
.jpg)










|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
||||
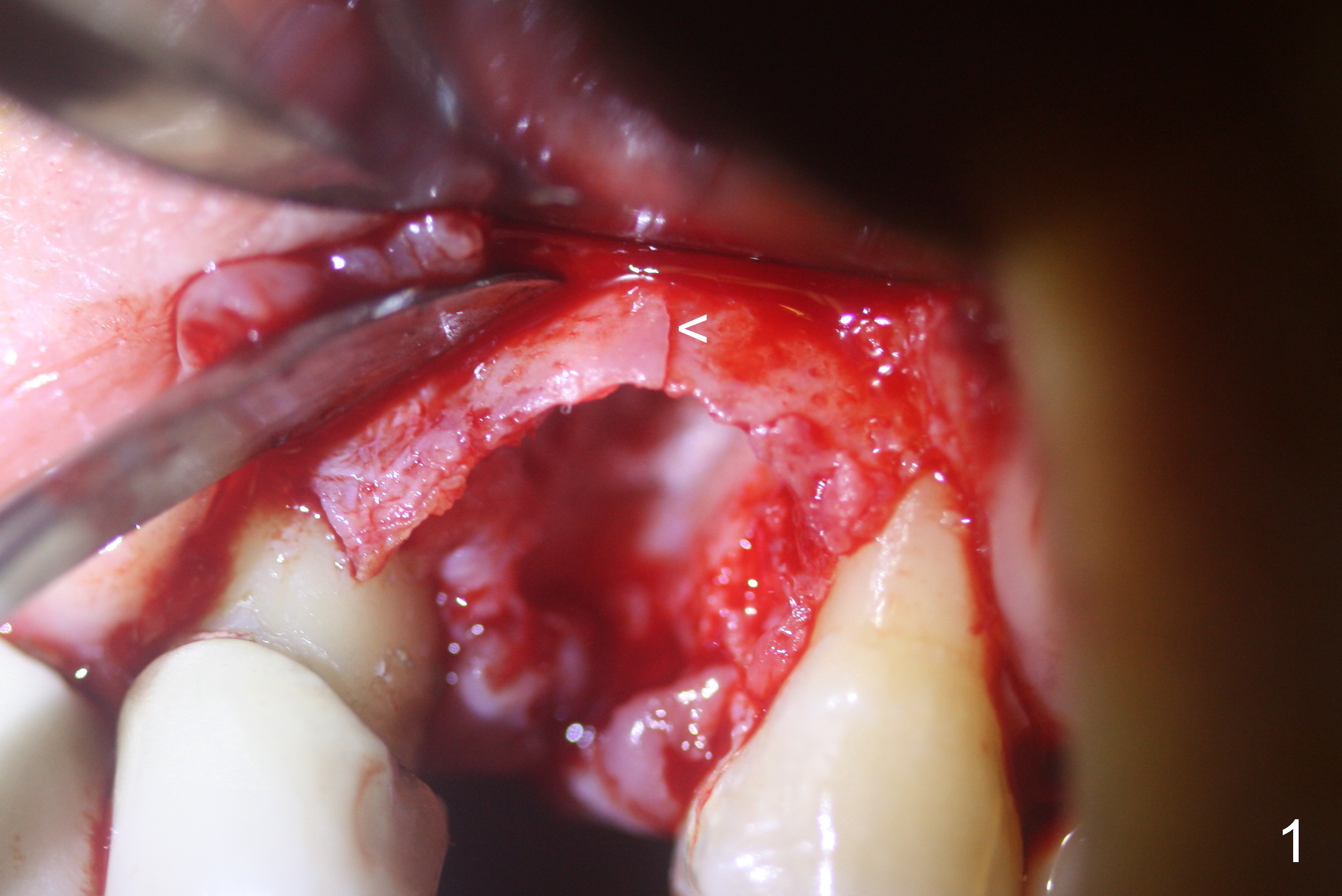
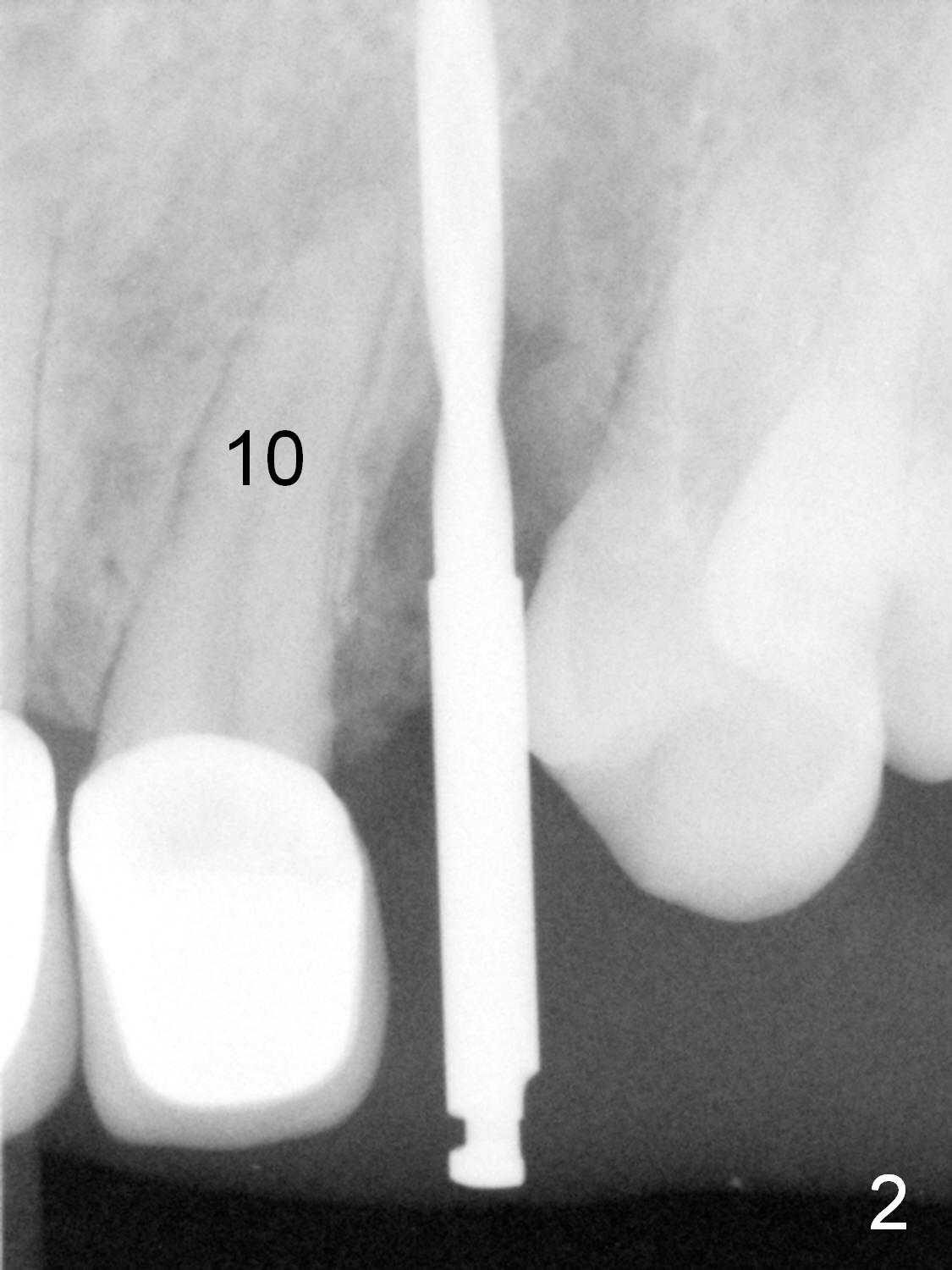
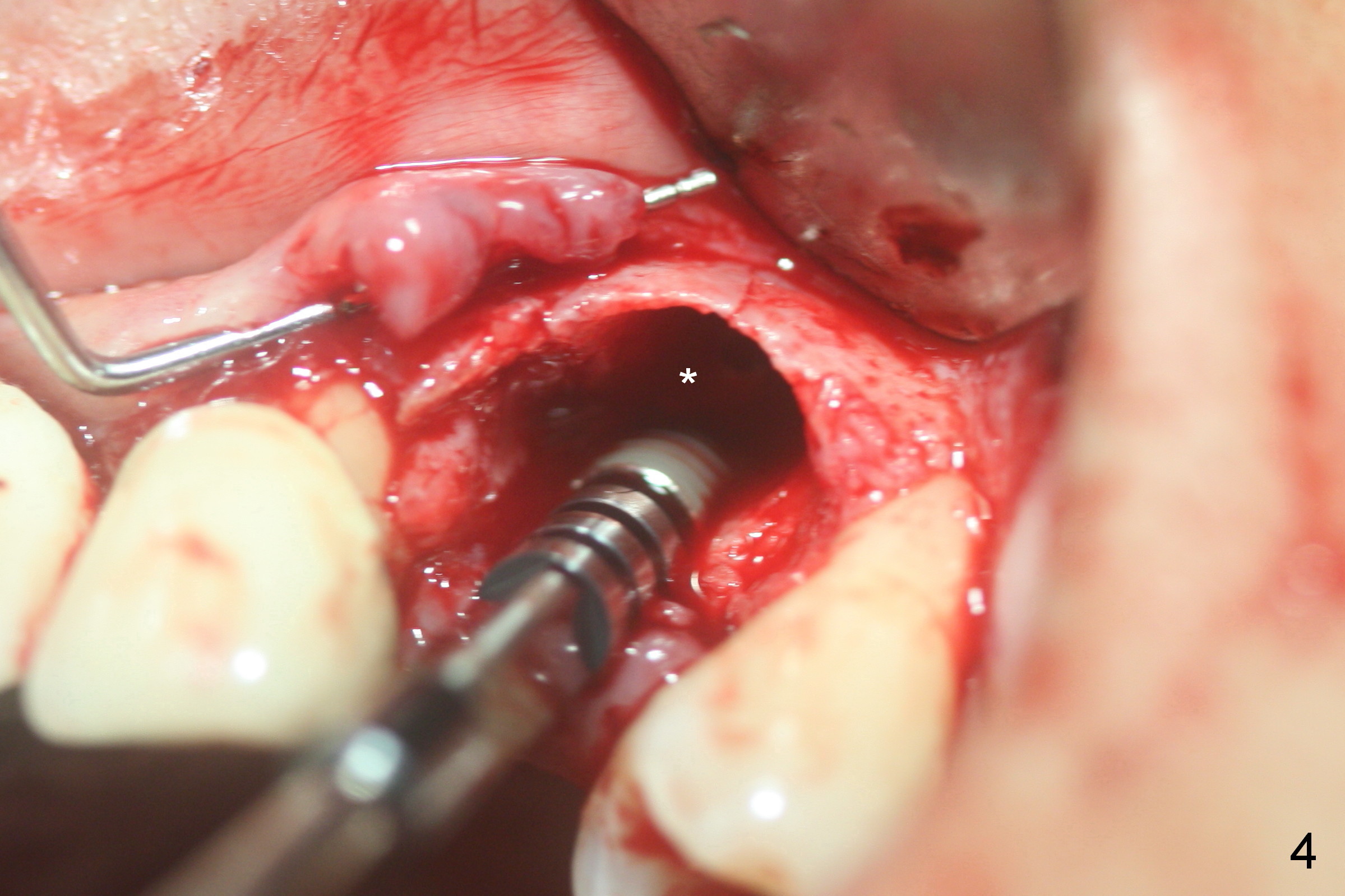
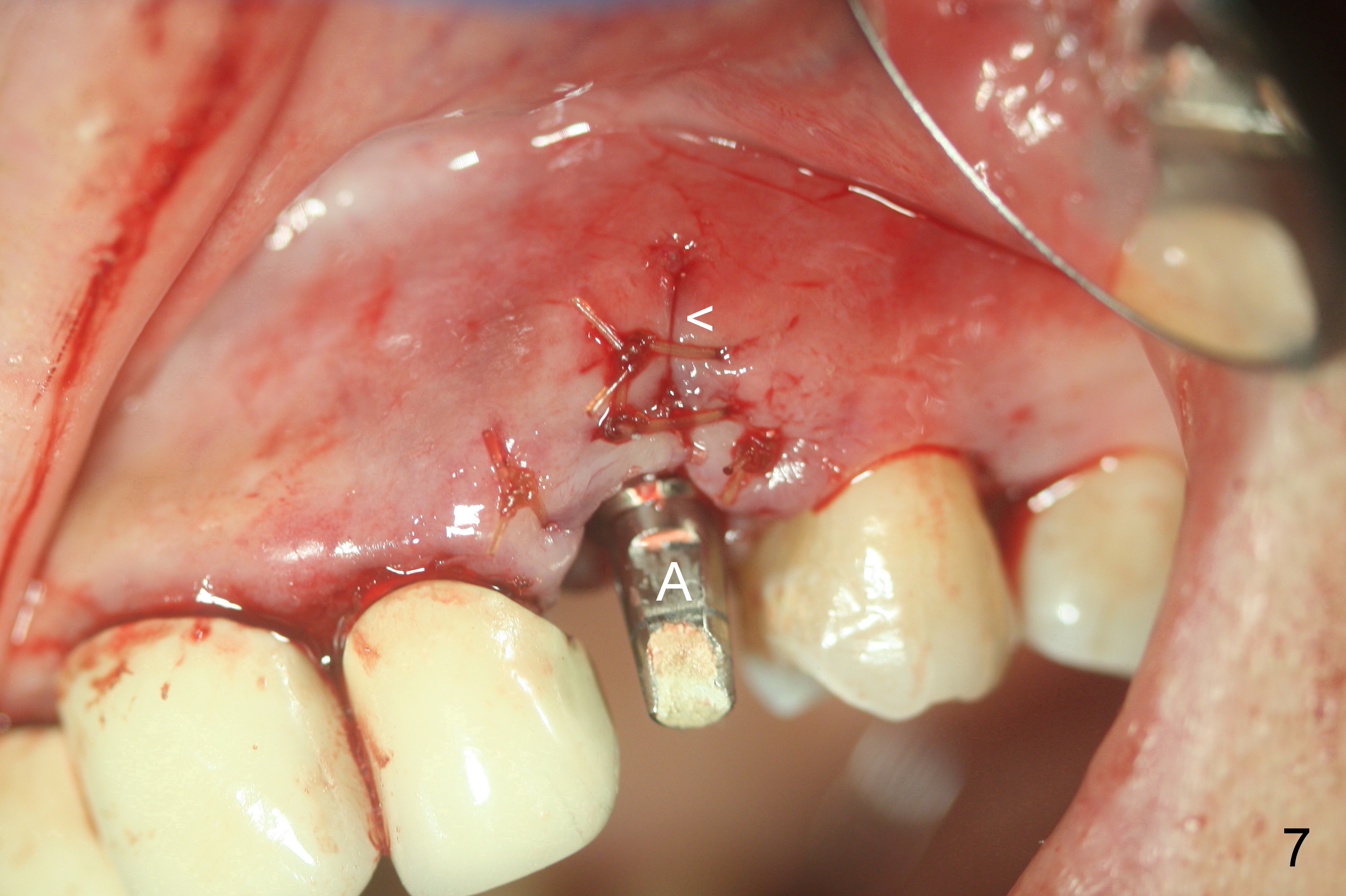
Labial sulcus incision is made to extract the residual root at #11; the labial plate is thin with a crack line (Fig.1 <). A 2 mm pilot drill appears to be close to the root tip of the tooth #10 in one of PAs (Fig.2) and seems to be parallel to the root of the tooth #12 in the other (Fig.3). On the other hand, the roots of the teeth #10 and 12 are apparently parallel (Fig.2,5,6). In spite of the artifact, the osteotomy is moved slightly distal. The biggest challenge is the narrow mesiodistal space at #11 so that a smaller implant than expected is placed (Fig.4: 3.8x18 mm). The large labial gap (Fig.4 *) is filled with allograft/Osteogen (Fig.5,6 *). A long abutment is placed (Fig.5-7 A (4.5x7(4) mm) for an immediate provisional. Gingival laceration (Fig.7 <) could be avoided if two oblique accessory incisions were made or the gingival sulcus were extended more laterally.
There is no crestal bone loss 6.5 months postop (Fig.8). Although there is buccal gingival recession (Fig.9), the buccal plate does not collapse (Fig.10 *). Please stop the crown margin at the prep margin (Fig.11 ^). With better oral hygiene, the buccal recessed gingiva should be able to grow downward.
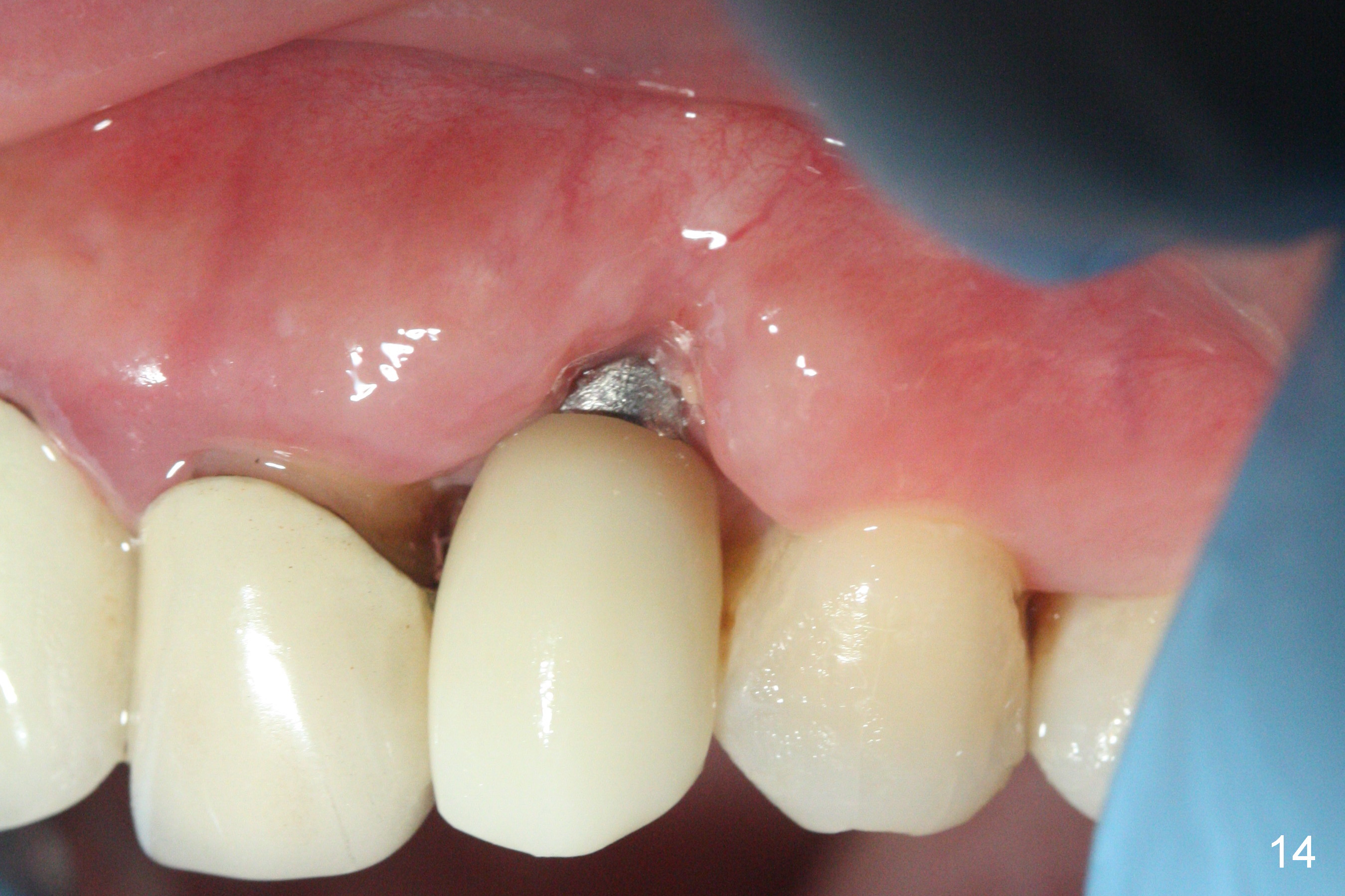
Indeed, the margin improves in a month (Fig.13,15), but the crown margin is short (Fig.14,16). The die margin should be higher (Fig.17 pencil mark).
The patient is satisfied with the redo (Fig.18). With good oral hygiene, the gingiva should be able to grow down to make the tooth look shorter. The attached gingiva seems to have been interrupted (^), due to laceration intraop.
Return to Upper
Canine Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 05/25/2016, last revision 01/31/2017