

|
|
|
|
|
|
|
|
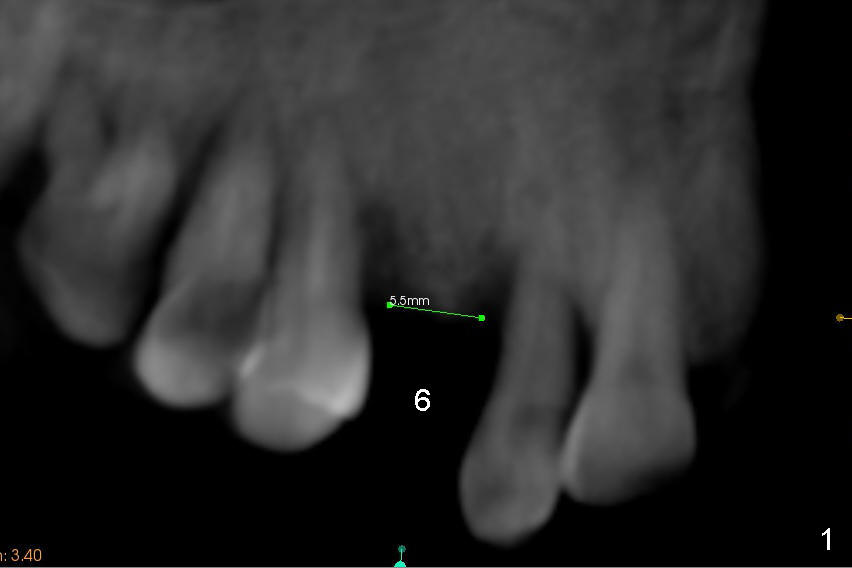
Bone Expansion at Healed Site
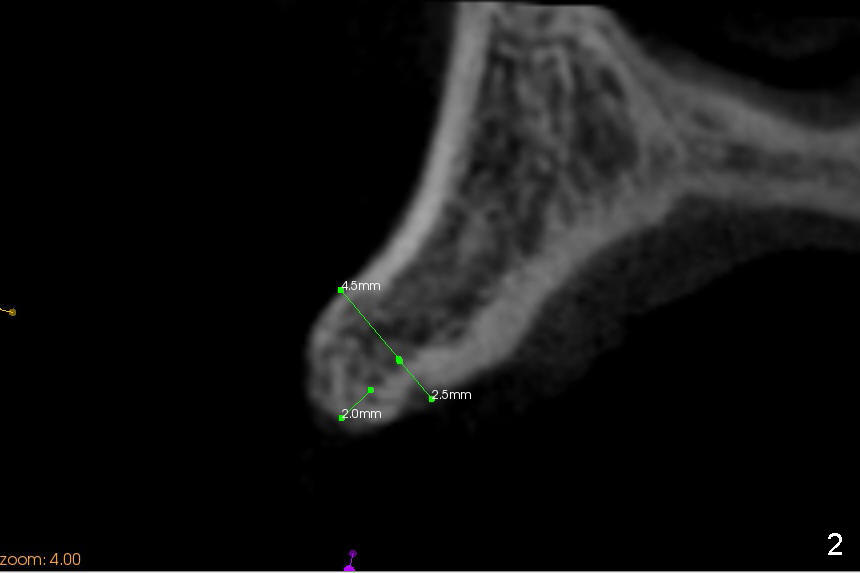
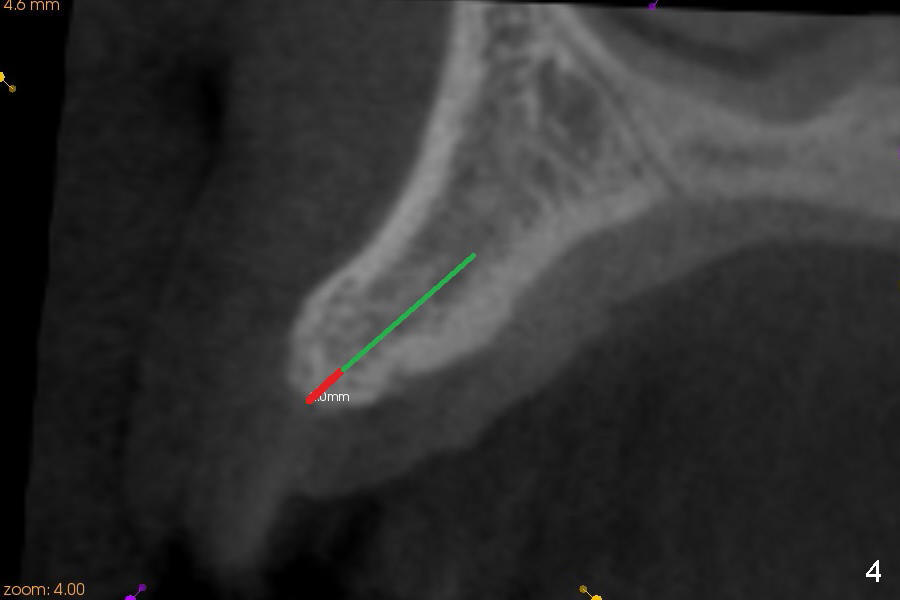
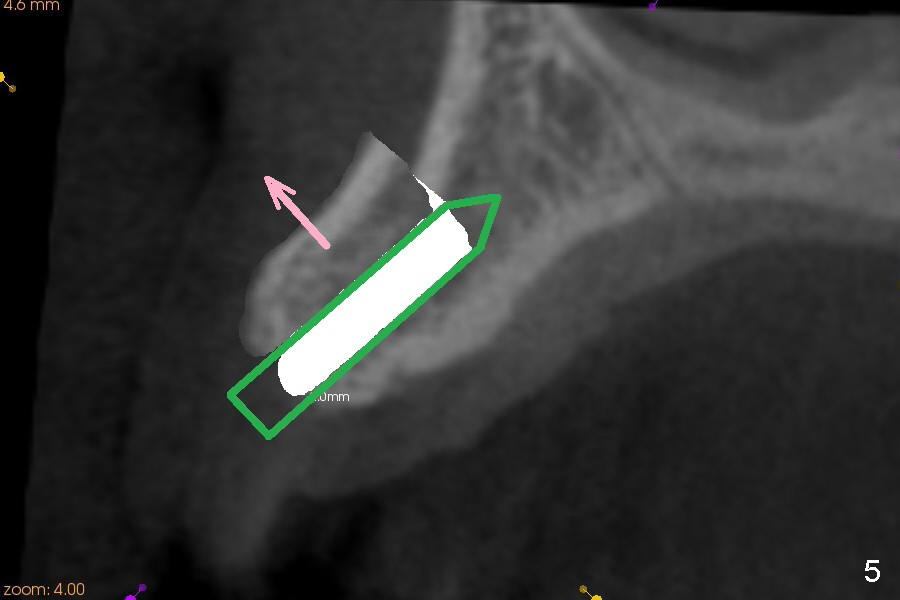
A 45-year-old lady has history of chronic periodontitis. The tooth #6 has lost several years (Fig.1). The buccolingual width decreases (Fig.2 (7mm), as compared to #11 in Fig.6 (10 mm)). Bone expansion is necessary for implantation. It should be done gently, since she is a dental phobic. First the crestal cortex is split with a surgical fissural bur (Fig.3 red line), followed by thin osteotomes (Fig.4 green line: scalpel, bone scalpels (probably until 5 or 6 mm, as indicated by Fig.1 (mesiodistal width)), bone blades (until 5.5 mm)). If the patient cannot tolerate tapping, 1.6 mm pilot drill is used at the depth of 14 mm, followed by bone expanders (probably until 2.9/3.8 using handpiece). As expanders or rounded osteotomes increases in diameter (Fig.5 green arrow), the buccal plate moves buccally (pink arrow). The bone expansion improves cosmetics as well. The implant is planned to be 4.5x14 mm, bone level. Angled abutment is expected. In contrast, immediate implant prevents buccal plate atrophy and avoids bone expansion. How is the surgery?
Return to Upper Canine Immediate Implant Xin Wei, DDS, PhD, MS 1st edition 11/16/2014, last revision 11/17/2019