|
|
|||
|
|
|
|
|
Bone Density
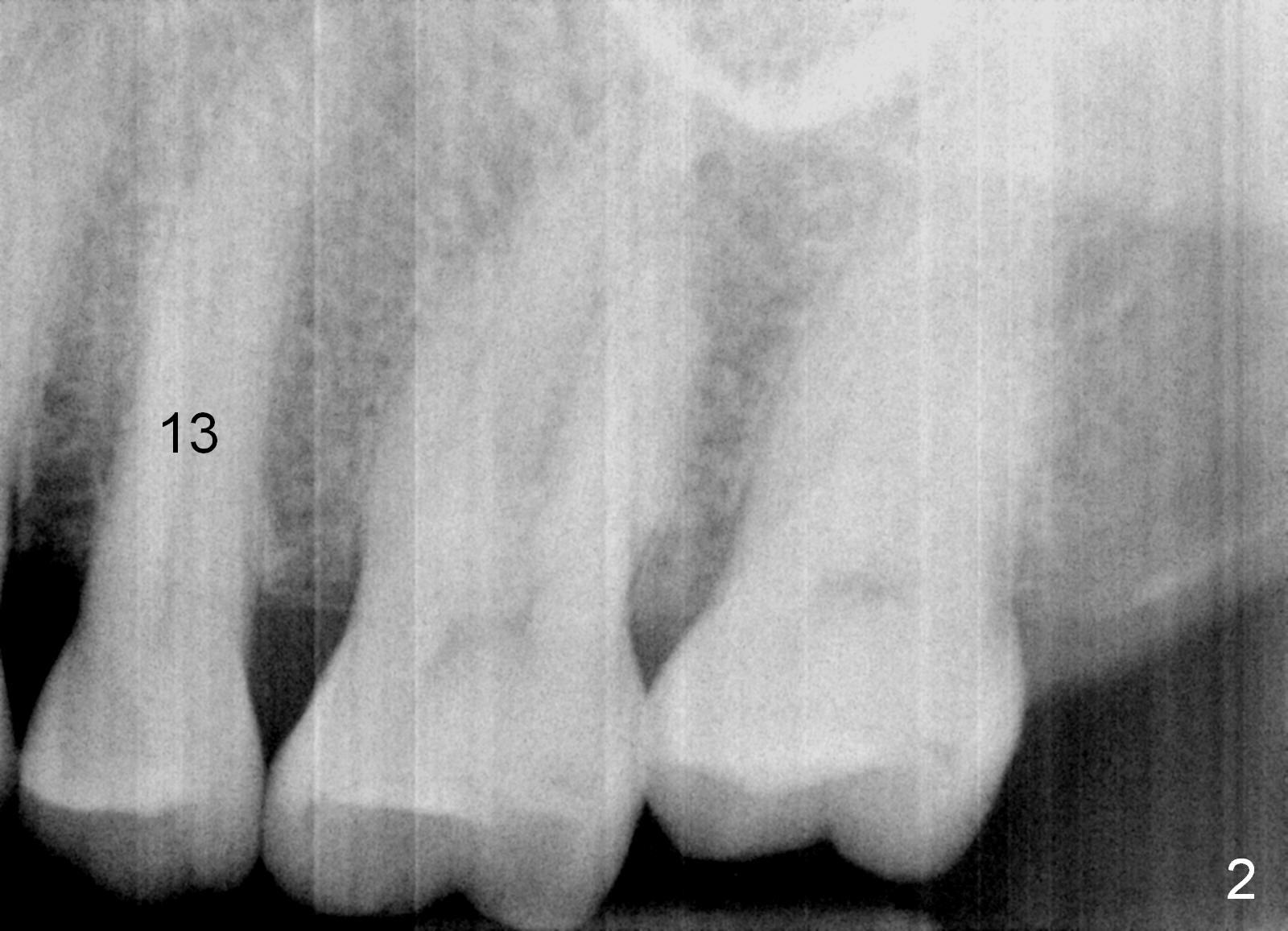
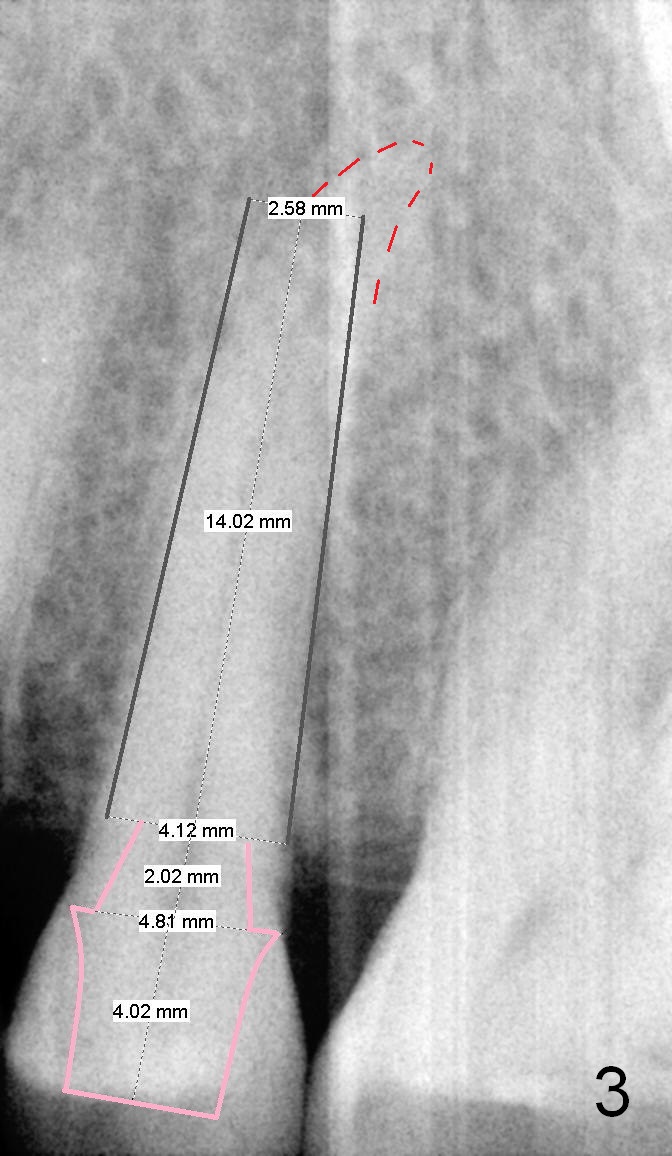
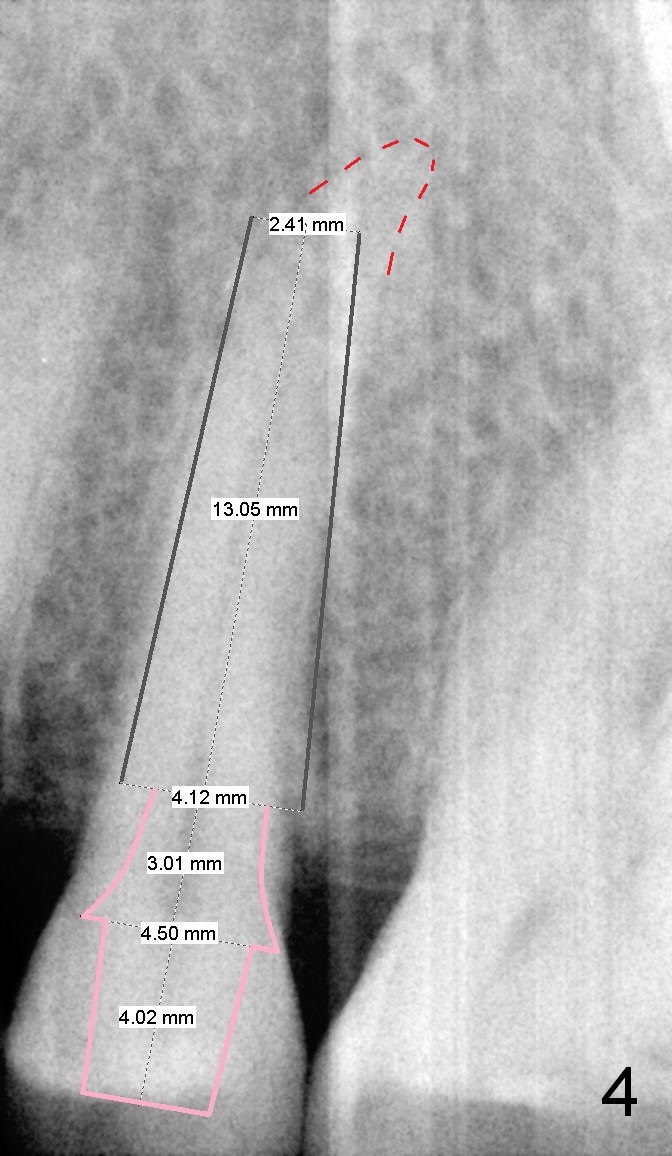
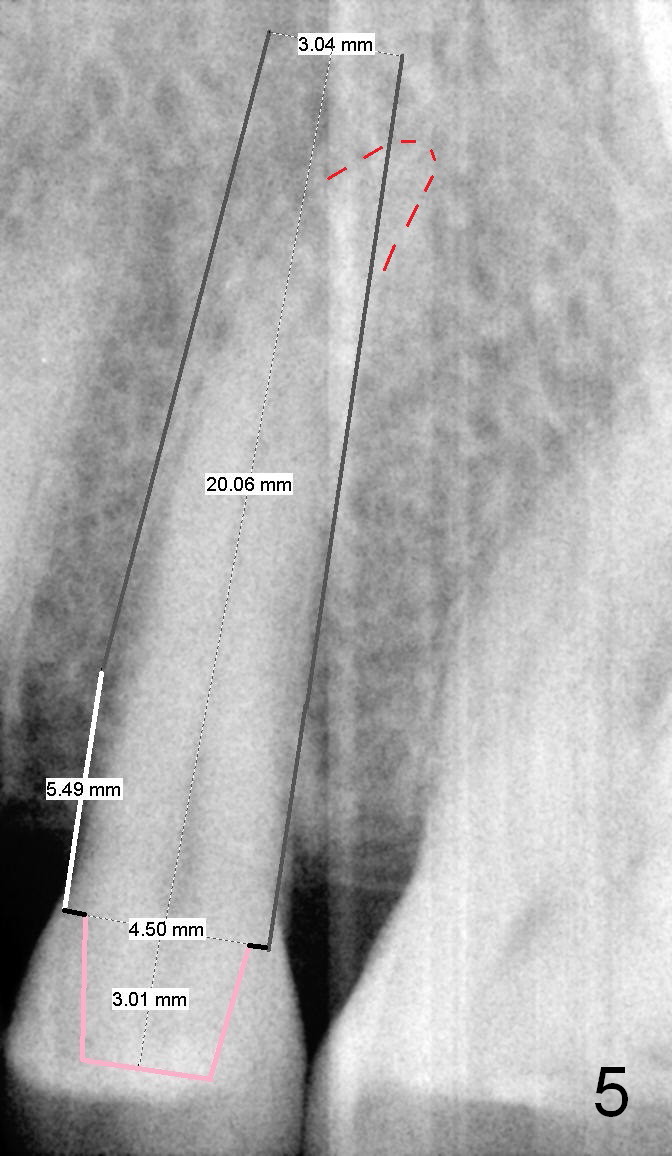
A 67-year-old lady (CC) has an implant at the site of #3, which replaces the fractured tooth (Fig.1). Recently the tooth #13 also fractures subgingivally (Fig.2). The tooth has a long and curved root. All of these suggest that the patient is a bruxer. The bone density is high. After extraction and placement of Clindamycin gauze in the socket, a 2 mm pilot drill is used to start osteotomy ~17 mm from the gingival margin, followed by 2.5 mm reamer ~ 17 mm, and 3 for 14 mm. If the socket looks small (mesiodistally), the goal is to place 4.1x14 (Fig.3) or 13 mm (Fig.4) implant. Otherwise use 4.5x17 mm Tatum tapered tap at 14 mm and plan to place a 4.5x13 or 14 mm implant. If it is difficult to insert an implant, use one size smaller drill from its original cassette or use 5x17 mm tap at 11 mm (to open up the entrance of the osteotomy). If the implant or tap is being deviated buccally while it is placed, use a Lindermann bur from Bicon Restorative plastic box to remove the bone from the palatal wall. When the side-cutting drill is cleaned, keep it in the Bicon Surgical Cassette. If the bone density turns out to be low, osteotomy depth will be 20 mm instead (Fig.5). When the flutes of 2.5 and 3 mm reamers collects bone particles, the bone density is high.
Return to Upper Premolar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 09/05/2015, last revision 01/19/2018