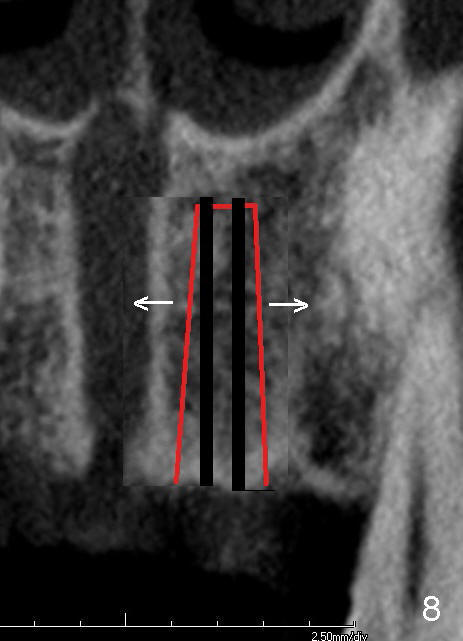
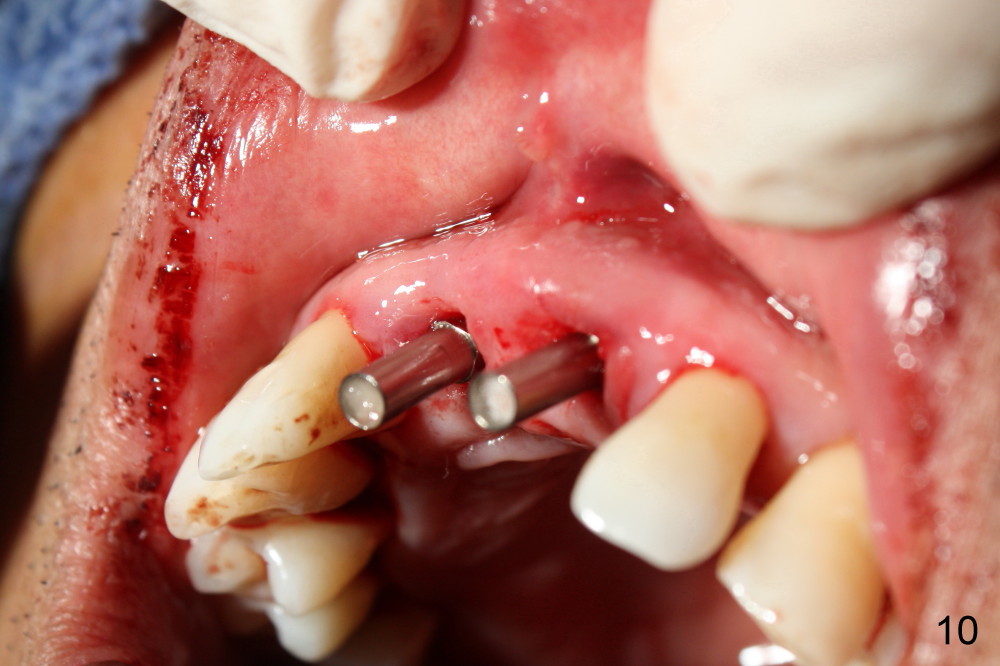
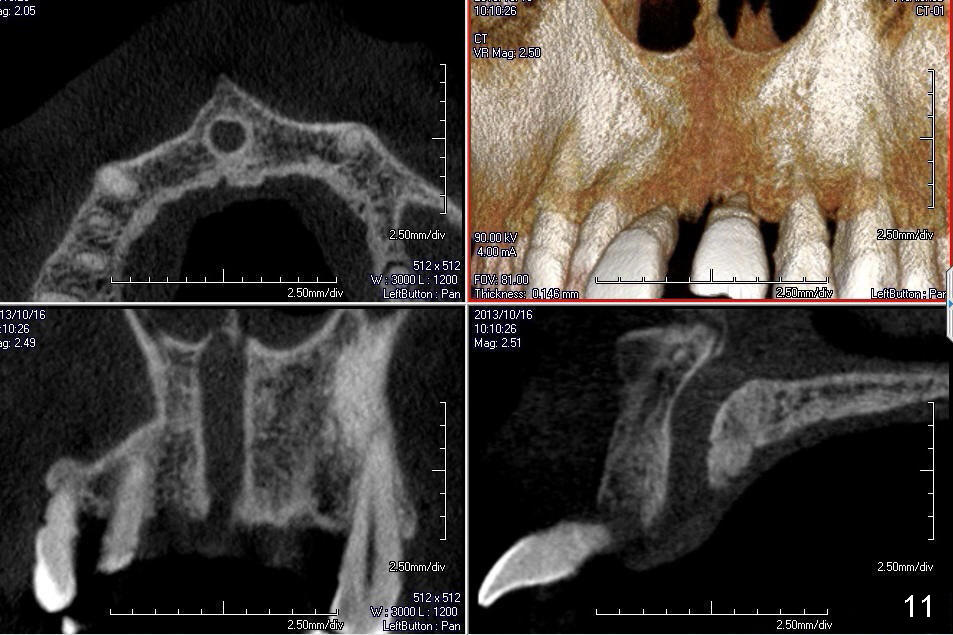
The patient returns for immediate implants for #8,9 following scaling & root planing of the upper arch (Fig.1). Paralleling pins are placed in the sockets lingually (Fig.2) with improved overjet (Fig.3). It appears that the left paralleling pin is close to the nasopalatine canal (Fig.4 arrowheads). The left trajectory is adjusted (Fig.5). The osteotomies are being expanded with taps (Fig.7, compare Fig.6,8). Although there is more oozing from the left osteotomy than the right one (Fig.2), there is no hemorrhage when implants are placed with reasonable primary stability (Fig.9,10). No bone graft is placed. The nasopalatine canal is studied using CBCT scans after surgery (Fig.11). There is no important structure within the nasopalatine canal. The osteotomies are under prepared (Fig.6 (from CT coronal section) red lines) and then expanded with taps and implants, pushing the wall of the nasopalatine canal medially (Fig.8 arrow).
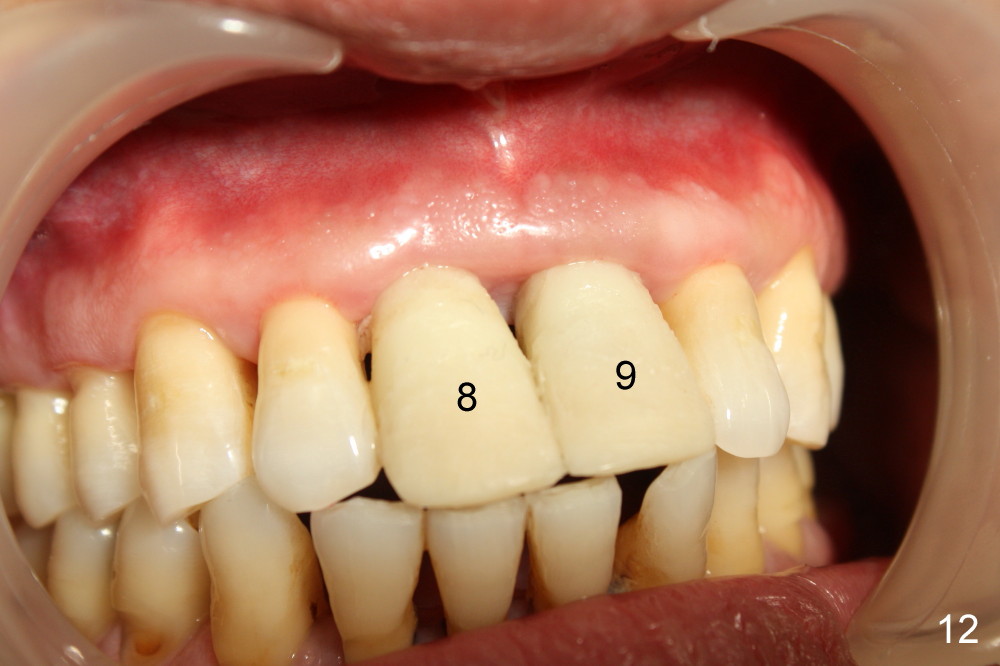
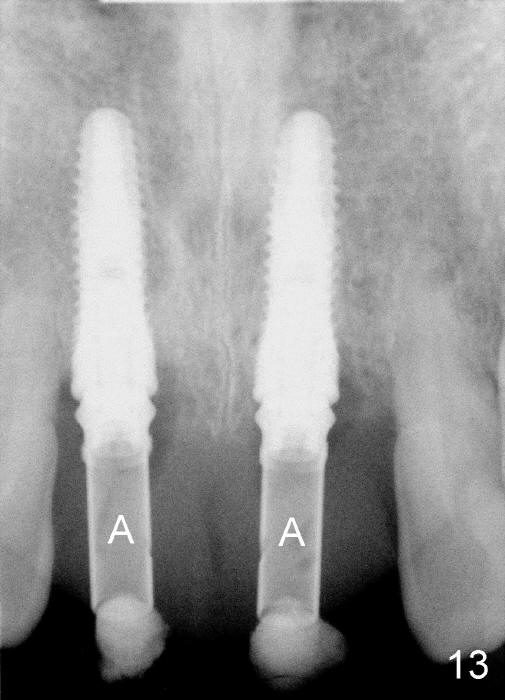
Fig.12 shows immediate provisionals 3 days postop. Four months later, the implants appear to have osteointegrated (Fig.13); there is no buccal plate atrophy (Fig.14).
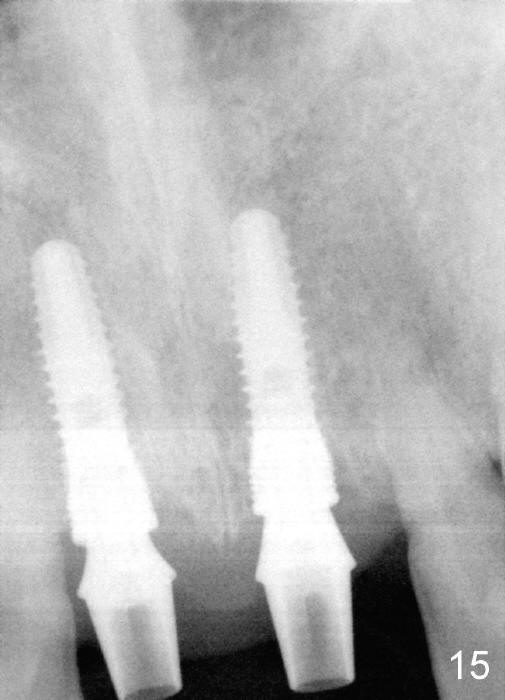
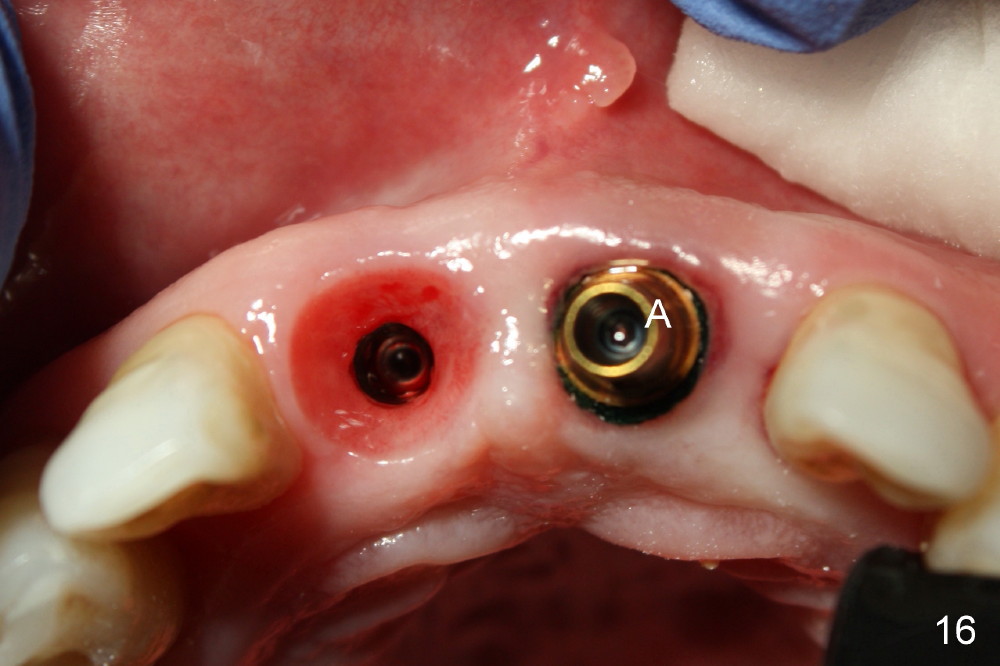
The patient returns for impression 4.5 months postop (Fig.15-17): an abutment (Fig.16 A) having been placed at the site of #9, while the healing abutment just removed at the site of #8 (gingiva healthy).
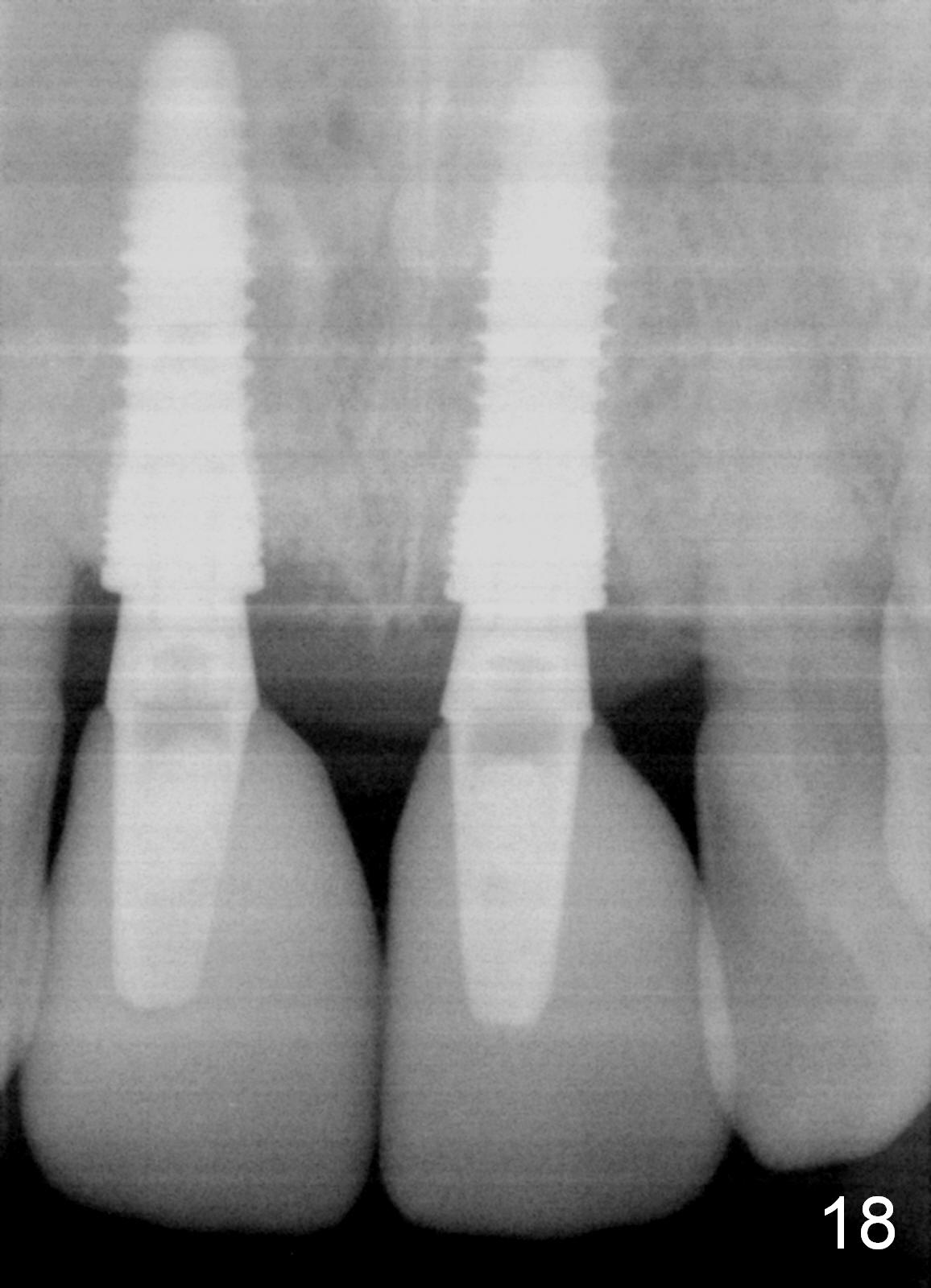
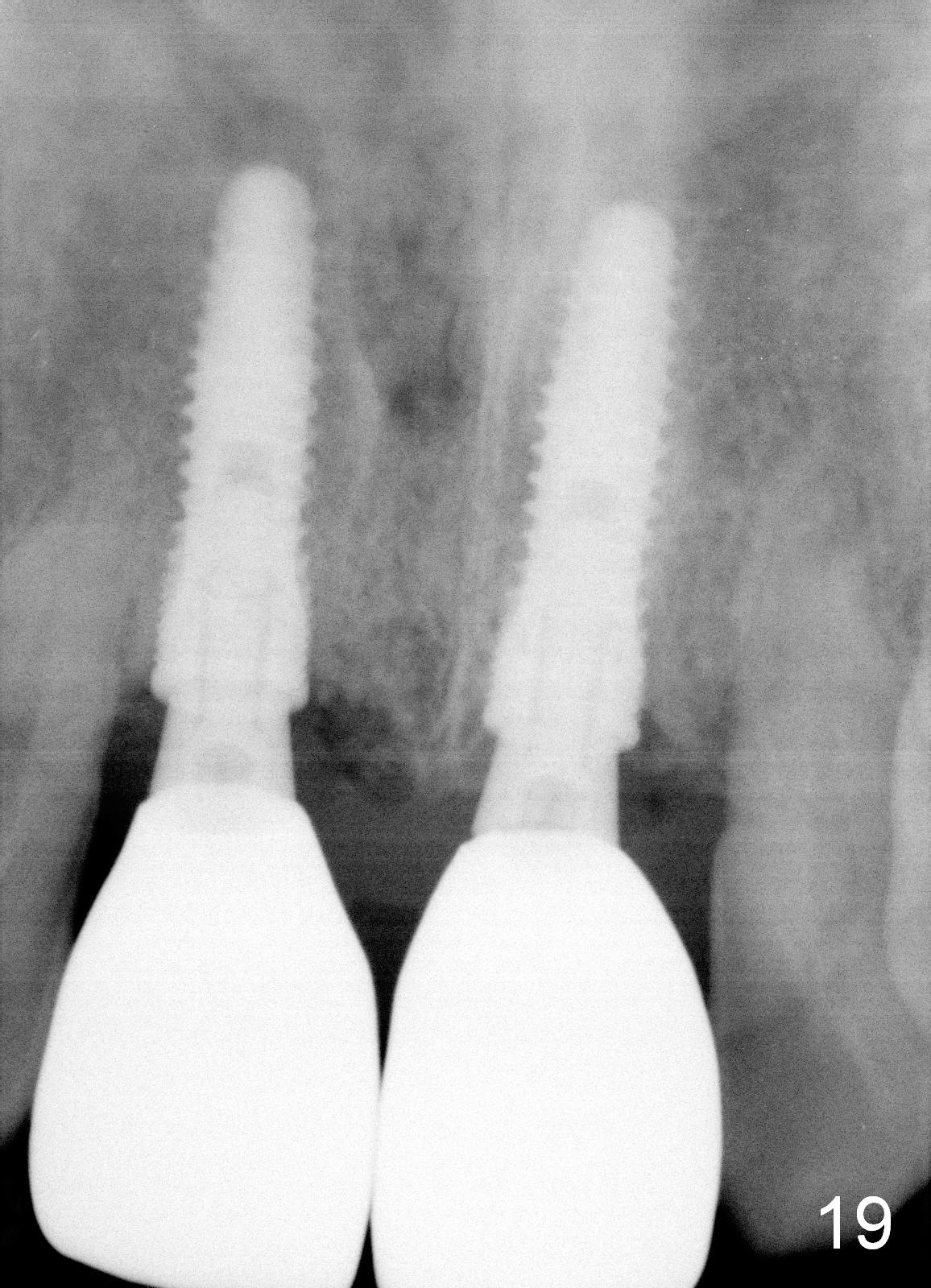
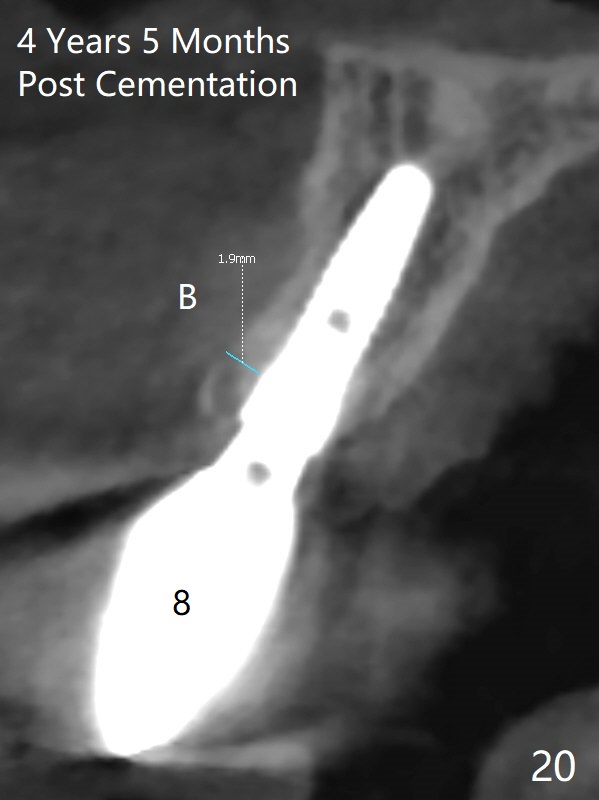
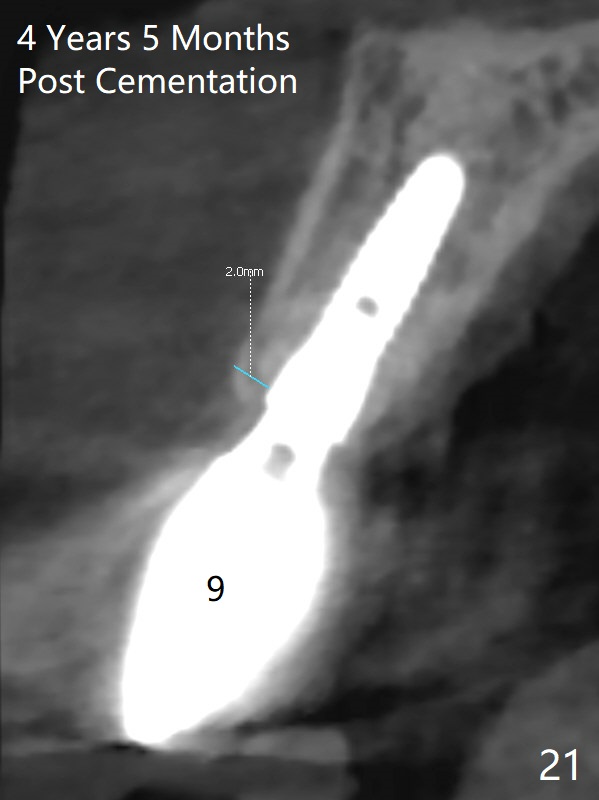
The patient is not satisfied with crowns, 2 months post cementation, 6 month postop (Fig.18). Fig.19 shows the crowns 6 months after redo, 14 months postop. There is 2 mm bone buccal and palatal to the implants 4 years 5 months post cementation (Fig.20,21).
Return to Upper Incisor
Immediate Implant
28/31
Xin Wei, DDS, PhD, MS 1st edition 06/02/2014, last revision 07/25/2019